
Abstract
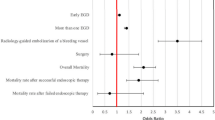
We reviewed the discharge records of all diabetic ketoacidosis hospitalizations over 30 months for the presence of clinically significant upper gastrointestinal hemorrhage. Of 284 hospitalizations in 193 patients, hemorrhage occurred in 26 hospitalizations (9%) in 25 patients (13%). None required invasive therapy to achieve hemostasis, and there were no bleeding recurrences and no deaths due to bleeding. Endoscopy in eight revealed esophagitis in all (five had erosions or ulcerations), one Mallory-Weiss tear, five with gastritis (mild in four), four with duodenitis (one erosive), one duodenal ulcer, and no gastric ulcers. Hemorrhage patients had a longer diabetes duration (14.85 vs 9.16 years,P<0.02), and more nephropathy (40% vs 11%,P<0.001), retinopathy (28% vs 12%,P<0.03) and gastroparesis (36% vs 10%,P<0.002) than those without hemorrhage. Ulcer medication (42% vs 23%,P<0.03) or anticoagulant (12% vs 1%,P<0.005) but not nonsteroidal antiinflammatory drug usage (12% vs 12%) was higher in the hemorrhage group. Admission glucose (P<0.02), BUN (P<0.04), and creatinine (P<0.02) levels were higher in hemorrhage patients, but arterial pH, serum ketones, hemoglobin, platelet count, and coagulation values were not. Hemorrhage patients required more blood transfusions (27% vs 10%,P<0.003) and intensive care unit admissions (69% vs 43%,P<0.009). Total (15% vs 3%,P<0.003) and intensive care unit mortality (22% vs 6%,P<0.026) were higher in the hemorrhage group. We conclude that upper gastrointestinal hemorrhage complicates 9% of diabetic ketoacidosis hospitalizations. Blood transfusion may be required, but the bleeding is self-limited and not severe. The most common lesion is erosive esophagitis. Hemorrhage correlates with glucose level, admission to the intensive care unit, duration of diabetes, the presence of diabetic complications, and portends a high non-bleeding-related mortality.
Similar content being viewed by others


References
Sipperstein MD: Diabetic ketoacidosis and hyperosmolar coma. Endocrin Metab Clin North Am 21:415–432, 1992
Barrett EJ, Sherwin RS: Gastrointestinal manifestations of diabetic ketoacidosis. Yale J Biol Med 56:175–178, 1983
Katz LA, Spiro HM: Gastrointestinal manifestations of diabetes. N Engl J Med 24:1350–1361, 1966
Campbell IW, Duncan LJP, Innes JA, MacCuish AC, Munro JF: Abdominal pain in diabetic metabolic decompensation, clinical significance. JAMA 233:166–168, 1975
Hirsch ML: Gastric hemorrhage in diabetic coma. Diabetes 9:94–96, 1960
Carandang NV, Schuman BM, Whitehouse FW: The gastric mucosa of patients in diabetic ketoacidosis: A gastrocamera study. Gastrointest Endosc 16:156–158, 1970
Fleckman AM: Diabetic ketoacidosis. Endocrin Metab Clin North Am 22:181–207, 1993
Wachtel TJ, Tetu-Mouradjian LM, Goldman DL, Ellis SE, O'Sullivan PS: Hyperosmolarity and acidosis in diabetes mellitus: A three-year experience in Rhode Island. J Gen Intern Med 6:495–502, 1991
Mundth ED: Cholecystitis and diabetes mellitus. N Engl J Med 267:642–646, 1962
Wright AD, Hale PJ, Singh BM, Kilvert JA, Nattrass M, FitzGerald MG: Changing sex ratio in diabetic ketoacidosis. Diabetic Med 7:628–632, 1990
Faich AG, Fishbein HA, Ellis SE: The epidemiology of diabetic acidosis: A population-based study. Am J Epidemiol 117:551–558, 1983
Ellemann K, Soerensen JN, Pedersen L, Edsberg B, Andersen OO: Epidemiology and treatment of diabetic ketoacidosis in a community population. Diabetes Care 7:528–532, 1984
Basu, A, Close CF, Jenkins D, Krentz AJ, Nattrass M, Wright AD: Persisting mortality in diabetic ketoacidosis. Diabetic Med 10:282–284, 1993
Soler NG, Bennett MA, Fitzgerald MG, Malins JM: Intensive care in the management of diabetic ketoacidosis. Lancet 1:951–954, 1973
Sheppard MC, Wright AD: The effect on mortality of low-dose insulin therapy for diabetic ketoacidosis. Diabetes Care 5:111–113, 1982
Snorgaard O, Eskildsen PC, Vadstrup S, Nerup J: Diabetic ketoacidosis in Denmark: epidemiology, incidence rates, precipitating factors and mortality rates. J Intern Med 226:223–228, 1989
Rothstein RD: Gastrointestinal motility disorders in diabetes mellitus. Am J Gastroenterol 85:782–785, 1990
Pope CE: Acid-reflux disorders. N Engl J Med 331:555–560, 1994
Dooley CP, El Newihi HM, Zeidler A, Valenzuela JE: Abnormalities of the migrating motor complex in diabeties with autonomic neuropathy and diarrhea. Scand J Gatroenterol 23:217–223, 1988
Mearin F, Camilleri M, Malagelada JR: Pyloric dysfunction in diabeties with recurrent nausea and vomiting. Gastroenterology 90:1919–1925, 1986
Stewart IM, Hosking DJ, Preston BJ, Atkinson M: Oesophageal motor changes in diabetes mellitus. Thorax 31:278–283, 1976
Keshavarzian A, Iber FL, Nasrallah S: Radionuclide esophageal emptying and manometric studies in diabetes mellitus. Am J Gastroenterol 82:625–631, 1987
Mandelstam P, Siegel CI, Lieber A, Siegel M: The swallowing disorder in patients with diabetic neuropathy-gastroenteropathy. Gastroenterology 56:1–12, 1969
Hollis JB, Castell DO, Braddom RL: Esophageal function in diabetes mellitus and its relation to peripheral neuropathy. Gastroenterology 73:1098–1102, 1977
Loo FD, Dodds WJ, Soergel KH, Arndorfer RC, Helm JF, Hogan WJ: Multipeaked esophageal peristaltic pressure waves in patients with diabetic neuropathy. Gastroenterology 88:485–491, 1985
Werth B, Meyer-Wyss B, Spinas GA, Drewe J, Beglinger C: Non-invasive assessment of gastrointestinal motility disorders in diabetic patients with and without cardiovascular signs of autonomic neuropathy. Gut 33:1199–1203, 1992
MacGregor IL, Gueller R, Watts HD, Meyer JH: The effect of acute hyperglycemia on gastric emptying in man. Gastroenterology 70:190–196, 1976
Barnett JL, Owyang C: Serum glucose concentration as a modulator of interdigestive gastric motility. Gastroenterology 94:739–744, 1988
Oster-Jorgenson E, Pedersen SA, Larsen ML: The influence of induced hyperglycaemia on gastric emptying rate in healthy humans. Scand J Clin Lab Invest 50:831–836, 1990
Fraser R, Horowitz M, Dent J: Hyperglycaemia stimulates pyloric motility in normal subjects. Gut 32:475–478, 1991
Hasler WL, Soudah HC, Dulai G, Owyang C: Mediation of hyperglycemia-evoked gastric slow-wave dysrythmias by endogenous prostaglandins. Gastroenterology 108:727–736, 1995
DeBoer SY, Maselee AAM, Lamers CBHW: Effect of hyperglycemia on gastrointestinal and gallbladder motility. Scand J Gastroenterol 27(suppl 194):13–18, 1992
Fraser RJ, Horowitz M, Maddox AF, Harding PE, Chatterton BE, Dent J: Hyperglycaemia slows gastric emptying in type 1 (insulin-dependent) diabetes mellitus. Diabetologia 33:675–680, 1990
DeBoer SY, Masclee AAM, Lam WF, Lamers CBHW: Effect of acute hyperglycemia on esophageal motility and lower esophageal sphincter pressure in humans. Gastroenterology 103:775–780, 1992
Mazze RS, Sinnock P, Deeb L, Brimberry JL: An epidemiological model for diabetes mellitus in the United States: Five major complications. Diabetes Res Clin Pract 1:185–191, 1985
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Faigel, D.O., Metz, D.C. Prevalence, etiology, and prognostic significance of upper gastrointestinal hemorrhage in diabetic ketoacidosis. Digest Dis Sci 41, 1–8 (1996). https://doi.org/10.1007/BF02208576
Received:
Revised:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF02208576