
Abstract
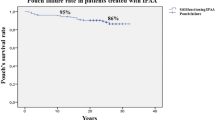
PURPOSE: Ileal pouch-anal anastomosis (IPAA) is the surgical treatment of choice for most patients with chronic ulcerative colitis. Crohn's disease is, however, a contraindication. Because distinction between UC and Crohn's disease can be difficult, some patients with Crohn's disease inadvertently undergo IPAA. The aim of this study was to determine the long-term outcome of patients with Crohn's disease who have undergone IPAA. METHODS: A total of 37 patients (20 men) were studied. Each had undergone mucosectomy with handsewn IPAA (J-pouch, n=35; S-pouch, n=1; W-pouch, n=1). Histologic examination of the resected specimen at time of IPAA showed features of ulcerative colitis (n=22), indeterminate colitis (n=9), or Crohn's disease (n=6). The stoma was closed in all patients. RESULTS: A total of 11 of 37 patients developed complex fistulas (pouch-cutaneous (n=6), pouch-vaginal (n=4), or pouch-vesical (n=1). Crohn's disease has recurred in the pouch (n=20), anal canal (n=4), pouch and anal canal (n=10), and elsewhere (n=3). After ten years (range, 3–14), the pouch remains in situ in 20 patients in whom frequency of bowel movement is seven times (3–10)/24 hours,in situ but defunctioned in seven patients, and excised in ten patients (failure rate, 45 percent). CONCLUSIONS: Inadvertent IPAA for Crohn's disease is associated with a high rate of failure (45 percent) but an acceptable long-term functional result if the pouch can be kept in situ.
Similar content being viewed by others


References
Kelly KA, Pemberton JH, Wolff BG, Dozois RR. Ileal pouch-anal anastomosis. Curr Probl Surg 1992;29:65–131.
Kohler LW, Pemberton JH, Zinsmeister AR, Kelly KA. Quality of life after proctocolectomy: a comparison of Brooke ileostomy, Kock pouch and ileal pouch-anal anastomosis. Gastroenterology 1991;101:679–84.
Hyman NH, Fazio VW, Tuckson WB, Lavery IC. Consequences of ileal pouch-anal anastomosis for Crohn's disease. Dis Colon Rectum 1991;34:653–7.
Warren BF, Shepherd NA. The role of pathology in pelvic ileal reservoir surgery. Int J Colorectal Dis 1992;7:68–75.
Pezim ME, Pemberton JH, Beart RW Jr,et al. Outcome of “indeterminant” colitis following ileal pouch-anal anastomosis. Dis Colon Rectum. 1989;32:653–8.
Wells AD, McMillan I, Price AB, Ritchie JK, Nicholls RJ. Natural history of “indeterminate” colitis. Br J Surg 1991;78:179–81.
Dozois RR, Kelly KA, Beart RW Jr, Beahrs OH. Improved results with continent ileostomy. Ann Surg 1980;192:319–24.
Handelsman JC, Gottlieb LM, Hamilton SR. Crohn's disease as a contraindication to Kock pouch. Dis Colon Rectum 1993;36:840–3.
Galandiuk S, Scott NA, Dozois RR, et al. Ileal pouch-anal anastomosis: reoperation for pouch-related complications. Ann Surg 1990;212:446–54.
Deutsch AA, McLeod RS, Cullen J, Cohen Z. Results of the pelvic-pouch procedure in patients with Crohn's disease. Dis Colon Rectum 1991;34:475–7.
Wexner SD, Rothenberger DA, Jensen L,et al. Ileal pouch vaginal fistulas: incidence, etiology and management. Dis Colon Rectum 1989;32:460–5.
Schoetz DJ Jr, Coller JA, Veidenheimer MC. Can the pouch be saved? Dis Colon Rectum 1988;31:671–5.
Nicholls RJ. Controversies and practical problem solving. In: Nicholls RJ, Bartolo D, Mortensen N, eds. Restorative proctocolectomy. London: Blackwell Scientific, 1993:53–82.
Author information
Authors and Affiliations
Additional information
Read at the meeting of the Association of Surgeons of Great Britain and Ireland, Glasgow, United Kingdom, May 22 to 24, 1996.
About this article
Cite this article
Sagar, P.M., Dozois, R.R. & Wolff, B.G. Long-term results of ileal pouch-anal anastomosis in patients with Crohn's disease. Dis Colon Rectum 39, 893–898 (1996). https://doi.org/10.1007/BF02053988
Issue Date:
DOI: https://doi.org/10.1007/BF02053988