
Abstract
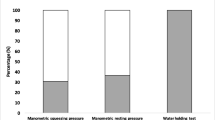
Conservation of the anal transition zone (ATZ) has been deemed necessary for continence after coloanal anastomosis (CAA) with reservoir. Therefore, we have studied functional and manometric results after CAA with reservoir and excision of the ATZ in 18 consecutive patients (mean age, 65.2 years; ten males and eight females), 17.4 months after closure of a temporary loop colostomy (Study 1). Twelve of the 18 initial patients were studied again 30.2 months after closure (Study 2). In Study 1, all patients underwent 1) a standardized interview, 2) a manometric study with measurement of anal pressure at rest (PR), voluntary contraction (VC), inhibitor anal reflex (IAR), conscious sensation (CS), and maximum tolerable volume (MTV), and 3) a liquid continence test (LCT) with measurement of colonic reservoir pressure during infusion. In Study 2, patients underwent all the same tests except the LCT. Results were compared with those of six controls (mean age, 65.8 years; two females and four males). In Study 1, 14/18 patients were continent; PR, VC, and CS did not differ among continent patients, incontinent patients, and controls. MTV was significantly lower in incontinent patients (mean ± SD, 165±46.5 ml) than in continent patients and controls (mean±SD, 261±50.8 mlvs. 250.7±83 ml). IAR was not observed in continent or incontinent patients but was observed in controls. Contraction waves in the colonic reservoir during LCT were more frequent in incontinent patients (4/4) than in continent patients (4/14), and their amplitudes were higher (119vs. 32 mm Hg). In Study 2, 12/12 patients were continent; PR and MTV remained unchanged except in the two initially incontinent patients, in whom MTV was increased. VC was slightly increased (94.7vs. 116 mm Hg). IAR remained absent in all patients. We conclude that 1) excision of the ATZ did not increase the risk of incontinence, and 2) poor functional results were mainly due to small MTV and contraction waves in the colonic reservoir.
Similar content being viewed by others


References
Williams NS. The rationale for preservation of the anal sphincter in patients with low rectal cancer. Br J Surg 1984;71:575–81.
Nicholls RJ, Lubowski DZ, Donaldson DR. Comparison of colonic reservoir and straight colo-anal reconstruction after rectal excision. Br J Surg 1988;75:318–20.
Lazorthes F, Fages P, Chiotasso P, Lemozy J, Bloom E. Resection of the rectum with construction of a colonic reservoir and colo-anal anastomosis for carcinoma of the rectum. Br J Surg 1986;73:136–8.
Parc R, Tiret E, Frileux P, Moszkowski E, Loygue J. Resection and colo-anal anastomosis with colonic reservoir for rectal carcinoma. Br J Surg 1986;73:139–41.
Keighley MR, Winslet MC, Yoshioka K, Lightwood R. Discrimination is not impaired by excision of the anal transition zone after restorative proctocolectomy. Br J Surg 1987;74:1118–21.
Martelli H, Devroede G, Arhan P, Duguay C, Dornic C, Faverdin C. Some parameters of large bowel motility in normal man. Gastroenterology 1978;75:612–8.
Read NW, Harford WN, Schmulen AC, Read MG, Santa Ana C, Fordtrand JS. A clinical study of patients with faecal incontinence and diarrhea. Gastroenterology 1979;76:747–56.
Bartolo D, Read NW, Jarratt JA, Read MG, Donnelly TC, Johnson AG. Differences in anal sphincter function and clinical presentation in patients with pelvic floor descent. Gastroenterology 1983;85:68–75.
Duthie HL, Bennett RC. The relation of the sensation in the anal canal to the functional anal sphincter: a possible factor in anal continence. Gut 1963;4:179–82.
Pedersen IB, Hint K, Olsen J, Christiansen J, Jensen P, Mortensen P. Anorectal function after low anterior resection for carcinoma. Ann Surg 1986;204:133–5.
Iwai N, Hashimoto K, Yamane T,et al. Physiologic status of the anorectum following sphincter-saving resection for carcinoma of the rectum. Dis Colon Rectum 1982;25:652–9.
Suzuki H, Matsumoto K, Amano S, Fujioka M, Honzumi M. Anorectal pressure and rectal compliance after low anterior resection. Br J Surg 1980;67:655–7.
Cortesini C. Anorectal reflex following sphinctersaving operations. Dis Colon Rectum 1980;23:320–6.
Parks AG, Porter NH, Melzak J. Experimental study of the reflex mechanism controlling the muscles of the pelvic floor. Dis Colon Rectum 1962;5:407–14.
Bennet RC, Duthie HL. The functional importance of the internal sphincter. Br J Surg 1964;51:355–7.
Heppel J, Kelly K, Philips SF, Beart R, Telander R, Perrault J. Physiologic aspects of continence after colectomy, mucosal proctectomy and endorectal ileo-anal anastomosis. Ann Surg 1982;195:435–43.
Author information
Authors and Affiliations
Additional information
Partial results of this work were read at the meeting of the British Society of Gastroenterology, Sheffield, United Kingdom, September 14 to 16, 1988.
About this article
Cite this article
Guillemot, F., Leroy, J., Boniface, M. et al. Functional assessment of coloanal anastomosis with reservoir and excision of the anal transition zone. Dis Colon Rectum 34, 967–972 (1991). https://doi.org/10.1007/BF02049959
Issue Date:
DOI: https://doi.org/10.1007/BF02049959