
Abstract
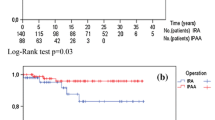
Thirty-seven patients underwent construction of a J-ileal pouch-anal anastomosis (IPAA) without temporary diverting ileostomy for chronic ulcerative colitis (CUC) (20 patients), familial adenomatous polyposis (FAP) (15 patients), indeterminate colitis (1 patient) and nonhereditary polyposis coli (1 patient) between 1981 and 1990. Seven of 20 CUC patients (35 percent) were on steroids at the time of hospital admission. The postoperative course of these patients was compared with that of a group of patients undergoing IPAA with ileostomy during that same time period and matched for age, sex, diagnosis, date of surgery, and steroid use. Eight patients (22 percent) in the group without ileostomy and four patients (11 percent) with ileostomy experienced one or more postoperative pouch-related complications. Complications requiring reoperation in patients without ileostomy occurred more frequently in patients either taking steroids or having previous pelvic radiation therapy. Functional results in patients undergoing one-stage procedures after a mean of 28 postoperative months were comparable to those in patients having staged procedures. Surgeons' criteria for a one-stage procedure in these patients should include absolute lack of tension on the anastomosis, good blood supply to the terminal ileum, good general health, and absence of recent intake of steroids at the time of surgery. We conclude that J-pouch construction with IPAA can be safely performed without diverting ileostomy, provided that these selection factors are taken into account.
Similar content being viewed by others

References
Pemberton JH, Kelly KA, Beart RW Jr, Dozois RR, Wolff BG, Ilstrup DM. Ileal pouch-anal anastomosis for chronic ulcerative colitis: long-term results. Ann Surg 1987;206:504–13.
Skarsgard ED, Atkinson KG, Bell GA, Pezim ME, Seal AM, Sharp FR. Function and quality of life results after ileal pouch surgery for chronic ulcerative colitis and familial polyposis. Am J Surg 1989;157:467–71.
Stevenson JK, Volwiler W. Ileostomy stoma complications—prevention and correction. Surg Annu 1971;3:305–22.
Feinberg SM, McLeod RS, Cohen Z. Complications of loop ileostomy. Am J Surg 1987;153:102–7.
Metcalf AM, Dozois RR, Beart RW Jr, Kelly KA, Wolff BG. Temporary ileostomy for ileal pouch-anal anastomosis: function and complications. Dis Colon Rectum 1986;29:300–3.
Rothenberger DA, Wong WD, Buls JG, Goldberg SM. The S ileal pouch-anal anastomosis. In: Dozois RR, ed. Alternatives to conventional ileostomy. Chicago: Yearbook Medical Publishers, 1985:345–66.
Thow GB. Single-stage colectomy and mucosal proctectomy with stapled antiperistaltic ileoanal reservoir. In: Dozois RR, ed. Alternatives to conventional ileostomy. Chicago: Yearbook Medical Publishers, 1985:420–32.
Metcalf AM, Dozois RR, Kelly KA, Wolff BG. Ileal pouch-anal anastomosis without temporary, diverting ileostomy. Dis Colon Rectum 1986;29:33–5.
Author information
Authors and Affiliations
Additional information
Read at the meeting of The American Society of Colon ar Rectal Surgeons, St. Louis, Missouri, April 29 to May 4, 1990.
About this article
Cite this article
Galandiuk, S., Wolff, B.G., Dozois, R.R. et al. Ileal pouch-anal anastomosis without ileostomy. Dis Colon Rectum 34, 870–873 (1991). https://doi.org/10.1007/BF02049699
Issue Date:
DOI: https://doi.org/10.1007/BF02049699