
Abstract
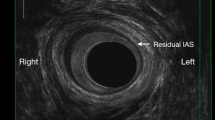
PURPOSE: The aim of lateral internal anal sphincterotomy when treating anal fissure is to divide the distal one-third to one-half of the internal anal sphincter. This study aimed to evaluate prospectively the extent of disruption to the internal anal sphincter following lateral anal internal sphincterotomy and also to establish the prevalence of symptoms of anal incontinence in these patients. METHODS: Fifteen patients with anal fissure (ten females and five males) had bowel symptoms assessed and anal endosonography performed preoperatively and two months after lateral internal anal sphincterotomy. RESULTS: Anal endosonography was normal preoperatively in all but two females who had anterior external sphincter defects (presumedly from previous obstetric trauma). Postoperatively, apart from one male in whom no defect could be identified, all had an internal anal sphincter defect corresponding to the site of lateral internal anal sphincterotomy. In nine of the ten females, the defect involved the full length of the internal anal sphincter, but in the other four males, the defect involved the distal internal anal sphincter only. All were continent preoperatively, but after lateral internal anal sphincterotomy, three females became incontinent to flatus (two of whom had a preoperative external sphincter defect). CONCLUSION: In contrast to lateral internal anal sphincterotomy in males, division of the internal anal sphincter in most females tends to be more extensive than intended. This is probably related to their shorter anal canal. In some females, lateral internal anal sphincterotomy may compromise sphincter function and precipitate anal incontinence, particularly in the presence of other sphincter defects. Care should be exercised especially in the presence of previous obstetric trauma, as internal anal sphincter division may further compromise sphincter function.
Similar content being viewed by others

References
Eisenhammer S. The surgical correction of chronic anal (sphincteric) contracture. S Afr Med J 1951;25:486–9.
Parks AG. The management of fissure-in-ano. Hosp Med 1967;1:737–43.
Hawley PR. The treatment of chronic fissure-in-ano: A trial of methods. Br J Surg 1969;56:915–8.
Notaras MJ. The treatment of anal fissure by lateral subcutaneous internal sphincterotomy-technique and results. Br J Surg 1971;58:96–100.
Abcarian H. Surgical correction of chronic anal fissure: results of lateral anal sphincterotomyvs. fissurectomy-midline sphincterotomy. Dis Colon Rectum 1980;23:31–6.
Olsen J, Mortensen PE, Krogh Petersen I, Christiansen J. Anal sphincter function after treatment of fissure-in-ano by lateral subcutaneous sphincterotomyversus anal dilatation. Int J Colorectal Dis 1987;2:155–7.
Walker WA, Rothenberger DA, Goldberg SM. Morbidity of internal sphincterotomy for anal fissure and stenosis. Dis Colon Rectum 1985;28:832–5.
Khubchandani IT, Reed JF. Sequalae of internal sphincterotomy for chronic fissure in ano. Br J Surg 1989;76:431–4.
Ravikumar TS, Sridhar S, Rao RN. Subcutaneous lateral internal sphincterotomy. Dis Colon Rectum 1982;25:798–801.
Law PJ, Bartram CI. Anal endosonography: technique and normal anatomy. Gastrointest Radiol 1989;14:349–53.
Sultan AH, Nicholls RJ, Kamm MA, Hudson CN, Beynon J, Bartram CI. Anal endosonography and correlation within vitro andin vivo anatomy. Br J Surg 1993;80:508–11.
Sultan AH, Kamm MA. Ultrasound of the anal sphincter. In: Schuster MM, ed. Atlas of gastrointestinal motility in health and disease. Baltimore: Williams and Wilkins, 1993:115–21.
Sultan AH, Kamm MA, Nicholls RJ, Hudson CN, Bartram CI. Endosonography of the anal sphincters: normal anatomy and comparison with manometry. Clin Radiol 1994;49;368–74.
Taylor BM, Beart RW Jr, Phillips SF. Longitudinal and radial variations of pressure in the human anal canal. Gastroenterology 1984;86:693–7.
Felt-Bersma RJ, Gorr G, Meuwissen SG. Normal values in anal manometry and rectal sensation: a problem of range. Hepatogastroenterology 1991;38:444–9.
Sultan AH, Kamm MA, Hudson CN, Thomas JM, Bartram CI. A prospective study of anal sphincter disruption during vaginal delivery. N Engl J Med 1993;329:1905–11.
Frezza EE, Sandei F, Leoni G, Biral M. Conservative and surgical treatment in acute and chronic anal fissure: A study of 308 patients. Int J Colorectal Dis 1992;7:188–91.
Loder PB, Kamm MA, Nicholls RJ, Phillips RK. ‘Reversible chemical sphincterotomy’ by local application of glyceryl trinitrate. Br J Surg 1994;81:1386–9.
Author information
Authors and Affiliations
Additional information
Mr. Sultan was supported by the Joint Research Board and Directorate of Obstetrics and Gynaecology, St. Bartholomew's Hospital and Mr. Kamm was supported by the St. Mark's Research Foundation.
Read at the British Society of Gastroenterology, Manchester, United Kingdom, March 25, 1993.
About this article
Cite this article
Sultan, A.H., Kamm, M.A., Nicholls, R.J. et al. Prospective study of the extent of internal anal sphincter division during lateral sphincterotomy. Dis Colon Rectum 37, 1031–1033 (1994). https://doi.org/10.1007/BF02049319
Issue Date:
DOI: https://doi.org/10.1007/BF02049319