
Abstract
Objective
To compare and contrast different heparin regimens for extracorporeal circuit anticoagulation in patients receiving acute continuous hemodiafiltration (ACHD).
Design
Prospective controlled randomized comparisons of the following regimens: 1) Low dose (500 IU/h) prefilter heparin versus regional anticoagulation in patients on continuous arteriovenous hemodiafiltration (CAVHD) via A-V shunt. 2) Low dose pre-filter heparin versus no anticoagulation in patients receiving CAVHD via femoral cannulae. 3) Low dose pre-filter heparin versus regional anticoagulation in patients on continuous veno-venous hemodiafiltration (CVVHD). 4) An assessment of the consequences of the use of no anticoagulant in patients predicted to be at high risk of hemorrhagic complications on treatment with CVVHD.
Setting
University Teaching Hospital ICU.
Patients
64 ICU patients with acute renal failure.
Measurements and main results
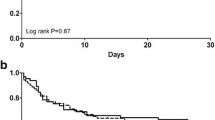
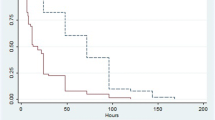
Haemofilter survival during shunt CAVHD was significantly prolonged by the use of regional anticoagulation compared to the use of low dose heparin (mean filter survival: 57.1 h versus 42.9 h;p<0.05). In CAVHD using femoral cannulae, no significant differences in haemofilter survival were found between anticoagulation with low dose heparin and the use of no anticoagulant (mean filter survival: 55 h versus 52.5 h; NS). During CVVHD, regional anticoagulation compared to low dose heparin produced a trend towards prolonged filter life which was, however, not statistically significant (mean filter survival: 40.5 h versus 31.4 h; NS). In patients assessed to be at high risk of bleeding, CVVHD without anticoagulation provided a mean filter survival of 40.9 h (95% CI 27-54.8 h).
Conclusions
Regional anticoagulation leads to longer filter survival than low dose heparin in shunt CAVHD. A regimen of no anticoagulation during femoral CAVHD leads to a filter life similar to that of low dose heparinization. During CVVHD, regional anticoagulation and low dose heparin are associated with similar filter survival times. In patients assessed to be at high risk of bleeding, treatment with CVVHD without anticoagulation results in adequate filter survival.
Similar content being viewed by others
References
Schetz M, Lanwers PM, Ferdinande P (1989) Extra-corporeal treatment of acute renal failure in the Intensive care unit: a critical view. Intensive Care Med 15:349–357
Dickson DM, Hillman KM (1990) Continuous renal replacement in the critically ill. Anaesth Intensive Care 18:76–101
Bellomo R, Ernest D, Love J, Parkin G, Boyce N (1990) Continuous arteriovenous haemodiafiltration: optimal therapy for acute renal failure in an intensive care setting? Aust NZ J Med 20:237–242
Storck M, Hartl WH, Zimmerer E, Inthorn D (1991) Comparison of pump driven and spontaneous continuous hemofiltration in postoperative acute renal failure. Lancet 337:452–455
Geronemus R, Schneider N (1984) Continuous arteriovenous hemodialysis: a new modality for treatment of acute renal failure. Trans Am Soc Intern Organs 30:610–613
Harris D (ed) (1990) Acute renal replacement — which treatment is best? Aust NZ J Med 20:197–200
Stevens PE, Davies SP, Brown EA, Riley B, Gower PE, Knox W (1988) Continuous arteriovenous haemodialysis in critically ill patients. Lancet II:150–152
Tam PY-W, Huraib S, Mahan B et al (1988) Slow continuous hemodialysis for management of complicated acute renal failure in an intensive care unit. Clin Nephrol 30:79–85
Basu D, Gallus AJ, Hirsch J, Cade J (1972) A prospective study of the value of monitoring heparin treatment with the activated partial thromboplastin time. N Engl J Med 287:324–327
Lewis SM (1987) Thromboplastin and oral anticoagulant control. Br J Hematol 66:1–4
Elms MJ (1983) Measurement of crosslinked fibrin degradation products — An immunoassay using monoclonal antibodies. Throm Haemost 50:591–594
Mehta RL, McDonald BR, Aguilar MM, Ward DM (1990) Regional citrate anticoagulation for continuous arteriovenous hemodialysis in critically ill patients. Kidney Int 38:976–981
Kaplan AA, Petrillo R (1987) Regional heparinization for continuous arteriovenous hemofiltration. Trans Am Soc Artif Intern Organs 33:312–315
Morita Y, Johnson RW, Corn RE, Hall DS (1961) Regional anticoagulation during hemodialysis using citrate. Am J Med 242:32–36
Pinnick RV, Wiegemann TB, Diedrich DA (1983) Regional citrate anticoagulation for haemodialysis in the patient at high risk of bleeding. N Engl J Med 308:258–263
Zusman RM, Rubin RH, Cato AE, Cocchetto DM, Crow JW, Tolkoff-Rubin N (1981) Hemodialysis using prostacyclin instead of heparin as the sole antithrombotic agent. N Engl J Med 304:934–939
Mehta RL, Dobos GJ, Ward DM (1992) Anticoagulation in continuous renal replacement procedures. Semin Dial 5:61–68
Schneider NS, Geronemus RP (1988) Continuous arteriovenous hemodialysis. Kidney Int 33:S159-S162
Yohay DA, Schwab SJ, Quarter LD (1990) Parallel plates are more effective than hollow fiber dialysis in continuous arteriovenous hemodialysis. J Am Soc Nephrol 1:382–386
Miller ML (1989) Heparin-induced thrombocytopenia. Cleveland Clin J Med 56:483–490
King DK, Kelton JG (1984) Heparin-associated thrombocytopenia. Ann Intern Med 100:535–540
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Bellomo, R., Teede, H. & Boyce, N. Anticoagulant regimens in acute continuous hemodiafiltration: a comparative study. Intensive Care Med 19, 329–332 (1993). https://doi.org/10.1007/BF01694706
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF01694706