
Abstract
The need for continous, noninvasive, and reliable respiratory rate monitoring during recovery from general anesthesia has long been recognized. Alternative principles can be grouped into those detecting the respiratory effort, and those detecting the actual result, i.e. the respiratory gas flow. The second category is of greatest interest for patient monitoring. In this paper, we report the development and initial clinical experience with a new acoustic air-flow sensor. By differential, multipoint detection of the air-flow in the mouth and nose region, the sensor can easily discriminate against different kinds of interference, including motion arterfacts. The sensor is nonexpensive, rugged, simple to apply, and inherently safe. An instrument with continous display of respiratory rate, and an audiovisual apnea alarm has been designed and built.
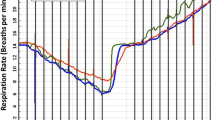
The complete system has been tested on patients during recovery after general anesthesia. In 16 patients, the respiratory rate displayed by the instrument has been correlated against that visually observed. A good correlation was obtained. Minor discrepancies can be explained from the fact that visual observation corresponds to the respiratory effort, whereas the sensor detects the actual air flow. In 12 patients, 24 hour simultaneous recordings were made of respiratory rate with the new sensor, with simultaneous recording of the oxygen saturation and the heart rate with a pulse oximeter. It was found that the new sensor reliabley recorded respiratory depression and apnea. Such events may in some patients be as frequent as one incident per hour. One case of ‘Ondine's curse’ provided clear evidence that pulse oximetry has a low sensitivity to respiratory disorders.
Similar content being viewed by others


References
Gravenstein JS. Monitoring in the post-operative period. Current Anesthesia and Critical Care 1991; 2: 32–6.
Abbott MA. Monitoring oxygen saturation levels in the early recovery phase of general anesthesia. In: Payne JP, Severinghaus JW (eds) Pulse Oximetry, Springer-Verlag, Berlin, 1986, Chapter 21, 165–71.
Tyler IL, Tantisira B, Winter PM, Motoyama EK. Continuous monitoring of arterial oxygen saturation with pulse oximetry during transfer to the recovery room. Anesth Analg 1985; 64: 1108–12.
Kataria BK, Harnik EV, Mitchard R, Kim Y, Admed S. Postoperative arterial oxygen saturation in the pediatric population during transportation. Anesth Analg 1988; 67: 280–2.
Kurth CD, LeBard SE. Association of postoperative apnea, airway obstruction, and hypoxemia in former premature infants. Anesthesiology 1991; 75: 22–6.
Møller JT, Pedersen T, Johannesen NW, Espersen K, Rasmussen L, Drylund B, Jensen PF, Rasmussen MH, Ravlo O, Chremmer-Jørgensen B, Wiberg-Jørgensen F, Cooper JB, Gravenstein JS, Johansen SH. Pulse oximetry does not reduce post-operative complications: A prospective study of 20,802 patients. Anesthesiology 1991; 75: A867.
Hök B. Microphone design for bio-acoustic signals with suppression of noise and artifacts. Sensors and Actuators 1991; A25–27: 527–33.
Wiklund L, Hök B. Monitoring of adequate ventilation in the recovery room: pulse oximetry of respiratory rate? 2nd ESCTAIC Meeting 1991 October 9–12; Goldegg, Austria, Abstract B6.
Vegfors M, Ugnell H, Hök B, Öberg PÅ, Lennmarken C.A comparison of new sensors for respiratory rate monitoring. Proc. 2nd Soc. Techn. Anesth. Meeting, 1992 Jan. 30–Feb. 1, San Diego, paper 3-4.1.
Young D, Jewkes C, Spittal M, Blogg C, Weissmann J, Gradwell D. Response time of pulse oximeters assessed using acute decompression. Anesth Analg 1992; 74: 189–95.
Scuderi P, Bowton D, Anderson R, Prough D. Pulse oximetry: would further technical alterations improve patient outcome? Anesth Analg 1992; 74: 177–80.
Lenz G, Heiprtz W, Epple E. Capnometry for contnous postoperative monitoring of nonintubated, spontaneously breathing patients. J Clin Monit 1991; 7: 245–9.
Lindberg LG, Ugnell H, Öberg Å. Monitoring of respiratory- and heart rates using a fibre optic sensor. Med Biol Eng Comput, in press.
Cyna AM, Kulkarni V, Tunstall ME, Hutchison JMS, Mallard JR. AURA: A new respiratory monitor and apnoea alarm for spontaneously breathing patients. Br J Anaesth 1991; 63: 341–5.
Shibutani K, Komatsu T, Ogawa T, Braatz TP, Tsuenekage T. Monitoring of breathing intervals in narcotic sedation. Int J Clin Monit Comput 1991; 8: 159–62.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Hök, B., Wiklund, L. & Henneberg, S. A new respiratory rate monitor: development and initial clinical experience. J Clin Monit Comput 10, 101–107 (1993). https://doi.org/10.1007/BF01142280
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF01142280