
Summary
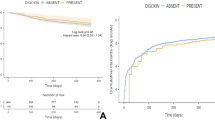
Controversy surrounds the safety of digoxin use in patients recovering from acute myocardial infarction. Previous observations yielded contradictory conclusions. To determine whether digoxin therapy is associated with increased mortality in patients recovering from acute myocardial infarction, we analyzed data from 1731 survivors of acute myocardial infarction enrolled in the Secondary Prevention Reinfarction Israeli Nifedipine Trial (SPRINT), from which patients with severe heart failure were excluded. At the time of hospital discharge, 175 patients (10%) were taking digoxin. Mortality over 1 year after infarction was significantly higher in patients treated with digoxin than in patients who were not receiving digoxin [27 of 175 (15%) vs. 60 of 1556 (4%); p<0.0001]. Digoxin administration was associated with increased mortality in several subsets of patients. Since patients treated with digoxin had baseline characteristics predictive of mortality more frequently than their counterparts, we adjusted for these differences. Multivariate analysis performed by the Cox proportional hazards model identified treatment with digoxin as an independent determinant associated with increased death during the first year after myocardial infarction [relative risk (RR) 2.8; 90% confidence interval (CI) 1.8–4.2]. Subgroup multivariate analysis indicated digoxin as an independent predictor of first year death in 464 patients who developed heart failure during their hospital stay (RR 2.3; 90% CI 1.3–4.0), as well as among 1267 patients who did not (RR 3.4; 90% CI 1.7–6.9). The present study suggests a significant excess mortality associated with digoxin therapy after myocardial infarction. The increased mortality risk may be related to unidentified variables associated with the severity of disease in patients treated with digoxin. However, our findings raise concern that the administration of digoxin may contribute to increased mortality in survivors of acute myocardial infarction.
Similar content being viewed by others


References
Yusuf S, Wittes J, Bailey K, Furberg C. Digoxin—a new controversy regarding an old drug: The pitfalls of inappropriate methods.Circulation 1986;73:14–18.
Fleiss JL, Bigger T, Rolnitzky LM. Is catch 22 alive and well and living at NHLBI? Reactions to “Digitalis—a new controversy regarding an old drug.”Circulation 1986;73:19–20.
Yusuf S, Garg R, Held P, Gorlin R. Need for a large randomized trial to evaluate the effects of digitalis on morbidity and mortality in congestive heart failure.Am J Cardiol 1992;69:64G-70G.
Maroko PR, Kjekshus JK, Sobel BE, et al. Factors influencing infarct size following experimental coronary artery occlusions.Circulation 1971;43:67–82.
Lynch JJ, Lucchessi BR. Effect of digitalis on the extent of injury and the severity of arrhythmias during acute myocardial ischemia and infarction in the dog.J Cardiovasc Pharmacol 1988;11:193–203.
Kumar R, Hood WB, Jaison J, Gilmour DP, Norman JC, Abelman WH. Efficacy and toxicity of digitalis in acute and healing phase in intact and conscious dogs.J Clin Invest 1970;43:358–364.
Iesaka Y, Kazutaka A, Gosselin A, et al. Susceptibility of infarcted canine hearts to digitalis-toxic ventricular tachycardia.J Am Coll Cardiol 1983;2:45–51.
Moss AJ, Davis HT, Conard DL, DeCamilla JJ, Odoroff CL. Digitalis-associated cardiac mortality after myocardial infarction.Circulation 1981;64:1150–1155.
Bigger AJ, Fleiss JL, Rolnitzky LA, Merab JP, Ferrick KJ. Effect of digitalis treatment on survival after acute myocardial infarction.Am J Cardiol 1985;55:623–630.
The Digitalis Subcommittee of the Multicenter Post-Infarction Research Group. The mortality risk associated with digitalis treatment after myocardial infarction.Cardiovasc Drugs Ther 1987;1:125–132.
Ryan TJ, Bailey KR, McCable CH, et al. The effects of digitalis on survival in high-risk patients with coronary artery disease.Circulation 1983;67:735–742.
Byington R, Goldstein S, for the BHAT Research Study Group. Association of digitalis therapy with mortality in survivors of acute myocardial infarction: Observations in the Beta-Blocker Heart Attack Trial.J Am Coll Cardiol 1985;6:976–982.
Madsen EB, Glipin E, Henning H, et al. Prognostic importance of digitalis after myocardial infarction.J Am Coll Cardiol 1984;3:681–689.
Muller JE, Turi ZG, Stone PH, et al. Digitalis therapy and mortality after myocardial infarction. Experience in the MILIS study.N Engl J Med 1986;314:265–271.
The Israeli Study Group. Secondary Prevention Reinfarction Israeli Nifedipine Trial (SPRINT): A randomized intervention trial of nifedipine in patients with acute myocardial infarction.Eur Heart J 1988;9:354–364.
Blackburn H. Electrocardiographic classification for population comparisons: The Minnesota code.J Electrocardiol 1969;2:5–9.
Killip T, Kimball JT. Treatment of myocardial infarction in coronary care unit: Clinical and hemodynamic profile.Am J Cardiol 1967;20:457–464.
SAS Institute Inc.SAS Technical Report P-229, SAS/STAT Software: Changes and Enhancements, release 6.07. Cary, NC: SAS Institute, Inc, 1992, 620 pp.
Mancini DM, Benotti JR, Elkayam U, et al. Antiarrhythmic drug use and serum levels of digitalis are independent adverse prognostic factors in patients with chronic heart failure (abstr).Circulation 1991;84:II243.
Akiyama T, Pawitan Y, Campbell WB, et al. Effects of advancing age on the efficacy and side effects of antiarrhythmic drugs in post-myocardial infarction patients with ventricular arrhythmias. The CAST Investigators.J Am Geriatr Soc 1992;40:666–672.
Sweeney MO, Moss AJ, Eberly S. Instantaneous cardiac death in the post hospital period after acute myocardial infarction.Am J Cardiol 1992;70:1375–1379.
The Beta-Blocker Pooling Project Research Group. The Beta-Blocker Pooling project (BBPP): Subgroup findings from randomized trials in post infarction patients.Eur Heart J 1988;9:8–16.
Molstad P, Abdelnoor M. Digitoxin-associated mortality in acute myocardial infarction.Eur Heart J 1991;2:65–69.
Schulz R, Rose J, Martin C, Brodde OE, Heusch G. Development of short-term myocardial hibernation: Its limitation by the severity of ischemia and inotropic stimulation.Circulation 1993;88:684–695.
Lee KL, Woodlief LH, Granger CB, Topol EJ, Califf RM. The risk of mortality following thrombolytic therapy is chiefly influenced by baseline clinical factors: Results from the GUSTO trial.J Am Coll Cardiol 1994;(Suppl A):29A.
Lawson MA, Davis RW, Burgard SL, Rogers WJ. Predictors of mortality at hospital discharge and at one year for patients presenting to tertiary care hospitals with myocardial infarction.J Am Coll Cardiol 1994; (Suppl A):296A.
Dfaz R, Paviotti CE, Sarmiento R, et al. Clinical and angio-graphic predischarge predictors of late mortality after acute myocardial infarction.Circulation 1993;88(Suppl):I60.
Bonaduce D, Petretta M, Arrichiello P, et al. Effects of captopril treatment on left ventricular remodeling and function after anterior myocardial infarction: Comparison with digitalis.J Am Coll Cardiol 1992;19:858–863.
The Captopril-Digoxin Multicenter Research Group. Comparative effects of therapy with captopril and digoxin in patients with mild to moderate heart failure.JAMA 1988;259:539–544.
Pfeffer MA, Braunwald E, Moye LA, et al. Effect of captopril on mortality and morbidity in patients with left ventricular dysfunction after myocardial infarction.N Engl J Med 1992;327:669–677.
Yusuf S, Pepine CJ, Garces C, et al. Effect of enalapril on myocardial infarction and unstable angina in patients with low ejection fraction.Lancet 1992;340:1173–1178.
Author information
Authors and Affiliations
Consortia
Rights and permissions
About this article
Cite this article
Leor, J., Goldbourt, U., Behar, S. et al. Digoxin and mortality in survivors of acute myocardial infarction: Observations in patients at low and intermediate risk. Cardiovasc Drug Ther 9, 609–617 (1995). https://doi.org/10.1007/BF00878094
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF00878094