
Abstract
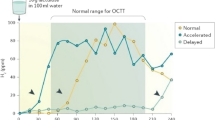
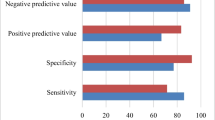
To date, there is no general agreement as to which test is to be preferred for the diagnosis of small-intestinal bacterial overgrowth. The 1-g carbon-14d-xylose breath test has been proposed as a very sensitive and specific test for the diagnosis of bacterial overgrowth. However, in patients with severe gastrointestinal motor dysfunction, the lack of consistent delivery of14C-d-xylose to the region of bacterial contamination may result in a “negative” result. The aim of this study was to determine whether the accuracy of14C-d-xylose breath test for detecting bacterial overgrowth can be increased by correction with the gastric emptying rate of14C-d-xylose. Ten culture-positive patients and ten culture-negative controls were included in the study. Small-intestinal aspirates for bacteriological culture were obtained endoscopically. A liquid-phase gastric emptying study was performed simultaneously to assess the amount of14C-d-xylose that entered the small intestine. The results of the percentage of expired14CO2 at 30 min were corrected with the amount of14C-d-xylose that entered the small intestine. There were six patients in the culture-positive group with a14CO2 concentration above the normal limit. Three out of four patients with initially negative results using the uncorrected method proved to be positive after correction. All these three patients had prolonged gastric emptying of14C-d-xylose. When compared with cultures of small-intestine aspirates, the sensitivity and specificity of the uncorrected14C-d-xylose breath test were 60% and 90%, respectively. In contrast, the sensitivity and specificity of the corrected14C-d-xylose breath test improved to 90% and 100%, respectively. In conclusion, using the gastric emptying rate of14C-d-xylose as a correcting factor, we found a higher sensitivity and specificity for the14C-d-xylose breath test in the detection of small-intestinal bacterial overgrowth than were achieved with the conventional method.
Similar content being viewed by others

References
Sarker SA, Gyr K. Non-immunological defense mechanisms of the gut.Gut 1992; 33: 987–993.
Schuffler MD. Diagnosis and treatment of chronic idiopathic intestinal pseudo-obstruction syndromes.Surv Dig Dis 1984; 2: 104.
Sherman PM. Bacterial overgrowth. In: Yamada T, ed.Textbook of gastroenterology. Philadelphia: J.B. Lippincott; 1991: 1520–1540.
Kerlin P, Wong L. Breath hydrogen testing in bacterial overgrowth of the small intestine.Gastroenterology 1988; 95: 982–988.
Corazza GR, Menozzi MG, Strocchi A, Rasciti L, Varia D, Lecchini R, Avanzini P, Chezzi C, Gasbarrini G. The diagnosis of small bowel bacterial overgrowth. Reliability of jejunal culture and inadequacy of breath testing.Gastroenterology 1990; 98: 302–309.
Craig RM, Atkinson AJ.d-Xylose testing; a review.Gastroenterology 1988; 95: 223–231.
King CE, Toskes PP, Spivey JC, Lorenz E, Welkos S. Detection of small intestine bacterial overgrowth by means of a C14 D-Xylose breath test.Gastroenterology 1979; 77: 75–82.
King CE, Toskes PP, Guilarte TR, Lorenz E, Welkos SL. Comparison of the one-gramd-[14C]xylose breath test to the [14C]bile acid breath test in patients with small-intestinal bacterial overgrowth.Dig Dis Sci 1980; 25: 53–58.
King CE, Toskes PP. Comparison of the 1-gram [14C]xylose, 10-gram lactulose-H2, and 80-gram glucose-H2 breath tests in patients with small intestine bacterial overgrowth.Gastroenterology 1986; 91: 1447–1451.
Schneider A, Novis B, Chen V, Leichtman G. Value of the14C-d-xylose breath test in the patients with intestinal bacterial overgrowth.Digestion 1985; 32: 86–91,
Valdovinos MA, Camilleri M, Thomforde GM, Frie C. Reduced accuracy of14C-d-xylose breath test for detecting bacterial overgrowth in gastrointestinal motility disorders.Scand J Gastroenterol 1993; 28: 963–968.
Vantrappen G, Jassens J, Hellemans J, Ghoos Y. The interdigestive motor complex of normal subjects and patients with bacterial overgrowth of the small intestine.J Clin Invest 1977; 59: 1158–1166.
Kim CH, Kennedy FP, Camilleri M, Zinsmeister AR, Ballard DJ. The relationship between clinical factors and gastrointestinal dysmotility in diabetes mellitus.J Gastrointest Mot 1991; 3: 268–272.
Soudah HC, Hasler WL, Owyang C. Effect of octreotide on intestinal motility and bacterial overgrowth in scleroderma.N Engl J Med 1991; 325: 1461–1467.
Chesta J, Defilippi C, Defilippi C. Abnormalities in proximal small bowel motility in patients with cirrhosis.Hepatology 1993; 17: 828–832.
Ealdron B, Cullen PT, Kumar R, Smith D, Tankowski J, Hopwood D, Sutton D, Kennedy N, Campbell FC. Evidence for hypomotility in non-ulcer dyspepsia: a prospective mutifactorial study.Gut 1991; 32: 246–251.
umessen JJ, Gudmand-Hoyer E, Bachmann E, Justesen T. Diagnosis of bacterial overgrowth of the small intestine. Comparison of the14C-d-xylose breath test and jejunal culture in 60 patients.Scand J Gastroenterol 1985; 20: 1267–1275.
O'Connor MP, Healy M, Keheley A, Keane CT, O'Moore RR, Weir DG. H2 or14C-breath tests in the disgnosis of small intestinal bacterial overgrowth?Gastroenterology 1987; 92: 1557.
Rumessen JJ. [14C]d-xylose breath test for small intestinal bacterial overgrowth.Gastroenterology 1989; 96: 273–274.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Chang, CS., Chen, GH., Kao, CH. et al. Increased accuracy of the carbon-14d-xylose breath test in detecting small-intestinal bacterial overgrowth by correction with the gastric emptying rate. Eur J Nucl Med 22, 1118–1122 (1995). https://doi.org/10.1007/BF00800592
Received:
Revised:
Issue Date:
DOI: https://doi.org/10.1007/BF00800592