
Abstract
Adrenal venous blood samples drawn before and after stimulation with adrenocorticotropic hormone (ACTH) were analysed in 32 consecutive patients with primary aldosteronism. Twenty-six patients had aldosterone-producing adenomas and six patients had bilateral hyperplasia.
The ratio of higher to lower levels of aldosterone in the right and left adrenals (aldosterone ratio), aldosterone to cortisol ratio (A/C ratio), and the ratio of higher to lower levels of A/C ratio in the right and left adrenals (ratio of A/C ratios) were calculated. We used both aldosterone ratio and ratio of A/C ratios as a means of diagnosis, a ratio of 3.0 or more for unilateral adenoma, and less than 3.0 for bilateral hyperplasia. With ACTH stimulation, correct characterization of lesions increased from 91% (29 of 32) to 97% (31 of 32) by aldosterone ratio and from 84% (27 of 32) to 97% (30 of 31) by ratio of A/C ratios. Correct diagnosis of bilateral hyperplasia increased markedly from 67% (4 of 6) to 100% and 50% (3 of 6) to 83% (5 of 6) with use of each criterion.
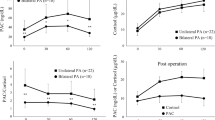
In patients with adenoma, aldosterone ratio rose in 54% (14 of 26) from the pre-stimulation levels. Before stimulation, it ranged from 1.5 to 115.9 (mean 34.8), and afterwards, from 2.1 to 1097.9 (mean 95.5). In contrast, in all patients with bilateral hyperplasia aldosterone ratio fell to less than 3.0 following stimulation with ACTH. With ACTH stimulation, aldosterone ratio increased in patients with adenoma and decreased in patients with hyperplasia.
Measurement of A/C ratio is used to ensure correct access to the adrenal veins, but it was useful in only one case and aldosterone ration was a more reliable diagnostic parameter than ratio of A/C ratios in both pre-and post-ACTH stimulations.
Assay of aldosterone levels and calculation of aldosterone ratios before and after ACTH stimulation were valuable in locating small adenomas in the right and left adrenal and especially in differentiating bilateral hyperplasia from adenoma.
Similar content being viewed by others


References
Conn JW, Cohen EL, Rovner DR (1964) Suppression of plasma renin activity in primary aldosteronism: Distinguishing primary from secondary aldosteronism in hypertensive disease. JAMA 190: 213–221
Davis WW, Newsome HH, Wright LD, Hammond WG, Easton J, Bartter FC (1967) Bilateral adrenal hyperplasia as a cause of primary aldosteronism with hypertension, hypokalemia and suppressed renin activity. Am J Med 42: 642–647
Katz FH (1967) Primary aldosteronism with suppressed plasma renin activity due to bilateral nodular adrenocortical hyperplasia. Ann Intern Med 67: 1035–1042
Biglieri EG, Stockigt JR, Schambelan M (1972) Adrenal mineralocorticoids causing hypertension. Am J Med 52: 623–632
White EA, Schambelan M, Rost CR, Biglieri EG, Moss AA, Korobkin M (1980) Use of computed tomography in diagnosing the cause of primary aldosteronism. N Eng J Med 303: 1503–1507
Dunnick NR, Doppman JL, Gill JR, Strott CA, Keiser, HR, Brennan MF (1982) Localization of functional adrenal tumors by computed tomography and venous sampling. Radiology 142: 429–433
Geisinger MA, Zelch MG, Bravo EL, Risius BF, O'Donovan PB, Borkowski GP (1983) Primary hyperaldosteronism: Comparison of CT, adrenal venography, and venous sampling. AJR 141: 299–302
Ikeda DM, Francis IR, Glazer GM, Amendola MA, Gross MD, Aisen AM (1989) The detection of adrenal tumors and hyperplasia inpatients with primary aldosteronism: Comparison of scintigraphy, CT, and MR imaging. AJR 153: 301–306
Dunnick NR (1990) Adrenal imaging: Current status. AJR 154: 927–936
Baker ME, Blinder R, Spritzer C, Leight GS, Herfkens RJ, Dunnick NR (1989) MR evaluation of adrenal masses at 1.5T. AJR 153: 307–312
Remer EM, Weinfeld RM, Glazer GM et al. (1989) Hyperfunctioning and nonhyperfunctioning benign adrenal cortical lesions: Characterization and comparison with MR imaging. Radiology 171: 681–685
Melby JC, Spark RF, Dale SL, Egdahl RH, Kahn PC (1967) Diagnosis and localization of aldosterone-producing adenomas by adrenal-vein catheterization. N Eng J Med 277: 1050–1056
Horton R, Finck E (1972) Diagnosis and localization in primary aldosteronism. Ann Int Med 76: 885–890
Weinberger MH, Grim CE, Hollifield JW et al. (1979) Primary aldosteronism: Diagnosis, localization, and treatment. Ann Int Med 90: 386–395
Dunnick NR, Doppman JL, Mills SR, Gill JR (1979) Preoperative diagnosis and localization of aldosteronomas by measurement of corticosteroids in adrenal venous blood. Radiology 133: 331–333
Vaughan NJA, Jowett TP, Slater JDH et al. (1981) The diagnosis of primary hyperaldosteronism. Lancet I: 120–125
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Tokunaga, K., Nakamura, H., Marukawa, T. et al. Adrenal venous sampling analysis of primary aldosteronism: value of ACTH stimulation in the differentiation of adenoma and hyperplasia. Eur. Radiol. 2, 223–229 (1992). https://doi.org/10.1007/BF00595834
Issue Date:
DOI: https://doi.org/10.1007/BF00595834