
Summary
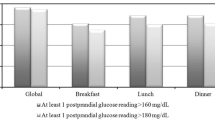
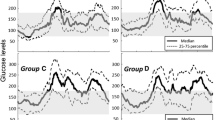
The European NIDDM Policy Group states that the lowest target for good control of Type 2 (non-insulin-dependent) diabetic patients is a blood glucose level 4.4 mmol/l, both fasting and postprandially. The aim of this study is to evaluate the occurrence and temporal distribution of values under this target in the clinical records of 463 Type 2 diabetic patients, treated by diet or diet and oral hypoglycaemic agents, monitored for at least 2 years. The protocol includes blood glucose measurements after overnight fasting (08.00 hours), 120–150 min after breakfast (11.00 hours) and 120 and 240 min after lunch (14.00 and 16.00 hours). At least one blood glucose concentration of less than 4.4 mmol/l was presented by 42% of the patients. The only difference between patients showing and not showing glycaemic levels under this target was the higher percentage on oral hypoglycaemic agents in the first group (68.4% vs 56.9%, p=0.016). We considered 299 blood glucose profiles containing at least one value of less than 4.4 mmol/l, observing that a) 46.9% of profiles from patients treated by diet alone and 68.7% of profiles from patients treated both by diet and oral hypoglycaemic agents presented the lowest blood glucose concentration at 16.00 hours (p=0.002). b) No correlation existed between fasting blood glucose and values at 16.00 hours in profiles from diet-treated patients, whereas a negative correlation was present in patients on diet and oral hypoglycaemic agents, indicating that an excess of oral agents, administered to correct fasting hyperglycaemia. was the cause of the low glycaemic values in the afternoon. c) 37.9% of profiles on a diet and 83.3% of profiles on diet and oral agents showed fasting glucose concentrations >6.7 mmol/l, the upper limit of good control according to the European NIDDM Policy Group. This indicates that fasting hyperglycaemia does not exclude the occurrence of low glucose values throughout the day and that it is necessary to monitor blood glucose profiles.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Alberti KGMM, Gries FA (1988) Management of non-insulin- dependent diabetes mellitus in Europe: a consensus view. Diab Med 5: 275–281
De Feo P, Gallai V, Mazzotta G et al. (1988) Modest decrements in plasma glucose concentration cause early impairment in cognitive function and later activation of glucose counterregulation in the absence of hypoglycaemic symptoms in normal man. J Clin Invest 82: 436–444
Hilsted J, Bonde-Petersen F, Norgaard MB, Greniam M, Christiansen NJ, Parving HH, Suzuki M (1984) Haemodynamic changes in insulin-induced hypoglycaemia in man. Diabetologia 26: 328–332
Fisher BM, Baylis PH, Frier BM (1987) Plasma oxytocin, arginine vasopressin and atrial natriuretic peptide responses to insulin-induced hypoglycaemia in man. Clin Endocrinol 26: 179–185
Trovati M, Anfossi G, Cavalot F et al. (1986) Studies on mechanisms involved in hypoglycaemia-induced platelet activation. Diabetes 35: 818–825
Trovati M, Massucco P, Mularoni E, Cavalot F, Anfossi G, Mattiello L, Emanuelli G (1988) Insulin-induced hypoglycaemia increases plasma concentrations of angiotensin II and does not modify atrial natriuretic polypeptide secretion in man. Diabetologia 31: 816–820
Kishikawa H, Takeda H, Kiyota S et al. (1987) Role of α 2-adrenergic receptor in platelet activation during insulin-induced hypoglycaemia in normal subjects. Diabetes 36: 407–412
Takeda H, Kishikawa H, Shinohara M et al. (1988) Effect of α 2-adrenoceptor antagonist on platelet activation during insulininduced hypoglycaemia in Type 2 (non-insulin-dependent) diabetes mellitus. Diabetologia 31: 657–663
Frier BM, Hilsted J (1985) Does hypoglycaemia aggravate the complications of diabetes? Lancet II: 1175–1177
Ferner RE, Neil H (1988) Sulphonylureas and hypoglycaemia. Br Med J 296: 949–950
National Diabetes Data Group (1979) Classification and diagnosis of diabetes mellitus and other categories of glucose intolerance. Diabetes 28: 1039–1057
Foster DW (1991) Diabetes Mellitus. In: Wilson JD, Braunwald E, Isselbacher KJ, Petersdorf RG, Martin JB, Fauci AS, Root RK (eds) Harrison's principles of internal medicine, 12th edn. Mc Graw Hill, New York, pp 1739–1759
Thai AC, Ng WF, Lui KF, Yeo PPB (1989) Three new glucose reflectance meters Diascan, Glucometer II, and Reflolux II. Diab Res Clin Pract 7: 75–81
Glantz SA (1987) Primer of Biostatistics. Mc Graw Hill. New York
Jennings AM, Wilson RM, Ward JD (1989) Symptomatic hypoglycaemia in NIDDM patients treated with oral hypoglycaemic agents. Diab Care 12: 203–208
Matsuda A, Kuzuya T, Sugita Y, Kawashima K (1983) Plasma levels of glibenclamide in diabetic patients during its routine clinical administration determined by specific radioimmunoassay. Horm Metab Res 15: 425–428
Balant L, Zahnd GR, Weber F, Fabrie J (1977) Behaviour of glibenclamide on repeated administration to diabetic patients. Eur J Clin Pharmacol 11: 19–25
Holman RR, Turner RC (1988) Optimizing blood glucose control in Type 2 diabetes: an approach based on fasting blood glucose measurements. Diab Med 5: 582–588
Tattersall RB (1984) Diabetes in the elderly ⊕ neglected area? Diabetologia 27: 167–173
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Trovati, M., Burzacca, S., Mularoni, E. et al. Occurrence of low blood glucose concentrations during the afternoon in Type 2 (non-insulin-dependent) diabetic patients on oral hypoglycaemic agents: importance of blood glucose monitoring. Diabetologia 34, 662–667 (1991). https://doi.org/10.1007/BF00400996
Received:
Revised:
Issue Date:
DOI: https://doi.org/10.1007/BF00400996