
Summary
The hospital prevalence rate for upper gastrointestinal ulcerative disease in 28,531 inpatients consecutively admitted in two teaching hospitals in the Comprehensive Hospital Drug Monitoring (CHDM) in Berne, from 1974 to 1985, was 2.2% (1.8% for gastric or duodenal ulcer, and 0.4% for erosive gastritis). This was based on the evaluation of 634 patients after exclusion of the subgroup of patients with hepatic cirrhosis or upper gastrointestinal neoplasia.
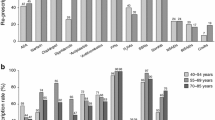
After exclusion of patients on anticoagulant therapy (n=73), 561 (=100%) patients could be further studied. Of them, 33.3% (n=187) were found to have been exposed to non-steroidal anti-inflammatory drugs (NSAIDs), including aspirin, within 21 days prior to confirmation of the diagnosis.
The observed relative risk (RR) of developing a substantial acute upper gastrointestinal bleeding (Hb < 10 g/100 ml for men, and <9 g/100 ml for women, or a decrease in Hb of more than 25%) was 1.61 when patients exposed to NSAIDs (n=187) were compared to patients not exposed to those drugs (n=374). Although there was no significant sex difference overall, the RR for gastrointestinal bleeding differed considerably in the various age-groups; it was elevated in men under 40 years (RR=2.86) and in women over 60 years of age (RR=1.89), as compared to the mean RR of 1.61.
Similar content being viewed by others


Abbreviations
- CHDM:
-
Comprehensive Hospital Drug Monitoring
- GIB:
-
acute upper gastrointestinal bleeding
- ICD:
-
International Classification of Diseases, 9 revision
- NSAID:
-
non-steroidal anti-inflammatory drug
- RR:
-
relative risk
References
Carson JL, Strom BL, Soper KA, West SL, Morse ML (1987) The Association of nonsteroidal anti-inflammatory drugs with upper gastrointestinal tract bleeding. Arch Intern Med 147: 85–89
Coggon D, Lambert P, Langman MJS (1981) 20 years of hospital admissions for peptic ulcer in England and Wales. Lancet I: 1302–1304
Coggon D, Langman MJS, Spiegelhalter D (1982) Aspirin, paracetamol, and haematemesis and melaena. Gut 23: 340–344
Conn HO, Blitzer BL (1979) Nonassociation of adrenocorticosteroid therapy and peptic ulcer. N Engl J Med 294: 473–479
Duggan JM, Dobson AJ, Johnson H, Fahey P (1986) Peptic ulcer and non-steroidal anti-inflammatory agents. Gut 27: 929–933
Elashoff JD, Grossman MI (1980) Trends in hospital admissions and death rates for peptic ulcer in the united states from 1970 to 1978. Gastroenterology 78: 280–285
Eliakim R, Ophir M, Rachmilewitz D (1987) Duodenal mucosal injury with nonsteroidal antiinflammatory drugs. J Clin Gastroenterol 9: 395–399
Fleiss JL (1973) Statistical methods for rates and proportions. John Wiley and Sons, New York
Guess HA, West R, Strand LM, Helston D, Lydick EG, Bergman U, Wolski K (1988) Fatal upper gastrointestinal hemorrhage or perforation among users and nonusers of nonsteroidal anti-inflammatory drugs in Saskatchewan, Canada 1983. J Clin Epidemiol 41: 35–45
Guslandi M (1988) How does smoking harm the duodenum? Br Med J 296: 311
Haefeli AM (1986) Beeinflussung der Häufigkeit akuter oberer gastrointestinaler Blutungen durch nicht-steroidale Antirheumatika bei Patienten mit peptischen Läsionen im gastro-duodenalen Bereich — Eine retrospektive Studie an 145 Fällen. Inaugural-Dissertation, Medizinische Fakultät der Universität Bern
Harrison A, Elashoff J, Grossman MI (1979) Peptic ulcer disease in “Smoking and Health, a report of the Surgeon General (prepared by Agencies of the U.S. Department of Health, Education and welfare/National Institute of Arthritis, Metabolism, and Digestive Diseases)” pp 9–21
Hoigné R, Hottinger S (1988) Monitoring adverse drug reactions in the postmarketing phase. Pharm Acta Helv 1: 2–12
Ivey KJ, Silvoso GR, Kruase WJ (1978) Effect of paracetamol on gastric mucosa. Br Med J 1: 1586–1588
Jick H (1981) Effects of Aspirin and Acetaminophen in gastrointestinal hemorrhage. Arch Intern Med 141: 316–321
Jick SS, Perera DR, Walker AM, Jick H (1987) Non-steroidal anti-inflammatory drugs and hospital admission for perforated peptic ulcer. Lancet II: 380–382
Kikendall JW, Evaul J, Johnson LF (1984) Effect of cigarette smoking on gastrointestinal physiology and non-neoplastic digestive disease. J Clin Gastroenterol 6: 65–78
Kurata JH, Haile BM, Elashoff JD (1985) Sex differences in peptic ulcer disease. Gastroenterology 88: 96–100
Langman MJS (1986) Anti-inflammatory drug intake and the risk of ulcer complications. Med Toxicol 1 [Suppl 1]: 34–38
Langman MJS (1987) The changing face of peptic ulceration. Scand J Gastroenterol 136: 37–40
Levy M (1974) Aspirin use in patients with major upper gastrointestinal bleeding and peptic-ulcer disease. N Engl J Med 290: 1158–1162
McCarthy DM (1984) Smoking and ulcers — time to quit. N Engl J Med 311: 726–728
Messer J, Reitman D, Sacks HS, Smith H, Chalmers T (1983) Association of adrenocorticosteroid therapy and peptic-ulcer disease. N Engl J Med 309: 21–24
Negre J (1985) Perforated ulcer in elderly people. Lancet II: 1118–1119
Piper DW, McIntosh JH, Ariotti DE, Fenton BH, Mac Lennan RM (1981) Analgesic ingestion and chronic peptic ulcer. Gastroenterology 80: 427–432
Scott JT, Porter IH, Lewis SM, Dixon StJ (1961) Studies of gastrointestinal bleeding caused by corticosteroids, salicylates and other analgesics. Q J Med XXX (NS) 118: 167–188
Singer MV (1986) Bewirken reiner Alkohol und alkoholische Getränke beim Menschen eine Stimulation der Magensäuresekretion und eine Freisetzung von Gastrin? Dtsch Med Wochenschr 111: 749–752
Somerville K, Faulkner G, Langman M (1986) Non-steroidal anti-inflammatory drugs and bleeding peptic ulcer. Lancet i: 462–464
Sonnenberg A, Fritsch A (1983) Changing mortality of peptic ulcer disease in Germany. Gastroenterology 84: 1553–1557
Walt R, Logan R, Katschinski B, Ashley J (1986) Rising frequency of ulcer perforation in elderly people in the United Kingdom. Lancet I: 489–492
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Stodolnik, E., Maurer, P., Hoigné, R. et al. Risk of acute upper gastrointestinal bleeding in patients with ulcerative disease and treatment with non-steroidal anti-inflammatory drugs (NSAIDs). Eur J Clin Pharmacol 38, 31–35 (1990). https://doi.org/10.1007/BF00314799
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF00314799