
Summary
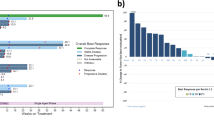
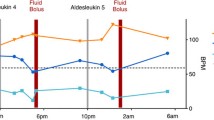
The combined administration of subcutaneous recombinant human interleukin-2 (rIL-2) and interferon-α (rIFN-α) was studied in a phase II trial on patients with advanced progressive renal cell cancer. Safety, tolerance and clinical response rate of this outpatient treatment protocol were assessed in 29 evaluable patients who received a total of 47 cycles, each consisting of s.c. rIL-2 at 14.4–18 million IU m−2day−1 on days 1 and 2, followed by 6 weeks of combined administration of s.c. rIL-2 at 3.6–4.8 million IU m−2 day−1 on 5 days a week, and s.c. rIFN-α at 3–6 million units m−2 three times weekly over a period of 6 consecutive weeks. In patients exhibiting stable or regressive disease upon combined IL-2 and rIFN-α, the therapy was continued. The overall response rate was 31% (95% confidence limits = 15%–51%), with 6 out of 29 patients achieving partial remission (PR, 21%) and 3 patients complete remission (CR, 10%). In addition, 12 patients presented with stable disease. The median duration of response was 8.5 months in PR and 19+ months in CR. Long-term treatment using this regimen was associated mainly with moderate (WHO grade I–II) toxicity including fevers, chills, malaise, nausea and/or vomiting, anorexia and transient local inflammation at the injection sites. No toxic deaths occurred. Altered thyroid function was observed in more than half the patients. The combination regimen resulted in a significant increase in peripheral blood eosinophils and natural killer cells (P<0.005). Up-on treatment, 14 patients developed non-neutralizing activity against rIL-2, and 2 of these developed specific neutralizing antibodies after consecutive cycles; no anti-rIFN-2b antibodies were detected. In summary, subcutaneous long-term outpatient treatment with low-dose rIL-2 and rIFN-α is feasible, with moderate toxicity, and results in an objective tumor response rate comparable to that obtained previously with high-dose rIL-2 i.v. regimens.
Similar content being viewed by others

References
Atkins MB, Mier JW, Parkinson DR, Gould JA, Berkman EM, Kaplan MM (1988) Hypothyroidism after treatment with interleukin-2 and lymphokine-activated killer cells. N Engl J Med 318:1557–1563
Atzpodien J, Shimazaki C, Wisniewski D, Gulati S, Bührer C, Öz S, Link H, Poliwoda H, Welte K, Clarkson B (1988) Interleukin-2 und Interferon-α in der adoptiven Immuntherapie Plasmozytoms: Ein experimentelles Modell. In: Lutz D, Heinz R, Nowotny H, Stacher A (eds) Leukämien und Lymphome. Munich, Vienna, Baltimore. Urban and Schwarzenberg, pp 211–212
Atzpodien J, Körfer A, Evers P, Franks CR, Knüver-Hopf J, Lopez-Hänninen E, Fischer M, Mohr H, Benter T, Hadam M, Poliwoda H, Kirchner H (1990) Low dose subcutaneous recombinant interleukin-2 in advanced human malignancy: a phase II outpatient study. Mol Biother 2:18–26
Aulitzky W, Gastl G, Aulitzky WE, Herold M, Kemmler J, Mull B, Frick J, Huber Ch (1990) Successful treatment of metastatic renal cell carcinoma with a biologically active dose of recombinant interferon-gamma. J Clin Oncol 7:1875–1884
Brunda MJ, Bellenton D, Sulich V (1987) In vitro and in vivo interactions of recombinant interferon alpha and interleukin-2 antitumor activity and induction of cytotoxic effector cells. Int J Cancer 40:365–371
Bukowski RM, Osgood B, Sergi J, Budd GT, Finke J, Medendorp S, Tubbs R, Montie J, Pontes E (1988) Phase IA/IB trial of interleukin-2 and interferon-alpha results in metastatic renal cell carcinoma. J Urol 139 [Suppl]:283
Buzaid AC, Todd MB (1989) Therapeutic options in renal cell carcinoma. Semin Oncol 16:12–19
Eberlein TJ, Schoof DD, Jung SE, Davidson D, Gramolini B, McGrath K, Massaro A, Wilson RE (1988) A new regimen of interleukin-2 and lymphokine-activated killer cells. Efficacy without significant toxicity. Arch Intern Med 148:2571–2576
Engvall E, Perlman P (1971) Enzyme-linked immunosorbent assay (ELISA). Quantitative assay of immunoglobulin G. Immunochemistry 8:871–874
Gillis S, Ferm MM, Ou W (1978) T cell growth factor: parameters of production and a quantitative microassay for activity. J Immunol 120:2027–2032
Hirsh M, Lipton A, Harvey H, Givant E, Hopper K, Jones G, Zeffren J, Levitt D (1990) Phase I study of interleukin-2 and interferon-α2a as outpatient therapy for patients with advanced malignancy. J Clin Oncol 8:1657–1963
Kirchner H, Körfer A, Franks CR, Evers P, Dallmann I, Goldmann U, Poliwoda H, Atzpodien J (1990) Thyroid dysfunction upon subcutaneous recombinant interleukin-2 with and without interferon-α2b in patients with advanced progressive malignancy. Proc Am Assoc Cancer Res 31:273
Kirchner H, Körfer A, Evers P, Szamel MM, Knüver-Hopf J, Mohr H, Franks CR, Pohl U, Resch K, Benter T, Poliwoda H, Atzpodien J (1991) The development of neutralizing antibodies in a patient receiving subcutaneous recombinant and natural interleukin-2. Cancer 67:1862–1864
Kolitz JE, Wong GY, Welte K, Merluzzi VJ, Engert A, Bialas T, Polivka A, Bradley EC, Konrad M, Gnecco C, Oettgen HF, Mertelsmann R (1988) Phase I trial of recombinant interleukin-2 and cyclophosphamide: augmentation of cellular immunity and T-cell mitogenic response with long-term administration of rIL-2. J Biol Response Mod 7:457–472
Mitchell MS, Kempf RA, Harel W, Shau H, Boswell WD, Lind S, Bradley EC (1988) Effectiveness and tolerability of low-dose cyclophosphamide and low-dose intravenous interleukin-2 in disseminated melanoma. J Clin Oncol 6:409–424
Philip T, Stoter G, Gasmin C, Fossa SD, Symann M, Israel L, Rugarli C, Bijman JT, Palmer PA, Franks CR (1989) Recombinant human interleukin-2 without LAK cells in metastatic renal cell carcinoma: the European experience. Proc Am Soc Clin Oncol 30:507
Rosenberg SA, Lotze MT, Muul LM, Chang AE, Avis FP, Leitman S, Linehan WM, Robertson CN, Lee RE, Rubin JT, Seipp CA, Simpson CG, White DE (1987) A progress report on the treatment of 157 patients with advanced cancer using lymphokine-activated killer cells and interleukin-2 or high-dose interleukin-2 alone. N Engl J Med 316:889–897
Rosenberg SA, Lotze MT, Yang JC, Linehan WM, Seipp C, Calabro S, Karp SE, Sherry RM, Steinberg S, White DE (1989) Combination therapy with interleukin-2 and alpha-interferon for the treatment of patients with advanced cancer. J Clin Oncol 7:1863–1874
Towbin H, Staehelin J, Gordon J (1979) Electrophoretic transfer of proteins from polyacrylamide gels to nitrocellulose sheets. Proc Natl Acad Sci USA 76:4350–4354
West WH, Tauer KW, Yannelli JR, Marshall GD, Orr DW, Thurman GB, Oldham RK (1987) Constant-infusion recombinant interleukin-2 in adoptive immunotherapy of advanced cancer. N Engl J Med 316:898–905
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Kirchner, H., de Riese, W., Allhoff, E. et al. Immunotherapy of advanced renal cell cancer using subcutaneous recombinant interleukin-2 and interferon-α. World J Urol 9, 219–222 (1991). https://doi.org/10.1007/BF00182844
Issue Date:
DOI: https://doi.org/10.1007/BF00182844