
Abstract
Growing interest in camelids presents a unique challenge to scientists and veterinarians engaged in diagnosing infectious diseases of this species. It is estimated that 65 % of fatalities in Old World camels (OWC, i.e., Camelus dromedarius and C. bactrianus) and 50 % in New World camelids/South American camelids (NWC/SAC, i.e., the domestic alpaca (Vicugna pacos) and llama (Lama glama)) are caused by infectious diseases. Factors that contribute to disease emergence in camelids involve climate change and increased demand for camel products resulting in the intensification of production and expanding camel contacts with other animal species and humans. In this chapter, the most important emerging diseases of camelids are described and discussed. The most notable emerging viral infections in OWC include camelpox, Rift Valley fever (RVF), peste des petits ruminants (PPR), and Middle East respiratory syndrome coronavirus (MERS-CoV) infection. Brucellosis, Johne’s disease (JD), and dermatophilosis are the emerging bacterial diseases in OWC. Emerging diseases of NWC include infections with bovine viral diarrhea virus (BVDV), bluetongue (BT), and coronavirus. Parasitic emerging infections in NWCs include the small liver fluke (Dicrocoelium dendriticum) and meningeal worm (Parelaphostrongylus tenuis).
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
- Camelids
- Camelpox
- Middle East respiratory syndrome coronavirus
- Rift Valley fever
- Bovine viral diarrhea virus
- Bluetongue
1 Introduction
It is estimated that 65 % of fatalities in Old World camels (OWC, i.e., Camelus dromedarius and C. bactrianus) and 50 % in New World camelids/South American camelids (NWC/SAC, i.e., the domestic alpaca (Vicugna pacos) and llama (Lama glama)) are caused by infectious diseases (Wernery and Kaaden 2002). In the past, camels were used mainly for transportation beside their role as the main source of milk and meat for pastoralists. Dromedary camel in sub-Saharan Africa was traditionally known to be reared in the arid and semiarid lands. Due to aridity and desertification, they obliged to move to the higher rainfall areas side by side with other domestic livestock and wildlife. This change resulted in exposure of camels to diseases that were uncommon in their natural habitat such as dermatophilosis, tick paralysis, trypanosomosis, and brucellosis. The situation in Niger, Chad, and Sudan is an example where diseases like contagious ecthyma, trypanosomosis, and tick paralysis have become very serious with increased mortality rates due to the migration of camels south of their well-known camel belt. Drought in the Sahel and the Horn of Africa has also brought pastoralists closer to urban centers, and sales of camel milk became their main source of cash income. Due to an increased demand of urban populations of many countries, particularly in North Africa and the Middle East for camel milk, many dairy farms are established in intensive and semi-intensive systems. This development may be responsible for making camels more susceptible to certain disease. Brucellosis, enterotoxemia, and Johne’s disease are examples of these diseases. A similar situation could be envisaged for an increased incidence of enterotoxemia in camels when raised in an intensive husbandry system as in the UAE (Wernery and Kaaden 2002) or Syria (Khalafalla AI 2015, personnel communication). Changes in animal husbandry related to increasing camel contacts with other animal species, such as equids, may cause disease emergence. Examples of newly emerged diseases of camels resulting from sharing premises with equines are glanders (Wernery et al. 2011), melioidosis (Wernery et al. 1997), and Rhodococcus equi infection (Kinne et al. 2011). Another factor that may contribute to the emergence of camel diseases is the migration into new habitat that never was reached before by camels (Faye and Vias 2010).
2 Emerging Viral Diseases of Camels
2.1 Camelpox
Camelpox is the only camel disease included in the OIE’s list of reportable diseases. A chapter on camelpox has been recently added to the OIE’s manual of terrestrial animal diseases, following its endorsement by OIE’s assembly during the general session of May 2014. A special research interest in camelpox has resulted in numerous publications on different aspects of the disease and the causative virus. This is mainly attributable to the resemblance of the CMLV to small poxvirus (Baxby 1974). Interestingly, the CMLV is recently becoming the subject for studies on antiviral therapies (Duraffour et al. 2014), cellular ion channel analysis, and apoptosis.
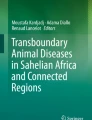
Camelpox is a highly contagious skin disease and the most frequent infectious viral disease of the camelids that occurs in almost every country in which camel husbandry is practiced (Fig.20.1). Outbreaks have been reported in Asia (Bahrain, Iran, Iraq, Oman, Saudi Arabia, the UAE, Yemen, Syria, Afghanistan, southern parts of Russia and India, and Pakistan) and in Africa (Algeria, Egypt, Ethiopia, Kenya, Mauritania, Morocco, Niger, Somalia, and Sudan). The disease is endemic in these countries, and a pattern of sporadic outbreaks occurs with a rise in the seasonal incidence usually during the rainy season (OIE 2008). The disease was recently reported from Saudi Arabia (Yousif 2011), India (Bhanuprakash et al. 2010; Bera et al. 2011), Ethiopia (Ayelet et al. 2013), and Iran (Mosadeghhesari et al. 2014).

Distribution of reported outbreaks of the important camelids diseases
2.1.1 The Etiology
Camelpox is caused by the camelpox virus (CMLV), which belongs to the genus Orthopoxvirus (OPXV) of the subfamily Poxvirinae in the family Poxviridae. Phylogenetic analysis of CMLV revealed that CMLV is most closely related to variola virus (VARV), sharing all genes involved in basic replicative functions and the majority of genes involved in other host-related functions (Afonso et al. 2002; Gubser and Smith 2002).
2.1.2 Clinical Picture
The disease is species specific and characterized by localized or generalized pox lesions that vary in severity in correlation with age of affected animals (Khalafalla and Mohamed 1996). Pox lesion of various stages may develop, particularly on the face, the neck, and under the tail (Fig. 20.2). Other symptoms include fever and lymph node enlargement. Abortion rates may reach 87 %, as observed by Al Zi’abi et al. (2007) in Syria.

Early skin lesion of camelpox in dromedary camels
2.1.3 Diagnosis
The presumptive diagnosis of camelpox infection can be made based on clinical signs. However, infections of camels in the early clinical stages and in mild cases should be differentiated from contagious ecthyma, which is caused by a Parapoxvirus (PPV), papilloma virus infections, and insect bites (Khalafalla et al. 1998; Bhanuprakash et al. 2010). Various laboratory techniques are available for the diagnosis of camelpox including virus isolation, electron microscopy, serology, and polymerase chain reaction (PCR).
2.1.4 Zoonotic Potentiality
It has been over 106 years since camelpox was first described in Punjab, India, in 1909 (Wernery and Kaaden 2002), but the zoonotic nature of the CMLV remained a debate. According to Baxby (1972), CMLV is different from the VARV, the causative agent of smallpox, and is incapable of infecting man. Kritz in Somalia (Kritz 1982) described the first report of a case of human camelpox. The case was a 40-year-old camel herder who developed lesions resembling those of smallpox in June 1978. From the 1970s until recently, it has been well accepted that CMLV rarely infects humans (Duraffour et al. 2011). This is probably due to the cross-immunity induced via smallpox vaccination that ended in the late 1970s. It was therefore postulated that human camelpox may become more common as the immunity of the human population wanes (Duraffour et al. 2011). Human population more than three decades after cessation of the smallpox vaccination has lost protection against that deadly virus and all zoonotic infections caused by human and animal OPVs as well. The first conclusive evidence of zoonotic CMLV infection in humans, associated with outbreaks in dromedary camels, has been recently reported in India where three human cases of camelpox have been reported (Bera et al. 2011). They were detected in animal handlers during an outbreak of camelpox, and the lesions were confined to the hands and fingers of camel handlers and passed through all the stages of pox lesions until the formation of scabs. These are the first confirmed cases of zoonotic camelpox as infection was diagnosed by conventional PCR and seroconversion. Additional four cases of camelpox in humans (camel herders) were detected recently in 2015 in Showak area of Eastern Sudan (Khalafalla et al. 2016, Vector borne & Zoonotic Diseases, accepted) (Fig. 20.3).

Lesion of camelpox on hand of a camel herder, Sudan
2.2 Rift Valley Fever (RVF)
Rift Valley fever is an acute viral, mosquito-borne disease that affects domestic animals (such as sheep, cattle, and goats) and humans distributed in sub-Saharan African countries and the Arabian Peninsula.
RVF is caused by an RNA virus of the family Bunyaviridae, genus Phlebovirus. Camels have been regularly involved in the RVF epidemics in East Africa and Egypt. However, clinical disease is not seen in adult camels, but abortion occurs and some early deaths have been observed (OIE 2008). Serological evidence of dromedary camel infection with RVF was documented. According to Davies et al. (1985), camel sera collected after an epizootic of Rift Valley fever in Kenya revealed positive sera with high titers of serum neutralizing antibody found in 22 % of camels at one of the seven sampling sites. Furthermore, the demonstration of specific IgG antibodies in camels (Nabeth et al. 2001) indicates that these animals are naturally infected. The disease emerged in Egypt in 1977, in Mauritania in 1998 (Nabeth et al. 2001), and in the Arabian Peninsula in 2000 (Abdo-Salem et al. 2006). In addition, the disease reappeared in Kenya in 2006/2007 (Bird et al. 2008). It also involved camels beside sheep, goats, and humans, again with abortion as the only clinical symptom.
Recently, El Mamy et al. (2014) have reported confirmatory evidence for a field camel infection with RVF. In September of 2010, an RVF outbreak occurred in northern Mauritania involving mass abortions in small ruminants and camels (Camelus dromedarius) and at least 63 human clinical cases, including 13 deaths. In camels, serological prevalence was 27.5–38.5 %, and for the first time, clinical signs other than abortions were reported in this species, including hemorrhagic septicemia and severe respiratory distress (Fig. 20.4). Phylogenetic analyses of the genome of isolates from camels suggested a shared ancestor between the Mauritania 2010 strain and strains from Zimbabwe, Kenya, South Africa, Uganda, and other strains linked to the 1987 outbreak of RVF in Mauritania.

Clinical symptoms of Rift Valley fever in dromedary camels during in Mauritania. (a) Conjunctivitis and ocular discharge, hemorrhages of the gums, and edema of the trough, (b) hemorrhages of gums and tongue (Courtesy of Dr. Ahmed El Mamy)
2.3 Peste Des Petits Ruminants (PPR)
Peste des petits ruminants (PPR) is a highly contagious disease of sheep and goats which has recently reemerged and is now found widely distributed through large parts of Africa, the Middle East, and Asia. The disease is characterized by severe pyrexia, anorexia, ulcerative necrotic stomatitis, diarrhea due to purulent oculo-nasal discharge, and respiratory distress.
The etiology
The disease is caused by the peste des petits ruminant virus (PPRV), which belongs to the Morbillivirus genus of the paramyxovirus family of viruses. PPRV is a non-segmented negative-strand RNA virus closely related to the rinderpest virus of cattle and buffaloes, the measles virus of humans, the distemper virus of dogs and some wild carnivores, and the morbilliviruses of aquatic mammals. To date, genetic characterization of PPR virus strains has allowed them to be categorized into four groups: three from Africa and one from Asia. This virus has a particular affinity for lymphoid tissues and epithelial tissue of the gastrointestinal (GI) and respiratory tracts, where it produces characteristic lesions.
PPR in camelids
Camels were not reported as possible hosts to PPR until Ismail and coauthors (Ismail et al. 1992) in Egypt detected the infection through serology in Sudanese camels. The first documented outbreak of PPR in camels reported from Ethiopia in 1996, consisted of a highly contagious respiratory syndrome with elevated morbidity and low mortality rates (Roger et al. 2000, 2001). Consecutive outbreaks of a similar disease occurred in Eastern Sudan in 2004 and later in Somalia and Kenya. Though investigations in Somalia and Kenya were inconclusive and failed to identify the real causative agent, the disease in Sudan was diagnosed as a PPR virus (small ruminant virus) infection (Khalafalla et al. 2010). The incriminated virus belongs to the genus Morbillivirus in the family Paramyxoviridae—a group of RNA viruses characterized by continuous evolution and species jumping. Newly evolved viruses in this family include phocine distemper virus and Hendra virus, formerly called equine Morbillivirus (Earle et al. 2011).
The clinical and epidemiological picture of the previous PPR-suspected or PPR-confirmed outbreaks in northeast Africa is not similar. At least two forms can be identified: a per acute disease characterized by sudden death, abortion, and diarrhea with a high mortality rate occurred in the region during 2004–2007 (Gluecks and Younan 2010; Dawo 2010; Khalafalla et al. 2010), whereas the early outbreaks (1992–1996) showed an acute respiratory disease with low mortality rates (Roger et al. 2000). The presence of more than one form points to involvement of other pathogens as secondary invaders or to the genetic variations of the causative virus. The last hypothesis was verified by detecting lineage III of PPRV from camels in Ethiopia in 1997 and lineage IV from camels affected by PPRV in 2004 in Sudan (Kwiatek et al. 2011). Kwiatek and coworkers (2011) suggested that a virulent lineage IV strain might have been introduced in Africa during the 1990s, resulting in outbreaks in both camels and small ruminants.
Clinically the disease is characterized by sudden death of apparently healthy animals and yellowish and later bloody diarrhea and abortion (Fig. 20.5). Death has been always sudden and proceeded with colic and difficulty in respiration. Mortality rate ranges between 0 and 50 % and vary in accordance with the area with a mean of 7.4 %. More than 80 % of deaths were in pregnant and recently delivered she-camels.

Carcasses of camels died of PPRV infection scattered in northern Butana, Sudan in 2004
2.4 Middle East Respiratory Syndrome Coronavirus Infection in Dromedary Camels
Middle East respiratory syndrome coronavirus (MERS-CoV) is an emerging pathogen associated with severe respiratory symptoms and renal failure in infected persons. Saudi Arabia is the country most severely affected by the virus and is where the first recognized case was reported in September 2012. The origin of MERS-CoV remains a mystery. Phylogenetic analyses of complete and partial genome sequences by Cotten et al. (2013) enabled estimates of the timing of introduction and geographic distribution of distinct virus clades. The authors proposed that MERS-CoV emerged in humans in 2011 and noted that sequence divergence among clades is consistent with multiple sporadic introductions of the virus into the human population, presumably from an animal reservoir (Alagaili et al. 2014).
Early observations that some MERS-CoV infected people had exposure to camels suggesting a possible role of this animal as an intermediate reservoir host (Milne-Price et al. 2014; Albarrak et al. 2012; Drosten et al. 2013). Serologic surveys subsequently conducted in several countries in the Arabian Peninsula and Africa have identified high rates of MERS-CoV-specific antibodies in camels (Hemida et al. 2013; Perera et al. 2013; Reusken et al. 2013; Meyer et al. 2014). Furthermore, researchers have found definitive proof that camels can be infected with MERS-CoV when viral genomic sequences were detected in nasal swabs collected in Qatar (Haagmans et al. 2014; Nowotny and Kolodziejek 2014), Saudi Arabia (Memish et al. 2014), and Egypt (Chu et al. 2014).
Infection in camels
Susceptibility of dromedary camels to and infection with MERS-CoV have been documented by the detection of high levels of antibodies to the virus and viral sequences in nasal swabs and lung tissues. Nevertheless, infection remained subclinical with only mild upper respiratory tract symptoms (Fig. 20.6) observed in some camels (Khalafalla et al. 2015). Experimental infection of dromedary camels with a human isolate of MERS-CoV induced no systemic illness despite shedding of large quantities of virus from the upper respiratory tract (Adney et al. 2014). It is therefore concluded that MERS-CoV causes no well-defined disease in camels.

Symptoms of MERS-CoV infection in a 10-month-old dromedary camel
3 Emerging Bacterial Infections
3.1 Brucellosis
Brucellosis is one of the most important worldwide zoonosis affecting livestock and humans. The disease is regarded as one of the most widespread diseases in the world by the Food and Agriculture Organization of the United Nations (FAO), the World Health Organization (WHO), and the World Animal Health Organization (OIE).
3.1.1 The Etiology
Camels of both species (Camelus dromedarius and Camelus bactrianus) are highly susceptible to brucellosis caused by B. melitensis and B. abortus. However, too few bacteriological surveys have been conducted to draw conclusions on the relative importance of either species of Brucella in the etiology of camel brucellosis in the respective countries (Abbas and Agab 2002). A recent report regarded brucellosis as a regionally emerging zoonotic disease in North Africa, the Middle East, and India (Gwida et al. 2010). Camels are infected by Brucella abortus and B. melitensis, which cause abortion and infertility (Wernery and Kaaden 2002). B. melitensis was isolated from camels in Iran, Libya, and Saudi Arabia; B. abortus was isolated in Sudan, Egypt, and Kuwait.
3.1.2 The Disease in Camelids
Serological surveys of camels conducted in many countries indicated that seroprevalence of B abortus ranged from 2 to15 %. However, recent reports showed a substantial increase in seroprevalence over the past few years (Ahmed et al. 2010). The increase reached 37.5 % in some areas in Sudan (Omer et al. 2010). Clinical disease was also reported (Musa et al. 2008; Al-Majali et al. 2008). Clinically, brucellosis in camelids induce symptoms similar to those in other livestock species. However, various researchers have noticed that abortion related to brucellosis is less in camels in comparison to other animals. Brucella infections in camels may cause stillborn calves, retained placenta, fetal death, mummification, reduced milk yield, delayed service age, and fertility (Wernery 2015).
3.2 Paratuberculosis (Johne’s Disease)
Johne’s disease (JD), also known as paratuberculosis, is widespread, chronic, and debilitating disease that affects mainly ruminants and causes severe economic loss. Once animals are infected, the disease gradually advances toward its chronic form, which is characterized by granulomatous enteritis, progressive weight loss with diarrhea, and finally death.
3.2.1 The Causative Agent
Mycobacterium avium subspecies paratuberculosis (MAP) causes Johne’s disease in domestic and wild ruminant and in camelids. A recent study by Ghosh and coauthors based on gene typing of MAP isolates from Saudi Arabia indicated that all isolates belong to the sheep lineage of strains, suggesting a putative transmission from infected sheep herds (Ghosh et al. 2012).
3.2.2 Disease in Camelids
JD affects camels worldwide, causing characteristic clinical illness of severe diarrhea ending in death (Manefield and Tinson 1997; Wernery and Kaaden 2002) (Fig. 20.7). The course of disease is often more rapid than that in cattle (Higgins 1986). Reports from Saudi Arabia described many deaths due to this disease. According to Gameel et al. (1994), nine camels died after displaying characteristic symptoms. The diagnosis was laboratory confirmed, and according to owners, 53 camels died in the field after showing typical symptoms. The disease continues to be reported as a serious and invariably fatal disease of the Arabian camel (Alharbi et al. 2012). According to several reports, Johne’s disease is considered an important emerging disease in dromedary camels in the Saudi Arabia and Gulf states.

A 2-year-old camel affected with Johne’s disease
3.3 Glanders and Melioidosis
Glanders in equids caused by Burkholderia mallei recently reappeared in Pakistan and Brazil in 2008 and 2009, respectively, and appeared for the first time in Kuwait and Bahrain in 2010 (Wernery 2009; Roberts et al. 2010). Recently, an outbreak of glanders that killed three dromedaries out of six was diagnosed in Bahrain (Wernery et al. 2011). Melioidosis is a potentially fatal disease caused by the gram-negative bacterium Burkholderia pseudomallei. During 1990, seven out of 13 camels died from the disease in Queensland, Australia (Bergin and Torenbeck 1991). Since then, at least four incidents of melioidosis-related camel deaths have been diagnosed in the northern areas of the Northern Territory in Australia, and a single case was reported from the UAE (Wernery et al. 1997).
3.4 Dermatophilosis
Natural Dermatophilus congolensis infection of camels has been reported, for the first time, in Kenya, Sudan, the UAE, and Saudi Arabia in the mid-1990s (Bornstein 1995, Gitao et al. 1998a; Wernery and Ali 1990) (Fig. 20.8). According to camel owners in the Butana region of Sudan, this disease has never been observed before in their herds (Gitao et al. 1998b).

Dermatophilosis lesion in a 3-year-old dromedary camel
4 Emerging Parasite Infections
4.1 Protozoal Infections
The most important and prevalent disease of camels, trypanosomiasis (Surra) caused by Trypanosoma evansi, has been reported from the Canary Islands, Spain, and recently from France (Molina et al. 1999; Gutierrez et al. 2010). Eimeria spp. have been introduced by importations of camels to Europe, e.g., E. cameli (Bornstein, personnel communication).
4.2 Ectoparasites
Camels harbor several tick species, and some are important vectors of pathogens; protozoal, virus, and bacteria spp. cause tick paralysis and toxicosis (see above). However, their role of transmitting these pathogens to camelids seems to be much less important than it is to other animals and humans (Bornstein 2002). Lately Alkhurma hemorrhagic fever virus (AHFV) was isolated in an Ornithodoros savignyi, the sand sampan, from Saudi Arabia (Charrel et al. 2007). This soft tick has a wide distribution in arid lands and may lay dormant for long periods during harsh conditions. The tick infests many different hosts including camels as well as humans. The AHFV causes an extremely severe hemorrhagic fever in humans with a case fatality rate of >30 %. About 20 human cases have been diagnosed with the infection in Saudi Arabia (Charrel et al. 2007). The authors associate these or some of these cases with tick bite history.
The above is one of many examples of emerging diseases transmitted by ticks and other arthropods (phylum Arthropoda including the class Insecta). The AHFV belong to tick-borne flaviviruses, which are among the medically most important arboviruses in Asia and Europe. Some are very important as human and animal pathogens; others have not yet been associated with human or animal diseases. Changes in human behavior, animal husbandry, land use, and/or climate may change the actual geographical distribution pattern and transmission intensity. This is already taking place, and it is often related to the present climate change. Tick-borne flaviviruses and other arboviruses may increase in medical and veterinary importance as, e.g., in the case with bluetongue virus (see below).
5 Emerging Viral Diseases of New World Camelids (NWC/ SAC)
Increasing numbers of South American camelids (SACs), particularly alpaca (Vicugna pacos) and llama (Lama glama), are being imported to various countries outside of South America, including Europe, for wool (fiber) production, breeding, and as pack and companion animals. These newly introduced species have proved to be susceptible to “old” and new pathogens in their new environments.
Three viral diseases can be regarded as emerging infections in NWCs.
5.1 Infections with Bovine Viral Diarrhea Virus (BVDV)
The BVDV is not limited to cattle, but may be detected in various species. There is documentation of infection of alpacas resulting in reproductive loss and illness. Kim et al. (2009) isolated BVDV from persistently infected alpacas and showed that unique genotypes of the virus may be maintained in the alpaca population even though camelids are susceptible to infection by other genotypes. There is clear evidence that the disease has been present in North American alpaca herds since at least 2001 and likely originated from BVDV-infected cows (van Amstel and Kennedy 2010).
5.2 Bluetongue (BT) Disease
The bluetongue virus (BTV) is an Orbivirus with 24 known sero-variants and is present worldwide. It exists in a broad band around the world covering large parts of the Americas, Africa, southern Asia and northern Australia (Mellor et al. 2008). Occasionally it has occurred on the southern borders of Europe. The BTV is transmitted by midges (Culicoides spp.) and naturally infects domestic and wild ruminants. The disease is considered to be one of the most important infections of domestic livestock. It is quite severe in sheep, less so in cattle. In June 2006, BTV appeared in northern Europe for the first time (Carpenter et al. 2009) and successfully wintered. Subsequently it caused substantial losses in livestock in 2007 and 2008. The virus has never previously occurred so far north anywhere in the world (Mellor et al. 2008). The explanation to this dramatic change in the epidemiology of BT is many, but one is linked to the recent extension in the distribution of its main vector(s) Culicoides imicola and perhaps new Culicoides vector(s) and to the ongoing climatic change (Wilson and Mellor 2009).
Alpacas and llamas are susceptible to BTV infections, but rarely show significant clinical signs. However, they remain infectious for several weeks and may thus serve as reservoirs of infection. Already Rivera et al. (1987) showed that camelids can be infected with BTV. About 100 sampled “healthy” alpacas were positive for specific antibodies against BVT. Although camelids are considered a “low-risk species,” there are reports of cases, e.g., during the recent outbreak of BT in Europe 2007 (Henrich et al. 2007). One alpaca in the area that was affected in Germany during this outbreak was infected within a radius of 5 km from clinically BTV-infected sheep (with high mortality) and cattle. Ortega et al. (2010) described a fatal BTV infection in an alpaca (Vicugna pacos) in California. Meyer et al. (2009) described a lethal BTV infection in llamas. Vaccines are available and are used for ruminants. They are not licensed for SACs but may be used (Zanolari et al. 2010) and are recommended by many.
5.3 Coronavirus Infection
Recently, a novel coronavirus possibly associated with acute respiratory syndrome in alpacas in California, 2007, was reported (Crossley et al. 2010). Despite epidemiological evidence of BVDV, BT, and coronavirus infections in NWCs, current knowledge regarding the impact of these diseases is incomplete.
6 Emerging Parasitic Infections of NWCs
The small liver fluke or the lancet fluke (Dicrocoelium dendriticum) is rarely found in camelids. However, natural infections with this intriguing parasite have been reported from a few countries in alpacas in Europe, Switzerland, Germany (Wenker et al. 1998), and recently Sweden (de-Verdier et al. 2011). Infection rates are most probably rel. high leading to rel. few but significant mortalities. Llamas and alpacas may act as aberrant hosts to some parasites. In the USA, e.g., llamas cohabiting with the common white-tailed deer (Odocoileus virginianus) may be infected with a meningeal worm (Parelaphostrongylus tenuis), a nematode-causing neurological disease in the aberrant hosts (Fowler 1998).
References
Abbas B, Agab H (2002) A review of camel brucellosis. Prev Vet Med 55:47–56
Abdo-Salem S, Gerbier G, Bonnet P, Al-Qadasi M, Tran A, Thiry E, Al-Eryni G, Roger F (2006) Descriptive and spatial epidemiology of Rift valley fever outbreak in Yemen 2000-2001. Ann N Y Acad Sci 1081:240–242
Adney DR, van Doremalen N, Brown VR, Bushmaker T, Scott D, de Wit E, Bowen RA, Munster VJ (2014) Replication and shedding of MERS-CoV in upper respiratory tract of inoculated dromedary camels. Emerg Infect Dis 20(12):1999–2005
Afonso CL, Tulman ER, Lu Z, Zsak L, Sandybaev NT, Kerembekova UZ, Zaitsev VL, Kutish GF, Rock DL (2002) The genome of camelpox virus. Virology 295(1):1–9
Ahmed MO, Elmeshri SE, Abuzweda AR, Blauo M, Abouzeed YM, Ibrahim A, Salem H, Alzwam F, Abid S, Elfahem A, Elrais A (2010) Seroprevalence of brucellosis in animals and human populations in the western mountains region in Libya, December 2006-January (2008). Euro Surveill 15(30):1–3
Alagaili AN, Briese T, Mishra N, Kapoor V, Sameroff SC, de Wit E (2014) Middle East respiratory syndrome coronavirus infection in dromedary camels in Saudi Arabia. MBiol 5:e00884–e00814
Albarrak AM, Stephens GM, Hewson R, Memish ZA (2012) Recovery from severe novel coronavirus infection. Saudi Med J 33:1265–1269
Alharbi KB, Al-Swailem A, Al-Dubaib MA, Al-Yamani E, Al-Naeem A, Shehata M, Hashad ME, Albusadah KA, Mahmoud OM (2012) Pathology and molecular diagnosis of paratuberculosis of camels. Trop Anim Health Prod 44(1):173–177
Al-Majali AM, Al-Qudah KM, Al-Tarazi YH, Al-Rawashdeh OF (2008) Risk factors associated with camel brucellosis in Jordan. Trop Anim Health Prod 40(3):193–200
Al-Ziabi O, Nishikawa H, Meyer H (2007) The first outbreak of camelpox in Syria. J Vet Med Sci 69(5):541–543
Ayelet G, Jenberie S, Belay A, Mohammed A, Mola B, Gizaw Y et al (2013) The first isolation and molecular characterization of camelpox virus in Ethiopia. Antiviral Res 98(3):417–422
Baxby D (1972) Smallpox-like viruses from camels in Iran. Lancet 2:1063–1065
Baxby D (1974) Differentiation of smallpox and camelpox viruses in cultures of human and monkey cells. J Hyg (Lond) 72:251–254
Bera BC, Shanmugasundaram K, Barua S, Venkatesan G, Virmani N, Riyesh T, Gulati BR, Bhanuprakash V, Vaid RK, Kakker NK, Malik P, Bansal M, Gadvi S, Singh RV, Yadav V, Nagarajan G, Balamurugan V, Hosamani M, Pathak KM, Singh RK (2011) Zoonotic cases of camelpox infection in India. Vet Microbiol 152(1–2):29–38
Bergin TJ, Torenbeck LR (1991) Melioidosis in camels. Austr Vet J 68:30–36
Bhanuprakash V, Balamurugan V, Hosamani M, Venkatesan G, Chauhan B, Srinivasan VA, Chauhan RS, Pathak KM, Singh RK (2010) Isolation and characterization of Indian isolates of camel pox virus. Trop Anim Health Prod 42(6):1271–1275
Biological Standard Commission. 2010. www.oie.int/doc/ged/D7690.PDF. Accessed 2/7/2011
Bird BH, Githinji JW, Macharia JM, Kasiiti JL, Muriithi RM, Gacheru SG, Musaa JO, Towner JS, Reeder SA, Oliver JB, Stevens TL, Erickson BR, Morgan LT, Khristova ML, Hartman AL, Comer JA, Rollin PE, Ksiazek TG, Nichol ST (2008) Multiple Virus Lineages sharing recent common ancestry were associated with a Large Rift Valley Fever outbreak among livestock in Kenya during 2006-2007. J Virol 82(22):11152–11166
Bornstein S (1995) Skin diseases of camels, in; Camel keeping in Kenya. Eds; Evans JO., Simpkin SP., Atkins DJ. Range Manage Handbook Kenya 3(8):7–13
Bornstein S (2002) Parasitic diseases. In: Wernery U, Kaaden OR (eds) Infectious diseases in Camelids. Blackwell Science, Berlin/Vienna, pp 267–387
Carpenter S, Wilson A, Mellor PS (2009) Culicoide and the emergence of bluetongue virus in northern Europe. Trends Microbiol 17(4):172–178
Charrel RN, Fagbo S, Moureau G, Algahtani MH, Temmam S, de Lamballerie X (2007) Alkhurma hemorrhagic fever virus in Ornithodoros savignyi ticks. Emerg Infect Dis 13(1):153–155
Chu DKW, Poon LLM, Gomaa MM, Shehata MM, Perera RAPM, Zeid DA, El Rifay AS, Siu LY, Guan Y, Webby RJ, Ali MA, Peiris M, Kayali G (2014) MERS coronaviruses in dromedary camels. Egypt Emerg Infect Dis 20(6):1049–1053
Cotten M, Watson SJ, Kellam P, Al-Rabeeah AA, Makhdoom HQ, Assiri A, Al-Tawfiq JA, Alhakeem RF, Madani H, AlRabiah FA, Al Hajjar S, Al-nassir WN, Albarrak A, Flemban H, Balkhy HH, Alsubaie S, Palser AL, Gall A, Bashford-Rogers R, Rambaut A, Zumla AI, Memish ZA (2013) Transmission and evolution of the Middle East respiratory syndrome coronavirus in Saudi Arabia: a descriptivegenomic study. Lancet 382(9909):1993–2002
Crossley BM, Barr BC, Magdesian KG, Ing M, Mora D, Jensen D, Loretti AP, McConnell T, Mock R (2010) Identification of a novel coronavirus possibly associated with acute respiratory syndrome in alpacas (Vicugna pacos) in California. 2007. J Vet Diagn Invest 22(1):94–97
Davies FG, Koros J, Mbugua H (1985) Rift Valley fever in Kenya: the presence of antibodies to the virus in camels (Camelus dromedarius). J Hyg (Lond) 94:241–244
Dawo F (2010) Mysterious mortality in camels (Camelus dromedarius) in Borana, Ethiopia: evidence of its association with reproductive age groups. Rev Sci Tech Off Int Epiz 29(3):621–628
de Verdier K, Sandros B, Christensson D, Osterman-Lind E, Lindqvist FK, Bornstein S (2011) Lilla leverflundran – första fallet hos alpacka i Sverige (The first case of the lancet fluke (Dicrocoelium dendriticum) in Swedish alpacas). Sv Vet Tidn 10(10):11–16
Drosten C, Seilmaier M, Corman VM, Hartmann W, Scheible G, Sack S (2013) Clinical features and virological analysis of a case of Middle East respiratory syndrome coronavirus infection. Lancet Infect Dis 13:745–751
Duraffour S, Meyer H, Andrei G, Snoeck R (2011) Camelpox virus. Antivir Res 92(2):167–186
Duraffour S, Drillien R, Haraguchi K, Balzarini J, Topalis D, van den Oord JJ, Andrei G, Snoeck R (2014) KAY-2-41, a novel nucleoside analogue inhibitor of orthopox viruses in vivo. Antimicrob Agents Chemother 58(1):27–37
Earle JA, Melia MM, Doherty NV, Nielsen O, Cosby SL (2011) Phocine distemper virus in seals, east coast, United States, 2006. Emerg Infect Dis 17(2):215–220
El Mamy AB, Lo MM, Thiongane Y, Diop M, Isselmou K, Doumbia B, Baba MO, El Arbi AS, Lancelot R, Kane Y, Albina E, Cêtre-Sossah C (2014 Dec) Comprehensive phylogenetic reconstructions of Rift Valley fever virus: the 2010 northern Mauritania outbreak in the Camelus dromedarius species. Vector Borne Zoonotic Dis 14(12):856–861
Faye N, Vias G (2010) The impact of climate change on camel farming system. Proc Int Camel Symp ‘Camel science and development for sustainable livestock’, Garissa, Kenya, KARI Ed, 10-15th June
Fowler M.E. 1998. Medicine and Surgery of South American Camelids: Llama, Alpaca, Vicuña, Guanaco, 2nd edn. Iowa State Press, Ames, p 549
Gameel AA, Ali AS, Razig SA, Brown J (1994) A clinic-pathological study on spontaneous Paratuberculosis in camels in Saudi Arabia. Pak Vet J 4(1):14–19
Ghosh P, Hsu C, Alyamani EJ, Shehata MM, Al-Dubaib MA, Al-Naeem A, Hashad M, Mahmoud OM, Alharbi KB, Al-Busadah K, Al-Swailem AM, Talaat AM (2012) Genome-wide analysis of the emerging infection with Mycobacterium avium subspecies paratuberculosis in the Arabian camels (Camelus dromedarius). PLoS One 7(2):e31947
Gitao CG, Agab H, Khalafalla AI (1998a) Outbreaks of Dermatophilus congolensis infection in camels (Camelus dromedarius) from the Butana region in eastern Sudan. Rev sci tech Off int Epiz 17(3):743–748
Gitao CG, Agab H, Khalafalla AI (1998b) Camel dermatophilosis in Kenya, Sudan and Saudi Arabia. Proceedings of the third annual meeting for animal production under arid conditions, vol 2. United Arab Emirates University Press, United Arab Emirates, pp 93–107
Gluecks IV, Younan M (2010) Camel sudden death syndrome: outbreak of an unknown camel disease in the Horn of Africa. http://www.mbali.info/doc560.htm. Accessed 1/7/2011
Gubser C, Smith GL (2002) The sequence of camelpox virus shows it is most closely related to variola virus, the cause of smallpox. J Gen Virol 83(Pt 4):855–872
Gutierrez C, Desquesnes M, Touratier L, Buscher P (2010) Trypanosoma evansi recent outbreaks in Europe. Vet Parasitol 174(1–2):26–29
Gwida M, Al DS, Melzer F, Rösler U, Neubauer H, Tomaso H (2010) Brucellosis – regionally emerging zoonotic disease? Croat Med J 51:289–295
Gwida M, El-Gohary A, Melzer F, Khan I, Rösler U, Neubauer H (2012) Brucellosis in camels. Res Vet Sci 92:351–355
Haagmans BL, Al Dhahiry SH, Reusken CB, Raj VS, Galiano M, Myers R et al (2014) Middle East respiratory syndrome coronavirus in dromedary camels: an outbreak investigation. Lancet Infect Dis 14(2):140–145
Hemida MG, Perera RA, Wang P, Alhammadi MA, Siu LY, Li M (2013) Middle East respiratory syndrome (MERS) coronavirus seroprevalence in domestic livestock in Saudi Arabia, 2010 to 2013. Euro Surveill 18:20659
Henrich M, Reinacher M, Hamann HP (2007) Lethal bluetongue virus infection in an alpaca. Vet Rec 161(22):764
Higgins AJ (1986) The camel in health and disease. Baillere Tindall, London, 104 p
Ismail TM, Hassan HB, Nawal MA, Rakha GM, Abd El-Halim MM, Fatebia MM (1992) Studies on prevalence of rinderpest and peste des petits ruminants antibodies in camel sera in Egypt. Vet Med J Giza 10(2):49–53
Jezek Z, Kriz B, Rothbauer V (1983) Camel pox and its risk to the human population. J Hyg Epidemiol Microbiol Immunol 27:29–42
Khalafalla AI (2000) Camel contagious ecthyma: risks in young calves. Rev Elev vet Pays Trop 53(2):173–176
Khalafalla AI, Abbas Z, Mohamed MEH (1998) Camel papillomatosis in the Sudan. J Camel Pract Res 5:157–159
Khalafalla AI, Mohamed MEH (1996) Clinical and epizootiological features of camelpox in eastern Sudan. J Cam Pract Res (2): 99–102
Khalafalla AI, Saeed IK, Ali YH, Abdurrahman MB, Kwiatek O, Libeau G, Obeida AA, Abbas Z (2010) An outbreak of peste des petits ruminants (PPR) in camels in the Sudan. Acta Trop 116(2):161–165
Khalafalla AI, Lu X, Al-Mubarak AI, Dalab AH, Al-Busadah KA, Erdman DD (2015) MERS-CoV in upper respiratory tract and lungs of dromedary camels, Saudi Arabia, 2013–2014. Emerg Infect Dis 21(7):1153–1158. doi:10.3201/eid2107.150070
Kim SG, Anderson RR, Yu JZ, Zylich NC, Kinde H, Carman S, Bedenice D, Dubovi EJ (2009) Genotyping and phylogenetic analysis of bovine viral diarrhea virus isolates from BVDV infected alpacas in North America. Vet Microbiol 136(3–4):209–216
Kinne J, Madarame H, Takai S, Jose S, Wernery U (2011) Disseminated Rhodococcus equi infection in dromedary camels (Camelus dromedarius). Vet Microbiol 149(1–2):269–272
Kritz B (1982) A study of camelpox in Somalia. J Comp Pathol 92:1–8
Kwiatek O, Ali YH, Saeed IK, Khalafalla AI, Mohamed OI, Abu OA, Abdelrahman MB, Osman HM, Taha KM, Abbas Z, El Harrak M, Lhor Y, Diallo A, Lancelot R, Albina E, Libeau G (2011) Asian lineage of peste des petits ruminants virus. Afr Emerg Infect Dis 17(7):1223–1231
Manefield GW, Tinson AH (1997) Camels – a compendium. Sydney Post Graduate Foundation, Australia, Vademecum Series C No 22
Mellor PS, Carpenter S, Harrup L, Baylis M, Mertens PP (2008) Bluetonge in Europe and the Mediterranean Basin: history of occurrence prior to 2006. Prev Vet Med 87(1–2):4–20
Memish ZA, Cotten M, Meyer B, Watson SJ, Alsahafi AJ, Al Rabeeah AA et al (2014) Human infection with MERS coronavirus after exposure to infected camels, Saudi Arabia, 2013. Emerg Infect Dis 20(6):1012–1015
Meyer G, Lacroux C, Léger S, Top S, Goyeau K, Deplanche M (2009) Lethal Bluetongue virus serotype 1 infection in llamas. Emerg Infect Dis 15(4):608–610
Meyer B, Müller MA, Corman VM, Reusken CBEM, Ritz D, Godeke GD (2014) Antibodies against MERS coronavirus in dromedary camels, United Arab Emirates, 2003 and 2013. Emerg Infect Dis 20:552–559
Milne-Price S, Miazgowicz KL, Munster VJ (2014) The emergence of the Middle East respiratory syndrome coronavirus. Pathog Dis 71(2):121–136
Molina JM, Ruiz A, Juste MC, Corbera JA, Amador R, Guitierrez C (1999) Seroprevalence of Trypanosoma evansi in dromedaries (Camelus dromedarius) from the Canary islands (Spain) using an Antibody Ab-ELISA. Prev Vet Med 47(1–2):53–59
Mosadeghhesari M, Oryan A, Zibaee S, Varshovi HR (2014) Molecular investigation and cultivation of camelpox virus in Iran. Arch Virol 159(11):3005–3011
Musa MT, Eisa MZ, El Sanousi EM, Abdel Wahab MB, Perrett L (2008) Brucellosis in camels (Camelus dromedarius) in Darfur, Western Sudan. J Comp Pathol 138(2–3):151–155
Nabeth P, Kane Y, Abdalahi MO, Diallo M, Ndiaye K, Schneegans M, Salam A, Mathiot C (2001) Rift Valley fever outbreak, Mauritania, 1998: seroepidemiologic, virologic, entomologic, and zoologic investigations. Emerg Infect Dis 7(6):1052–1054
Nowotny N, Kolodziejek J (2014) Middle East respiratory syndromecoronavirus (MERS-CoV) in dromedary camels, Oman, 2013. Euro Surveill 19(16). pii: 20781
OIE (2008) Manual of diagnostic tests and vaccines for terrestrial animals (terrestrial manual). Office international des épizooties, Paris
Omer MM, Musa MT, Bakhiet MR, Perrett L (2010) Brucellosis in camels, cattle and humans: associations and evaluation of serological tests used for diagnosis of the disease in certain nomadic localities in Sudan. Rev Sci Tech 29(3):663–669
Ortega J, Crossley B, Dechant JE, Drew CP, Maclachlan NJ (2010) Fatal Bluetongue virus infection in an alpaca (Vicugna pacos) in California. J Vet Diagn Investig 22(1):134–136
Perera RA, Wang P, Gomaa MR, ElShesheny R, Kandeil A, Bagato O (2013) Seroepidemiology for MERS coronavirus using microneutralisation and pseudoparticle virus neutralization assays reveal a high prevalence of antibody in dromedary camels in Egypt, June 2013. Euro Surveill 18:20574
Reusken CB, Ababneh M, Raj VS, Meyer B, Eljarah A, Abutarbush S (2013) Middle East respiratory syndrome coronavirus (MERS-CoV) serology in major livestock species in an affected region in Jordan, June to September 2013. Euro Surveill 18:20662
Rivera H, Madewell BR, Ameghino E (1987) Serological survey of viral antibodies in the Peruvian alpaca (Lama pacos). Am J Vet Res 48(2):189–191
Roberts H, Lopez M, Hancock R (2010) International disease monitoring. Vet Rec 167:192–195. doi:10.1136/vr.c5997
Roger F (2006) Descriptive and spatial epidemiology of Rift valley fever outbreak in Yemen 2000-2001. Ann N Y Acad Sci 1081:240–242
Roger F, Yigezu M, Hurard C, Libeau G, Mebratu GY, Diallo A, Faye B (2000) Investigations on a new pathological condition of camels in Ethiopia. J Camel Pract Res 7(2):163–165
Roger F, Guebre YM, Libeau G, Diallo A, Yigezu LM, Yilma T (2001) Detection of antibodies of rinderpest and peste des petits ruminants viruses (Paramyxoviridae, Morbillivirus) during a new epizootic disease in Ethiopian camels (Camelus dromedarius). Rev Méd Vét 152(3):265–268
van Amstel S, Kennedy M (2010) Bovine viral diarrhea infections in new world camelids – a review. Small Rumin Res 21:121–126
Wenker C, Hatt JM, Hertzberg H, Ossent P, Hänichen T, Brack A, Isenbuegel E (1998) Dicrocoeliosis in South American camelids. Tierärtzl Prax 26:355–361
Wernery U (2009) Glanders. In: Mair TS, Hutchinson RE (eds) Infectious diseases of the horse. Equine Veterinary Journal, Ltd., Fordham, pp 253–260
Wernery U (2015) Camelid brucellosis: a review. Rev Sci Tech Off Int Epiz 33(3):839–857
Wernery U, Ali M (1990) Dermatophilose in Renndromedaren – Fallbereicht. Tierärztl Umschau 45(3):209–210
Wernery U, Kaaden OR (2002) Infectious diseases of Camelids. Blackwell Science, Berlin
Wernery R, Kinne J, Hayden-Evans J, Ul HA (1997) Melioidosis in a seven year old camel. A new disease in the United Arab Emirates (UAE). J Camel Pract Res 4:141–143
Wernery U, Wernery R, Joseph M, Al-Salloom F, Johnson B, Kinne J, Jose J, Jose S, Tappendorf B, Hornstra H, Scholz HC (2011) Natural Burkholderia mallei infection in Dromedary, Bahrain. Emerg Infect Dis 17(7):1277–1279
Wilson AJ, Mellor PS (2009) Bluetongue in Europe: past, present and future. Philos Trans R Soc Lond Ser B Biol Sci 364(1530):2669–2681
Yousif AA, Al Naeem A (2011) Molecular characterization of enzootic camel pox in eastern province of Kingdom of Saudi Arabia. Int J Virol 7(4):135–136
Zanolari P, Bruckner L, Fricker R, Kaufmann C, Mudry M, Griot C, Meylan M (2010) Humoral response to 2 inactivated bluetongue virus serotype-8 vaccines in South American Camelids. J Vet Intern Med 24(4):956–959
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this chapter
Cite this chapter
Khalafalla, A.I. (2017). Emerging Infectious Diseases in Camelids. In: Bayry, J. (eds) Emerging and Re-emerging Infectious Diseases of Livestock. Springer, Cham. https://doi.org/10.1007/978-3-319-47426-7_20
Download citation
DOI: https://doi.org/10.1007/978-3-319-47426-7_20
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-47424-3
Online ISBN: 978-3-319-47426-7
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)