
Abstract
I hear and I forget.
I see and I remember.
I do and I understand.
—Confucius 551–479 BCE
Simulation is increasingly used in nursing education to supplement clinical and didactic learning activities. Simulation is a technique for practice and learning that can be used in many different disciplines as well as for trainees. Simulation is a technique (not a technology) aiming at replacing real experiences with guided ones; that is, it represents a context in which students can exercise and explore various aspects of a specific practical skill. Accordingly, simulation-based learning signifies a useful approach to develop health professionals’ knowledge, skills, and attitudes while protecting patients from unnecessary risks. Simulation involves learning situations that take place under the supervision of an expert or lecturer and is commonly applied as an active learning method in different health disciplines like nursing, social education, radiography, and medicine. This chapter concentrates on historical and pedagogical perspectives of simulation as a learning method in nursing education. Simulation as a learning method builds on pedagogical adult learning theory, with an emphasis on David A. Kolb and Donald Schön’s concepts experience-based learning, reflection-on-action, and reflection-in-action. Simulation-based learning is appropriate for topics such as patient safety, teamwork, and quality of health services. The literature states that simulation contributes positively to nursing students’ situational awareness, their ability to formulate and predict possible consequences of action implemented, decision-making, communication, and teamwork.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
- Simulation
- The history of simulation
- Nursing competence
- Social learning theory
- Adult learning
- Patient safety
1 Introduction
The workday of nurses is increasingly marked by complexity, variation, unpredictability, mutual dependence, and cooperation with other professions. The growing complexity in health services requires nurses to be able to respond quickly and adequately in different situations, act flexibly, and adapt to achieve the desired outcomes and quality of health services [1]. To prepare nursing students for their future everyday work, the nursing education has implemented new pedagogical methods. To satisfy the abovementioned requirements, student active learning methods have received more attention during the last decade; these learning methods are considered necessary to meet society’s demands for proper nursing competence. Consequently, a growing trend of making active learning methods a natural part of the nursing education is seen [2]. In the health services, errors do occur and sometimes with fatal consequences. In the USA, the third most common cause of death is medical errors, with only cardiac disease and cancer being more frequent causes [3]. Reports indicate that 44,000–98,000 deaths per year in American hospitals result from unwanted action, with human errors representing the most common reason [4]. Because of this, comprehensive measures, recommendations, and changes in the health services have been suggested [5]. The World Health Organization (WHO) defines patient safety as “the freedom for a patient from unnecessary harm or potential harm associated with healthcare” [6]. Measures that reduce the risk of patient injuries caused by health staff members, surveillance procedures, and analysis of results, as well as measures that identify new areas of risk, are decisive factors in promoting the quality of health services [7].
In this context, simulation has a key role in training healthcare providers in various procedures to prevent errors and unnecessary injuries. Research indicates that simulation leads to better cooperation skills, improved ability to make decisions in teams, and enhanced critical reflections among nursing students [8]. As a result, patient safety will be increased.
Simulation is a technique for practice and learning that can be utilized in many different disciplines as well as for trainees. Simulation is a technique (not a technology) aiming at replacing real experiences with guided ones; that is, it represents a context in which students can exercise and explore various aspects of a specific practical skill. Accordingly, simulation-based learning signifies a useful approach to develop health professionals’ knowledge, skills, and attitudes while protecting patients from unnecessary risks [7].
Through simulation as a learning method, the students can enhance their skills without the risk of causing injuries or damages to patients, colleagues, or equipment. To learn clinical skills under safe conditions enables nursing students to achieve mastery and at the same time have the energy to systematically reflect on their own action and discover the best approaches. Hence, the university lecturer’s role is to facilitate a safe and supportive environment based on fruitful interaction with, as well as between, the students. More effective learning is possible in a context that allows for mistakes, i.e., learning through trial and error [9].
Simulation as a learning method also involves observation of the student’s interaction with the patient and cooperation with colleagues; those students who participate in simulation exercises can observe behavior, communication and patterns of action among other people. Students working and learning together make it possible to exploit the potential for learning.
This chapter concentrates on simulation as one of several active learning methods that are now applied among nursing students throughout the world.
2 History of Simulator Development
The history of simulator development related to competence development is several centuries old, with its earliest use taking place in the fields of warfare, aviation, and nuclear energy [2]. The military use of simulation dates back to the eighteenth century [10], whereas the aviation industry was instrumental in the modern use of simulation through its focus on safety precautions [11]. Nowadays, pilots are trained in simulators, and this kind of simulation-based training is deemed necessary to protect the safety of passengers.
In the history of medicine, the earliest simulators were the mannequins of father and son Grégoire from Paris; these were primarily meant to assist in the training of midwives. Miss Chase, a life-sized mannequin, was one of the first simulators. She was built by a doll maker named Martha Jenkins Chase, so that nurses can learn how to dress and undress patients during transportation and how to turn patients over in bed (Weir 2012). In their training, nursing students used Miss Chase, other dolls, or fellow students to learn various techniques regarding injection and other basic skills [12].
The health disciplines underwent significant changes during the twentieth century. The knowledge base and learning moved from simple training to scientific principles and eventually toward more demanding methods that required competence in the specific field of knowledge, skills, and implementation. In the 1980s, we witnessed the first high-tech simulators in the health sciences, and in the 1990s, more modern patient simulators were used in the anesthesiology program. At the same time, simulation as a learning method became part of the curriculum of anesthesia nurses [7].
Later in the 1990s, David Gaba transferred the “Crew Resource Management” (CRM) concept from aviation to his specialist area of anesthesiology. CRM was based on the idea that successful interaction requires that the cooperating parties communicate effectively and work toward commonly identified objectives. Doctors and nurses of anesthesiology received training in coordination, communication, teamwork, and leadership with the help of advanced simulators [13].
Simulation as a student-active learning method has now reached a stage where one needs to consider what is technically possible and what is effective in terms of learning. With more recent technological development, it is now possible—using 360-degree video and VR glasses—to move around the room when, for instance, receiving trauma patients.
3 What Is Simulation?
There is currently an increasing use of simulation in nursing program [14]. Simulation can be defined as an active learning method where the objective is to enable the students to acquire a deeper understanding, competence, and capacity for critical reflection [15]. According to Prince (2004, p. 223), student-active learning can be described as:
[…] any instructional method that engages students in the learning process. In short, active learning requires students to do meaningful learning activities and think about what they are doing. […] The core elements of active learning are student activity and engagement in the learning process. Active learning is often contrasted to the traditional lecture where students passively receive information from the instructor.
Simulation is based on phenomena and activities that resemble a clinical context in which one can learn procedures, make decisions, and reflect critically, with the help of role plays, video, and simulators. Simulation can serve as an effective educational method to provide experience and opportunities to learn—in a secure environment—about how to provide efficient nursing care in various clinical cases. In simulation, complex patient situations are replicated, and nursing students get the opportunity to observe, recognize, interpret, and apply relevant information and knowledge to consider which course of action would be most appropriate—before the student reaches a decision and acts in accordance with his/her professional knowledge. During simulation, the situation is only a realistic replication of reality where students interact while making use of skills and communication in a safe environment, without any risk of causing injury to the patient [1].
Simulation can be defined in different ways; the definitions embrace both general descriptions and specific virtual tools. A commonly used general definition of simulation is “an imitation of some real thing, state of affairs, or process” for the practice of skills, problem-solving, and judgment [16]. In nursing and other health disciplines, one often relies on the definition of Pamela Jeffries (2005):
Simulation involves “activities that mimic the reality of a clinical environment and are designed to demonstrate procedures, decision making, and critical thinking through techniques such as role-playing and the use of devices such as interactive videos or mannequins” [17].
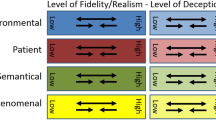
The term fidelity is used to describe the complexity of the simulation learning activity [18]. Fidelity is subdivided into low, medium, and high fidelity. Low fidelity means that one aims to obtain basic nursing skills, like the placement of urinary bladder catheters. Here, the focus is only on the procedure itself, but when moving on to medium fidelity, one expands the complexity of the learning activity requiring more advanced knowledge and techniques. For instance, the placement of urinary bladder catheters takes place in a scenario where the patient suffers from dementia and refuses to be catheterized. High fidelity involves advanced and realistic simulations in anatomy and clinics; here, the perspective is comprehensive and includes communication, decisions in complex clinical situations, interaction in teams, as well as leadership skills [9]. For instance, a scenario may involve a patient with dementia and permanent urinary catheters who also has symptoms of sepsis requiring immediate nursing intervention.
4 The Structure of Simulation
The level of fidelity relates to the complexity of the situation, or what is termed the “scenario”—which aims to cover a specific clinical reality. The level of fidelity is determined by the environment, the materials and equipment used, and factors associated with the students [19].
Simulations range from simple to complex. Simple simulations involve decision environments with low-level uncertainty that can be constructed with high or low levels of relevant information. Information at a high level is easily obtainable and relationships among the key decision variables are highly predictable and very stable [17].
When used as a learning approach in the nursing education, a preparation is needed. That is, a scenario depicting a specific realistic clinical situation is created on beforehand based on the students’ defined learning outcomes [9]. The scenario should include the necessary information to the nursing students, including an outline or description of the required preparations, equipment, case, order of action, as well as the distribution of roles and responsibilities among the participating students. Based on the learning objectives and defined outcomes, the scenario offers a context that is as realistic as possible, including the expected trajectory and pattern of behavior by the students [19]. Establishing a psychological safe environment is vital to ensure that the students feel comfortable to express thoughts without feeling awkward or fearing negative consequences [20]. When simulation is applied as a learning method in nursing, it is common to rely on a structure that consists of four phases: (1) preparation, (2) briefing, (3) patient description/case, and (4) action de-briefing [18]. The first phase of preparation based in the described scenario helps the students identify, interpret, and assess various appropriate courses of action [21]. The preparation which often is termed “Prebriefing” involves preparation and briefing, ensuring that simulation learners are prepared for the simulation learning activity. Prebriefing activities are intended to establish a psychologically safe learning environment by:
-
1.
Situating the learners into a common mental model and preparing learners for the educational content of the simulation-based experience (preparation).
-
2.
Conveying important ground rules for the simulation-based experience (briefing) [22]. Research shows that a good structure for the briefing is important to achieve the learning outcomes [1].
The literature on simulation presents different models used in the de-briefing phase, among them the diamond [23] which is a frequently used simulation model. The diamond de-briefing model implicates that the participants reflect on their experiences during the simulation learning activity. The students identify factors that influence their priorities and thinking in the concrete situation, evaluate the usefulness of their action, and eventually reflect on how the experiences may be used in other situations. The reflection is meant to promote in-depth learning that will enable the students to realize the connection between theory and practical action [23]; this indicates that they understand the reasoning behind their own actions. The reflection is based on the defined learning outcomes resulting from the simulation exercise. Awareness of one’s own body language, either disseminated through concrete responses from the observing participants, the others taking part in the simulation, or video recordings of the exercise, represents an important source of feedback.
5 Pedagogical Perspectives
5.1 Learning as Transformation of Experience
A well-known theory of learning related to simulation is Kolb’s “Experiential Learning Theory” (ELT) [24]. According to Kolb (1984, p. 38), learning is based on experience representing a process whereby knowledge is created through the transformation of experience. Consequently, human beings learn through experience, implying that what people experience denotes the foundation of their learning processes. Transferred to nursing students, they observe, reflect, and try to find new courses of action which in turn generate new experiences that can be reflected upon. In this way, learning has the character of a continuous cycle. Kolb argues that learning is a circular process that consists of four stages of learning, which is portrayed in Fig. 1. Even if it may sound natural to begin with concrete experience, Kolb’s model rather takes the shape of an open circle or spiral, with no beginning or end. Figure 1, developed by the authors, shows that in simulation as a learning activity, we ordinarily start the process with briefing and a concrete experience or a scenario. This is followed by a de-briefing phase where the students reflect on the experience and view the implementation from different perspectives. This represents the cycle in a simulation exercise. Through the reflection in the de-briefing stage, the students will be able to realize the significance of the knowledge and skills they have acquired.

The new knowledge creates the opportunity for abstract conceptualization, which means that the students are challenged to organize and generalize what they experienced during the implementation of the simulation. Subsequently, the students use abstract reflection to produce new theories and hypotheses that could provide solutions to similar problems at a later stage [14]
5.2 Reflection-on-Action and Reflection-in-Action
Donald A. Schön [25] developed the concepts reflection-on-action and reflection-in-action. According to Schön, a professional practitioner is marked by the ability to reflect while acting, that is, doing both things at the same time. If a patient during a simulation exercise gets respiratory problems, the nursing student might be reminded that the patient should be placed in a semi-sitting position. Based on knowledge about anatomic and physiological conditions, a professional practitioner knows this and will implement the required action after observing the patient’s symptoms. Following the simulation, those responsible for the action will by engaging in the scenario be able to reflect individually and together with the other participants. During simulation, the nursing student may carry out the right action but still be unaware on the reasoning behind it. In the de-briefing stage, the lecturer/facilitator or one of the other participants would get the chance to ask, “Why did you place the patient in upright sitting? Why did you carry out exactly this action? Could you have done anything else and achieved the same effect?” Through reflection on action, students raise their awareness. Repetition acts as a key to learning. Hence, if the same scenario is repeated several times, the student will preserve his/her experiences from the first round of implementation and reflection into the next rounds. In this way repetition is important for learning to take place through experience. The de-briefing is most successful when the participants themselves articulate what they handled well and what they need to work more on to act responsibly in similar situations [23,24,25]. To reflect on the action of oneself and others and to receive feedback on your action are central parts of the learning method of simulation.
In the four-stage experiential learning theory, reflection is implicitly present, as concrete action is at the heart of the learning process (Kolb 1984). If the students do not participate in all four stages, the potential for learning will be reduced. In simulation, the lecturer challenges the students to reflect on what they have experienced and observed during the simulation process [24]. Simulation as an active learning method and skills development are closely related to the concepts of Kolb and Schön, namely, experience-based learning, reflection-on-action, and reflection-in-action [14, 25, 26].
6 Simulation and Adult Learning
Simulation is rooted in adult learning theory [27]. Nursing students are seen as adults. What distinguishes adults from children is that adults can draw on the experiences of a lifetime when entering the classroom or a learning situation. Nursing students are adults with clear expectations toward the role of their lecturers as disseminators of knowledge. Adults, and therefore nursing students, tend to learn through interaction with others, and active participation helps reinforce the learning [28]. The sociocultural perspective on learning is based on how communication and language affect learning processes in general. In other words, the foundation of learning is that it happens through active participation, cooperation, and interaction in a social context [29]. Nursing students must realize the necessity of acquiring specific knowledge when solving a problem, a process which is also a source of motivation. In simulation, they need to participate actively and justify their action during the de-briefing stage [30].
Studies indicate that students might experience better learning outcomes, acquire more knowledge, and develop higher skills from high-quality simulation exercises compared to other learning methods, which can be explained by scenarios that appear closer to reality [31,32,33]. These scenarios require the ability to develop and apply clinical knowledge and skills to assess, examine, and communicate with patients, implement procedures, and use clinical reasoning. It has been claimed that simulation leads to improved knowledge and clinical skills while promoting patient safety, teamwork, and professionalism [34]. It may also help develop a deeper understanding (deep learning) and consequently develop critical thinking skills among nursing students. Simulation exercises offer complex scenarios which the students can use to learn action competence [35].
Professional nursing requires knowledge and skills to deal with a number of challenges; well-planned and organized simulation exercises could help in developing students’ critical reflection and clinical competence [36]. Some research emphasizes how de-briefing and reflection are crucial in successful simulation. Along with experienced facilitators, this may enhance students’ learning experience and ability to assess consequences related to the relevant scenario [36]. Simulation represents an important supplement that accords with the best educational standards and ethical principles of the health sciences [37].
Simulation exercises create many opportunities, but do not necessarily imply a guarantee for learning. Students’ learning outcomes depend on the quality of the planning, implementation, and evaluation of the entire simulation exercise. For instance, even if the student has participated and reflected well in the de-briefing stage following simulation, the technical skills are not automatically achieved. The learning outcomes of high-fidelity simulation involve complex settings that demand more than a separate skill, such as the placement of urinary bladder catheters. For example, CRM and confirmatory communication (closed loop) in cardiopulmonary resuscitation (CPR) require that the technical skills are mastered in advance. This means that high-fidelity simulation demands that the students have completed skills training and learned the procedure prior to the simulation.
In the abovementioned example concerning learning CPR, the practical skill training involving compression techniques and the CPR algorithm should take place before the simulation. In case the students have not learned to perform compressions and CPR, their focus is likely to be on carrying out CPR techniques and not on the learning outcomes of CRM and closed loop communication. Accordingly, simulation as a learning method involves a learning process based on a quite simple practical procedure, which will be followed by increasing complexity. When the student is able to apply the practical skills, simulation helps the student reflect when implementing the action and cope with the complexity of the situation [25]. This method allows the students to shape their own experiences and reflections while realizing how things are connected [26]. In the CPR simulation exercise, one can observe both effectiveness and cooperation. The reflection following the implementation stage enables the students to become aware of their action, justify their choices, and discuss other possible ways of handling the situation.
Fero et al. (2010) claim that an early identification of the patient’s clinical changes requires high competence and alertness on the part of the nurse. It is also important that the nurse is capable of critical reflection, good communication skills, and problem-solving skills. The link between critical reflection and concrete action may not be obvious to all nursing students. Here, simulation could contribute to develop analytical skills and improved knowledge among the students, who get the chance to operate in a solution-focused and decisive way while reflecting on their action [17, 36].
7 Summary
In today’s nursing educational program, simulation is used to learn technical skills along with non-technical skills like cooperation, critical thinking, and decision-making before using these skills in a scenario. The opportunity to perform exercises in real-life settings will lead to more patient safety, a greater scope of nursing action, and better quality of nursing care. Simulation is considered a suitable and effective pedagogical learning method that promotes commitment and curiosity among the students. By allowing nurses and other health professionals to train in a secure environment, with no risk of injury to patients, patient safety is enhanced—which is highly warranted.
Action and experience represent the foundation of Kolb’s learning cycle: in simulation-based leaning, both are reflected upon before the next stage of action and assessment takes place. Schön stressed the importance of reflection-in-action and reflection-on-action, as these are required to obtain more knowledge. Simulation exercises could help the transition from nursing student to clinical professional go more smoothly, as well as improve the quality of the early phase of nursing careers. Through interprofessional simulation experiences, nursing students can prepare for future collaborative practice [38].
References
Lee J, Lee H, Kim S, Choi M, Ko IS, Bae J, et al. Debriefing methods and learning outcomes in simulation nursing education: a systematic review and meta-analysis. Nurse Educ Today. 2020;87:104345.
Aebersold M. The history of simulation and its impact on the future. AACN Adv Crit Care. 2016;27(1):56–61.
Jones F, Passos-Neto CE, Braghiroli OFM. Simulation in medical education: brief history and methodology. Princip Prac Clin Res. 2015;1(2).
Kohn LT, Corrigan JM, Donaldson MS. To err is human: building a safer health system. Washington, DC: National Academies Press (US). Copyright 2000 by the National Academy of Sciences. All rights reserved; 2000.
Institute of Medicine Committee on Quality of Health Care in A. Crossing the quality chasm: a new health system for the 21st century. Washington, DC: National Academies Press (US). Copyright 2001 by the National Academy of Sciences. All rights reserved; 2001.
Organization WH. Patient safety [Web]. WHO. n.d. https://www.euro.who.int/en/health-topics/Health-systems/patient-safety/patient-safety.
Lateef F. Simulation-based learning: just like the real thing. J Emerg Trauma Shock. 2010;3(4):348–52.
Foronda C, Liu S, Bauman E. Evaluation of simulation in undergraduate nurse education: an integrative review. Clin Simul Nurs. 2013;9(10):409–16.
World Health Organization. Simulation in nursing and midwifery education. 2018. https://www.euro.who.int/en/health-topics/Health-systems/nursing-and-midwifery/publications/2018/simulation-in-nursing-and-midwifery-education-2018. Accessed 28 Oct 2021.
Bradley P. The history of simulation in medical education and possible future directions. Med Educ. 2006;40(3):254–62.
Scherer YK, Bruce SA, Graves BT, Erdley WS. Acute care nurse practitioner education: enhancing performance through the use of clinical simulation. AACN Clin Issues. 2003;14(3):331–41.
Nickerson M, Pollard M. Mrs. Chase and her descendants: a historical view of simulation. Creat Nurs. 2010;16(3):101–5.
Gaba DM. The future vision of simulation in health care. Qual Saf Health Care. 2004;13(Suppl 1):i2–10.
Akselbo I, Killingberg H, Aune I. Simulation as a pedagogical learning method for critical paediatric nursing in Bachelor of Nursing programmes: a qualitative study. Adv Simul (Lond). 2020;5:24.
Brannan JD, White A, Bezanson JL. Simulator effects on cognitive skills and confidence levels. J Nurs Educ. 2008;47(11):495–500.
Rosen KRM. The history of medical simulation. J Crit Care. 2008;23:157–66.
Jeffries PR. A framework for designing, implementing, and evaluating simulations used as teaching strategies in nursing. Nurs Educ Perspect. 2005;26(2):96–103.
INACSL Standards Commitee, McDermott DS, Ludlow J, Horsley E, Meakim C. Healthcare simulation standards of best practiceTM prebriefing: preparation and briefing. Clin Simul Nurs. 2021;58:9–13.
World Health Organization. Simulation in nursing midwife education: World Health Organization. 2018. https://www.euro.who.int/__data/assets/pdf_file/0011/383807/snme-report-eng.pdf.
Turner S, Harder N. Psychological safe environment: a concept analysis. Clin Simul Nurs. 2018;18:47–55.
Morton PG. Academic education. Creating a laboratory that simulates the critical care environment. Crit Care Nurse. 1996;16(6):76–81.
McDermott DS, Horsley E, Meakim C. Healthcare simulation standards of best practiceTM prebriefing: preparation and briefing. Clin Simul Nurs. 2021;58:9–13.
Jaye P, Thomas L, Reedy G. ‘The Diamond’: a structure for simulation debrief. Clin Teach. 2015;12(3):171–5.
Kolb DA. Experiential learning: experience as the source of learning and development. Upper Saddle River: FT Press; 2014.
Schon D. The reflective practitoner—how professionals think in action. New York: Harper Collins Publishers; 1983.
Kolb AY, Kolb DA. Experiential learning theory: a dynamic approach to management learning, education, and development. In: Armstrong SJ, Fukami C, editors. Handbook of management learning, education and development. Thousand Oaks: SAGE; 2009.
Rutherford-Hemming T. Simulation methodology in nursing education and adult learning theory. Adult Learn. 2012;23(3):129–37. https://doi.org/10.1177/1045159512452848.
Foley G. Dimensions of adult learning. Melbourne: Open University Press; 2004. 331 p.
Knowles MS, Holton Iii EF, Swanson RA. The adult learner: the definitive classic in adult education and human resource development. Burlington: Taylor & Francis Group; 2005.
Bryan RL, Kreuter MW, Brownson RC. Integrating adult learning principles into training for public health practice. Health Promot Pract. 2009;10(4):557–63.
Akselbo I, Olufsen V, Ingebrigtsen O, Aune I. Simulation as a learning method in public health nurse education. Public Health Nurs. 2018;36(2):226–32.
Harder BN. Use of simulation in teaching and learning in health sciences: a systematic review. J Nurs Educ. 2010;49(1):23–8.
Lindset MA, Aune I. Simulering som pedagogisk metode i lærerutdanning. Scand J Vocations Dev. 2020;5(1):side 46–70.
Nestel DH, Smith J, Krogh K, Bearman M. Simulated learning technologies in undergraduate curricula: an evidence check review for HETI; 2021.
Molnes SI, Hagen IH, Kongshaug AV, Vadset TB, Ryste TO, Alnes RE. Simulering gir økt læringsgevinst. Sykepleien fagutvikling. 2016:1–5.
Hayes C, et al. Nurse interrupted: development of a realistic medication administration simulation for undergraduate nurses. Nurse Educ Today. 2015;26(2):S96–103.
Chetlen AL, Mendiratta-Lala M, Probyn L, Auffermann WF, DeBenedectis CM, Marko J, et al. Conventional medical education and the history of simulation in radiology. Acad Radiol. 2015;22(10):1252–67.
Labrague LJ, McEnroe-Petitte DM, Fronda DC, Obeidat AA. Interprofessional simulation in undergraduate nursing program: an integrative review. Nurse Educ Today. 2018;67:46–55.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2023 The Author(s)
About this chapter

Cite this chapter
Karlsaune, H., Antonsen, T., Haugan, G. (2023). Simulation: A Historical and Pedagogical Perspective. In: Akselbo, I., Aune, I. (eds) How Can we Use Simulation to Improve Competencies in Nursing?. Springer, Cham. https://doi.org/10.1007/978-3-031-10399-5_1
Download citation
DOI: https://doi.org/10.1007/978-3-031-10399-5_1
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-10398-8
Online ISBN: 978-3-031-10399-5
eBook Packages: MedicineMedicine (R0)