
Abstract
Background
The WSP tool has previously been proposed as a method to detect signals for adverse drug reactions utilising time-to-event data without the need for a reference population. The aim of this study was to assess the performance of the tool on two well-known and two suspected adverse drug reactions for bisphosphonates that varied in both frequency and accuracy of reporting time.
Methods
The use of the WSP tool was investigated on data from a matched population cohort study involving data from UK primary care patients exposed to oral bisphosphonates. Four listed/suspected ADRs were selected for investigation: headache, musculoskeletal pain, alopecia and carpal tunnel syndrome. For each suspected ADR, a graphical exploratory analysis was performed and the WSP tool was applied for two censoring periods each.
Results
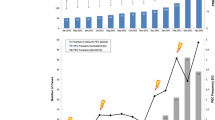
Both of the well-known and common ADRs (headache and musculoskeletal pain) were detected using the WSP tool, and the signals were present regardless of the censoring intervals used. A signal was also detected when the event was uncommon and the timing was likely to be an accurate reflection of onset time (alopecia). This signal was only present for some of the censoring intervals. As anticipated, no signals were raised in the control groups for these events regardless of the censoring interval used. The suspected ADR, which was uncommon and where reporting times may not reflect onset time accurately (carpal tunnel syndrome), was not detected. A signal was raised in the control group but its false-positive nature was visible in the exploratory graphical analysis, which led to it (frequent but for only a limited number of consecutive dates).
Conclusion
This study illustrates the usability and examines the reliability of the WSP tool as a method for signal detection in electronic health records. When the events are uncommon the success of this method may depend on the reporting time accurately reflecting the true event onset time. The study has shown that further work is required to define the censoring periods. The addition of a control group is not required but may enhance causal inference by showing that other causes than the exposure may lead to a signal.




Similar content being viewed by others
References
Coloma PM, Trifiro G, Schuemie MJ, et al. Electronic healthcare databases for active drug safety surveillance: is there enough leverage? Pharmacoepidemiol Drug Saf. 2012; 21(6):611–21.
Johansson S, Wallander MA, de Abajo FJ, et al. Prospective drug safety monitoring using the UK primary-care General Practice Research Database: theoretical framework, feasibility analysis and extrapolation to future scenarios. Drug Saf. 2010;33(3):223–32.
Park MY, Yoon D, Lee K, et al. A novel algorithm for detection of adverse drug reaction signals using a hospital electronic medical record database. Pharmacoepidemiol Drug Saf. 2011;20(6):598–607.
Schuemie MJ, Coloma PM, Straatman H, et al. Using electronic health care records for drug safety signal detection: a comparative evaluation of statistical methods. Med Care. 2012;50(10):890–7.
Cornelius VR, Sauzet O, Evans SJ. A signal detection method to detect adverse drug reactions using a parametric time-to-event model in simulated cohort data. Drug Saf. 2012;35(7):599–610.
WHO-UMC causality assessment.docx; 2011. Available from: URL:http://who-umc.org/Graphics/24734.pdf. Accessed 12 Dec 2012.
Naranjo CA, Busto U, Sellers EM, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30(2):239–45.
Agbabiaka TB, Savovic J, Ernst E. Methods for causality assessment of adverse drug reactions: a systematic review. Drug Saf. 2008; 31(1).
The Health Improvement Network [cited 2012 Oct 10]. Available from: URL: www.thin-uk.com.
Therneau T. A Package for Survival Analysis in S.: R package version 2.36-14. 2012.
Hess K, Gentleman R. Package ‘muhaz’; 2012 [cited 2012 Nov 16]. Available from: URL: http://cran.r-project.org/web/packages/muhaz/muhaz.pdf. Accessed 12 Dec 2012.
Carvajal A, Martin Diego I de, Matthews J, et al. Carpal Tunnel syndrome associated with bisphosphonates. A population-based cohort study. Pharmacoepidemiol Drug Saf. 2011; 47(12):1863–72. doi:10.1016/j.ejca.2011.03.027.
Jones D, Savage R, Highton JG. Synovitis induced by alendronic acid can present as acute carpal tunnel syndrome. Br Med J. 2005;330(7482):74.
Gomes I, Becker J, Ehlers JA, et al. Seasonal distribution and demographical characteristics of carpal tunnel syndrome in 1039 patients. Arquivos de Neuro-Psiquiatria. 2004; 62(3A):596–9.
The Uppsala Monitoring Centre. Available from: URL:http://www.who-umc.org/. Accessed 12 Dec 2012.
Medicines and Healthcare products Regulatory Agency. Available from: URL: www.mhra.gov.uk/. Accessed 12 Dec 2012.
U.S. Food and Drud Administration. Available from: URL: http://www.fda.gov/safety/FDAsSentinelInitiative/ucm2007250.htm. Accessed 12 Dec 2012.
European Medicines Agency. Available from: URL:http://www.ema.europa.eu/ema/. Accessed 12 Dec 2012.
Eurepean Network of Centres for Pharmacoepidemiology and Pharmacovigilance. Available from: URL: http://www.encepp.eu/. Accessed 12 Dec 2012.
Salas M, Hofman A, Stricker BH. Confounding by indication: an example of variation in the use of epidemiologic terminology. Am J Epidemiol. 1999;149(11):981–3.
Kaplan Y, Kurt SG, Karaer H. Carpal tunnel syndrome in postmenopausal women. J Neurol Sci. 2008;270(1–2):77–81.
Acknowledgments
V. Cornelius and M. Molokhia were supported by the National Institute for Health Research (NIHR) Biomedical Research Centre at Guy’s and St. Thomas’ NHS Foundation Trust and King’s College London. The views expressed are those of these authors and not necessarily those of the NHS, the NIHR or the Department of Health.
Dr. Molokhia has received grants from AstraZeneca, Pfizer and the Serious Adverse Events Consortium (SAEC; collaboration of academia and industry) for studies on drug safety. O. Sauzet, A. Carvajal, A. Escudero and V.R. Cornelius have no other conflict of interest to declare.
The authors would like to thank the reviewers of this paper for their insightful comments, which have greatly improved its quality.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sauzet, O., Carvajal, A., Escudero, A. et al. Illustration of the Weibull Shape Parameter Signal Detection Tool Using Electronic Healthcare Record Data. Drug Saf 36, 995–1006 (2013). https://doi.org/10.1007/s40264-013-0061-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40264-013-0061-7