
Abstract
Purpose
To reduce intensive care unit overcrowding and optimize resources, elderly patients affected by suspected infection with declining clinical conditions could be managed in internal medicine departments with stepdown beds. However, commonly used prognostic scores, as Sequential Organ Failure Assessment (SOFA) or quick SOFA (qSOFA) have never been studied in this specific setting. The aim of this study was to evaluate the role and the accuracy of SOFA and qSOFA as prognostic scores in a population of elderly patients with suspected infection admitted to stepdown beds of two internal medicine departments.
Methods
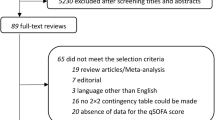
Elderly patients admitted from the emergency department in the stepdown beds of two different internal medicine departments for suspected infection were assessed with SOFA and qSOFA scores at the admission. All patients were treated according to current guidelines. Age, sex, comorbidities, Charlson comorbidity index, SOFA and qSOFA were assessed. In-hospital death and length of hospital admission were also recorded.
Results
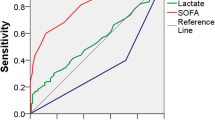
390 subjects were enrolled. In-hospital death occurred in 144 (36.9%) patients; we observed that both SOFA (HR 1.189; 95% CI 1.128–1.253; p < 0.0001) and qSOFA (HR 1.803; 95% CI 1.503–2.164; p < 0.0001) scores were independently associated with an increased risk of in-hospital death. However, the accuracy of both SOFA (AUC: 0.686; 95% CI 0.637–0.732; p < 0.0001) and qSOFA (AUC: 0.680; 95% CI 0.641–0.735; p < 0.0001) in predicting in-hospital death was low in this population.
Conclusion
Elderly patients admitted to stepdown beds for suspected infection experience a high rate of in-hospital death; both SOFA and qSOFA scores can be useful to identify a group of patients who can benefit from admission to an intermediate care environment, however their accuracy is low.



Similar content being viewed by others

Availability of data and material
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
References
Martin GS, Mannino DM, Moss M. The effect of age on the development and outcome of adult sepsis. Crit Care Med (Lippincott Williams and Wilkins). 2006;34:15–21.
Clifford KM, Dy-Boarman EA, Haase KK, Maxvill K, Pass SE, Alvarez CA. Challenges with diagnosing and managing sepsis in older adults. Expert Rev Anti Infect Ther (Taylor and Francis Ltd). 2016;14:231–41.
Girard TD, Ely EW. Bacteremia and sepsis in older adults. Clin Geriatr Med. 2007;23:633–47.
Nasa P, Juneja D, Singh O, Dang R, Arora V. Severe sepsis and its impact on outcome in elderly and very elderly patients admitted in intensive care unit. J Intensive Care Med. 2020;27:179–83.
Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med (Lippincott Williams and Wilkins). 2001;29:1303–10.
Singer M, Deutschman CS, Seymour C, Shankar-Hari M, Annane D, Bauer M, et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. 2016;315:801–10.
Raith EP, Udy AA, Bailey M, McGloughlin S, MacIsaac C, Bellomo R, et al. Prognostic accuracy of the SOFA score, SIRS criteria, and qSOFA score for in-hospital mortality among adults with suspected infection admitted to the intensive care unit. JAMA. 2017;317:290–300.
Ferreira FL, Bota DP, Bross A, Mélot C, Vincent J-L. Serial evaluation of the SOFA score to predict outcome in critically ill patients. JAMA. 2001;286:1754. https://doi.org/10.1001/jama.286.14.1754.
Soo A, Zuege DJ, Fick GH, Niven DJ, Berthiaume LR, Stelfox HT, et al. Describing organ dysfunction in the intensive care unit: a cohort study of 20,000 patients. Crit Care. 2019;23:186. https://doi.org/10.1186/s13054-019-2459-9.
Seymour CW, Liu VX, Iwashyna TJ, Brunkhorst FM, Rea TD, Scherag A, et al. Assessment of clinical criteria for sepsis for the third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. 2016;315:762–74.
Qiao Q, Lu G, Li M, Shen Y, Xu D. Prediction of outcome in critically ill elderly patients using APACHE II and SOFA scores. J Int Med Res. 2012;40:1114–21.
Haas LEM, Termorshuizen F, Lange DW, Dijk D, Keizer NF. Performance of the quick SOFA in very old ICU patients admitted with sepsis. Acta Anaesthesiol Scand (Blackwell Munksgaard). 2020;64:508–16. https://doi.org/10.1111/aas.13536.
Langlais E, Nesseler N, Le Pabic E, Frasca D, Launey Y, Seguin P. Does the clinical frailty score improve the accuracy of the SOFA score in predicting hospital mortality in elderly critically ill patients? A prospective observational study. J Crit Care (W.B. Saunders). 2018;46:67–72.
Wang HE, Shapiro NI, Griffin R, Safford MM, Judd S, Howard G. Chronic medical conditions and risk of sepsis (Gold JA, editor). PLoS ONE. 2012;7:e48307. https://doi.org/10.1371/journal.pone.0048307.
Prin M, Wunsch H. The role of stepdown beds in hospital care. Am J Respir Crit Care Med. 2014;190:1210–6. https://doi.org/10.1164/rccm.201406-1117PP.
Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med (Springer, Berlin). 2017;43:304–77. https://doi.org/10.1007/s00134-017-4683-6.
Vincent JL, de Mendonça A, Cantraine F, Moreno R, Takala J, Suter PM, et al. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: results of a multicenter, prospective study. Working group on “sepsis-related problems” of the European Society of Intensive Care Medicine. Crit Care Med. 1998;26:1793–800. http://www.ncbi.nlm.nih.gov/pubmed/9824069.
Lamontagne F, Harrison DA, Rowan KM. QSOFA for identifying sepsis among patients with infection. JAMA. 2017;317:267–8.
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373–83.
Jones AE, Trzeciak S, Kline JA. The Sequential Organ Failure Assessment score for predicting outcome in patients with severe sepsis and evidence of hypoperfusion at the time of emergency department presentation. Crit Care Med (Lippincott Williams and Wilkins). 2009;37:1649–54.
Freund Y, Lemachatti N, Krastinova E, Van Laer M, Claessens YE, Avondo A, et al. Prognostic accuracy of sepsis-3 criteria for in-hospital mortality among patients with suspected infection presenting to the emergency department. JAMA. 2017;317:301–8.
Galal I, Kassem E, Mansour M. Study of the role of different severity scores in respiratory ICU. Egypt J Bronchol. 2013;7:55. http://www.essbronchology.com1journal.html/text.asp?2013/7/2/55/123995.
Khwannimit B, Bhurayanontachai R, Vattanavanit V. Comparison of the performance of SOFA, qSOFA and SIRS for predicting mortality and organ failure among sepsis patients admitted to the intensive care unit in a middle-income country. J Crit Care (W.B. Saunders). 2018;44:156–60.
Askim Å, Moser F, Gustad LT, Stene H, Gundersen M, Åsvold BO, et al. Poor performance of quick-SOFA (qSOFA) score in predicting severe sepsis and mortality—a prospective study of patients admitted with infection to the emergency department. Scand J Trauma Resusc Emerg Med. 2017;25:56. https://doi.org/10.1186/s13049-017-0399-4.
Wang JY, Chen YX, Guo S, Mei X, Yang P. Predictive performance of quick Sepsis-related Organ Failure Assessment for mortality and ICU admission in patients with infection at the ED. Am J Emerg Med (W.B. Saunders). 2016;34:1788–93.
Scott EC, Ho HC, Yu M, Chapital AD, Koss W, Takanishi DM. Pre-existing cardiac disease, troponin I elevation and mortality in patients with severe sepsis and septic shock. Anaesth Intensive Care. 2008;36:51–9.
Funding
None.
Author information
Authors and Affiliations
Contributions
Conceptualization: LF and NT; methodology: LF, NT, MM; formal analysis and investigation: LF, NT, MM; writing—original draft preparation: LF, NT, MM, VZ, GV; writing—review and editing: MM, VZ, AR, GM, AF, CdP, AM, AS, CN, MB; data acquisition: MM, AF, CdP, AM; supervision: LF, NT, AS, MB.
Corresponding author
Ethics declarations
Conflict of interest
None.
Ethics approval
Ethical approval was waived by the Ethics Committees of both participating centres (INRCA Ethics Committee, Prot. N. 23533/19-CE and CERM Ethics Committee, Prot. N. 2019/387). In view of the retrospective nature of the study and all the procedures being performed were part of the routine care.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Falsetti, L., Martino, M., Zaccone, V. et al. SOFA and qSOFA usefulness for in-hospital death prediction of elderly patients admitted for suspected infection in internal medicine. Infection 48, 879–887 (2020). https://doi.org/10.1007/s15010-020-01494-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s15010-020-01494-5