
Abstract
Objectives
Although chronic obstructive pulmonary disease has been recognized as a significant risk factor for open-heart surgery, the relationship between vital capacity and postoperative outcomes remains unclear. Our objective was to analyze the effect of vital capacity on outcomes after total arch replacement.
Methods
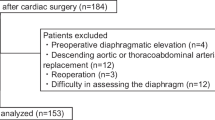
Between January 2003 and December 2018, 228 patients undergoing total arch replacement who were elective cases with preoperative spirometry records were retrospectively reviewed. Patients were divided into two groups, based on whether their preoperative vital capacity was less than or greater than 2.5 L. We compared perioperative data and long-term outcome after adjusting their backgrounds by propensity score matching analysis.
Results
The lower vital capacity group had more tracheostomy patients (5.1% vs 0.0%; p = 0.045). The actuarial survival rate was 58.0% in the lower vital capacity group and 86.3% in the higher vital capacity group at 8 years. Log-rank analysis revealed a significant difference between the two groups (p = 0.011). In the multivariate Cox proportional hazard model, vital capacity < 2.5 L (p = 0.024) and estimated glomerular filtration rate < 30mL/minute/1.73 m2 (p = 0.012) showed a significant association with a higher risk of long-term mortality.
Conclusions
Vital capacity should be considered an important risk factor for postoperative respiratory complications and long-term mortality in patients undergoing total arch replacement.


Similar content being viewed by others

References
Spivack SD, Shinozaki T, Albertini JJ, Deane R. Preoperative prediction of postoperative respiratory outcome: coronary artery bypass grafting. Chest. 1996;109:1222–300.
Samuels LE, Kaufman MS, Morris RJ, Promisloff R, Brockman SK. Coronary artery bypass grafting in patients with COPD. Chest. 1998;113:878–82.
Legare JF, Hirsch GM, Buth KJ, MacDougall C, Sullivan JA. Preoperative prediction of prolonged mechanical ventilation following coronary artery bypass grafting. Eur J Cardiothorac Surg. 2001;20:930–6.
Medalion B, Katz MG, Cohen AJ, Hauptman E, Sasson L, Schachner A. Long-term beneficial effect of coronary artery bypass grafting in patients with COPD. Chest. 2004;125:56–62.
Fuster RG, Argudo JAM, Albarova OG, Sos FH, Lopez SC, Codoner MB, et al. Prognostic value of chronic obstructive pulmonary disease in coronary artery bypass grafting. Eur J Cardiothorac Surg. 2006;29:202–9.
Di Eusanio M, Fortuna D, De Palma R, Dell’Amore A, Lamarra M, Contini GA, et al. Aortic valve replacement: results and predictors of mortality from a contemporary series of 2256 patients. J Thorac Cardiovasc Surg. 2011;141:940–7.
Iba Y, Minatoya K, Matsuda H, Sasaki H, Tanaka H, Kobayashi J, et al. Contemporary open aortic arch repair with selective cerebral perfusion in the era of endovascular aortic repair. J Thorac Cardiovasc Surg. 2013;145:S72–77.
Saleh HZ, Mohan K, Shaw M, Al-Rawi O, Elsayed H, Walshaw M, et al. Impact of chronic obstructive pulmonary disease severity on surgical outcomes in patients undergoing non-emergent coronary artery bypass grafting. Eur J Cardiothorac Surg. 2012;42:108–13.
Miyahara S, Nakai H, Izawa N, Yamanaka K, Sakamoto T, Nomura Y, et al. Influences of chronic obstructive pulmonary disease on outcomes of total arch replacement. Ann Thorac surg. 2015;99:72–8.
Suzuki T, Asai T, Nota H, Kuroyanagi S, Kinoshita T, Takashima N, et al. Selective cerebral perfusion with mild hypothermic lower body circulatory arrest is safe for aortic arch surgery. Eur J Cardiothorac Surg. 2013;43:e94–98.
Asai T, Suzuki T, Nota H, Kuroyanagi S, Kinoshita T, Takashima N, et al. Total arch replacement with selective antegrade cerebral perfusion and mild hypothermic circulatory arrest. Ann Cardiothorac Surg. 2013;2:235–8.
Manganas H, Lacasse Y, Bourgeois A, Perron J, Dagenais F, Maltais F. Postoperative outcome after coronary artery bypass grafting in chronic obstructive pulmonary disease. Can Respir J. 2007;14:19–24.
Angouras DC, Anagnostopoulos CE, Chamogeorgakis TP, Pokkas CK, Swistel DG, Connery CP, et al. Postoperative and long-term outcome of patients with chronic obstructive pulmonary disease undergoing coronary artery bypass grafting. Ann Thorac Surg. 2010;89:1112–8.
Asimakopoulos G, Smith PL, Ratnatunga CP, Taylor KM. Lung injury and acute respiratory distress syndrome after cardiopulmonary bypass. Ann Thorac Surg. 1999;68:1107–15.
Morimoto N, Morimoto K, Morimoto Y, Takahashi H, Asano M, Matsumori M, et al. Sivelestat attenuates postoperative pulmonary dysfunction after total arch replacement under deep hypothermia. Eur J Cardiothorac Surg. 2008;34:798–804.
Dhanani J, Mullany DV, Fraser JF. Effect of preoperative renal function on long-term survival after cardiac surgery. J Thorac Cardiovasc Surg. 2013;146:90–5.
Filsoufi F, Rahmanian PB, Castillo JG, Chikwe J, Carpentier A, Adams DH. Early and late outcomes of cardiac surgery in patients with moderate to severe preoperative renal dysfunction without dialysis. Interact Cardiovasc Thorac Surg. 2008;7:90–5.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None declared.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hachiro, K., Kinoshita, T., Suzuki, T. et al. Impact of vital capacity on outcome after total arch replacement. Gen Thorac Cardiovasc Surg 68, 951–955 (2020). https://doi.org/10.1007/s11748-020-01365-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11748-020-01365-8