
Abstract
Background
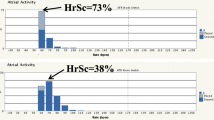
Heart rate score (HRSc), the percentage of atrial sensed and paced beats in the largest 10 beat/min bin of a device histogram and mean intrinsic heart rate (MIHR), predicted survival in nonrandomized studies of implantable defibrillator (ICD) patients. We evaluated whether HRSc and MIHR independently predicted mortality and heart failure (HF) hospitalization in the prospective, randomized, controlled INTRINSIC RV trial.
Methods and results
The INTRINSIC RV trial enrolled 1530 patients receiving dual-chamber ICDs. This analysis involves patients (n = 1471) for whom MIHR and HRSc data were available. Mean follow-up was 10.4 months. The relationship between pre-randomization MIHR and HRSc on the primary endpoint of all-cause mortality and HF hospitalization was assessed using multivariate regression and Cox modeling. As categorical variables, MIHR > 70 bpm and HRSc > 70% were considered high.
Results
The median baseline MIHR and HRSc were 74 (IQR = 16) and 50% (IQR = 20) respectively. As a continuous variable, for every 1% increase in HRSc, death/HF hospitalization increased by 1% (95%CI: 1.002–1.017; p = 0.01). Regression analysis showed baseline MIHR was associated with HRSc (p = 0.01); for every 1 beat/min increase in MIHR, HRSc increased by 1.8%. A MIHR > 70 bpm and HRSc ≥ 70% predicted, but were independently associated with, the primary endpoint (HR: 1.39; 95%CI: 1.10–1.76, p = 0.005 for MIHR and HR: 1.654; 95%CI: 1.11–2.46, p = 0.01 for HRSc). Male gender (HR: 0.75), history of HF (HR: 1.29), and atrial fibrillation (HR: 1.37) also predicted death/hospitalization in the Cox model.
Conclusions
In this large, prospectively studied ICD population, HRSc was a robust and independent predictor of death/HF hospitalization. High MIHR and high HRSc were associated but each predicted outcomes independently.






Similar content being viewed by others

Abbreviations
- HRSc:
-
Heart rate score
- MIHR:
-
Mean intrinsic heart rate
- ICD:
-
Implantable cardioverter defibrillator
- HF:
-
Heart failure
- ROC:
-
Receiver operating characteristic
References
Fox K, Borer JS, Camm AJ, Danchin N, Ferrari R, Lopez Sendon JL, et al. Resting heart rate in cardiovascular disease. J Am Coll Cardiol. 2007;50(9):823–30.
Gopinathannair R, Olshansky B. Resting sinus heart rate and first degree av block: modifiable risk predictors or epiphenomena? Indian Pacing Electrophysiol J. 2009;9(6):334–41.
Ahmadi-Kashani M, Kessler DJ, Day J, Bunch TJ, Stolen KQ, Brown S, et al. Heart rate predicts outcomes in an implantable cardioverter-defibrillator population. Circulation. 2009;120(21):2040–5.
Olshansky B, Richards M, Sharma A, Wold N, Jones P, Perschbacher D, et al. Survival after rate-responsive programming in patients with cardiac resynchronization therapy-defibrillator implants is associated with a novel parameter: the heart rate score. Circ Arrhythm Electrophysiol. 2016;9(8).
Olshansky B, Day JD, Moore S, Gering L, Rosenbaum M, McGuire M, et al. Is dual-chamber programming inferior to single-chamber programming in an implantable cardioverter-defibrillator? Results of the INTRINSIC RV (Inhibition of Unnecessary RV Pacing With AVSH in ICDs) study. Circulation. 2007;115(1):9–16.
Olshansky B, Day J, McGuire M, Pratt T. Inhibition of Unnecessary RV Pacing with AV Search Hysteresis in ICDs (INTRINSIC RV): design and clinical protocol. Pacing Clin Electrophysiol. 2005;28(1):62–6.
Benes J, Kotrc M, Borlaug BA, Lefflerova K, Jarolim P, Bendlova B, et al. Resting heart rate and heart rate reserve in advanced heart failure have distinct pathophysiologic correlates and prognostic impact: a prospective pilot study. JACC Heart failure. 2013;1(3):259–66.
Funding
This study was supported by an Investigator Sponsored Research (ISR) grant from Boston Scientific to the University of Louisville Research Foundation with Dr. Rakesh Gopinathannair as principal investigator.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Rakesh Gopinathannair, MD: Consultant/Honoraria—Abbott Medical, Boston Scientific, Zoll Medical; Physician Advisor—Altathera, PaceMate. Arjun Sharma, MD: Consultant to VivaQuant, Stock (significant)- Boston Scientific Corporation. Brian Olshansky, MD: Boehringer Ingelheim – GLORIA AF co-coordinator, Lundbeck – speaker and consultant, Amarin – Chair, DSMB (REDUCE IT), Sanofi Aventis – consultant. Paul Jones, MS: Boston Scientific Corporation. All the other authors have no relevant conflicts of interest to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
What’s New?
1. In a randomized trial of dual-chamber ICDs, the pre-randomization heart rate score (HRSc), the percent of atrial sensed and paced beats in the largest 10 beat/min bin on a device histogram, independently predicted death or HF hospitalization.
2. This is novel evidence that high HRSc, a marker of chronotropic incompetence and a reduction in heart rate variability, is associated with adverse outcomes in an ICD population.
Tweet:
“How does chronotropic incompetence/’low HR reserve’ affect outcomes? How to measure it? Sharing data on the impact of HR score (% of A-sensed & paced beats in the largest 10 bpm bin on CIED histogram) on death/HF hosp. in ICD pts in the INTRINSIC RV trial @esc_journals #EPeeps”
Rights and permissions
About this article

Cite this article
Gopinathannair, R., Sharma, A., Jones, P. et al. Heart rate score and outcomes in ICD patients: insights from the prospective randomized INTRINSIC RV trial. J Interv Card Electrophysiol 64, 87–93 (2022). https://doi.org/10.1007/s10840-021-01091-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-021-01091-y