
Abstract
Background
Adults with Barrett’s esophagus (BE) are often entered into surveillance for esophageal adenocarcinoma (EAC), although cancer risk is relatively low. BE can be detected in children (< 16 years). Little is known about the epidemiology of pediatric BE, and it is unclear what the optimal surveillance regimes are in children.
Aim
To evaluate the demographic and clinical characteristics, and future neoplastic progression risk in all pediatric BE patients diagnosed in Northern Ireland between 1993 and 2010.
Methods
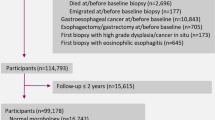
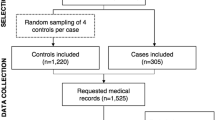
Data from the population-based Northern Ireland BE register were matched to the Northern Ireland Cancer Registry for EAC outcomes until end 2013. Age-adjusted incidence of pediatric BE was calculated, and characteristics between pediatric and adult BE patients compared using Chi-square tests.
Results
Over 18 years, 42 pediatric BE patients (< 16 years) were identified, equivalent to an age-adjusted incidence of < 2 per 100,000 children. There was a clear age differential, with BE incidence increasing with age within the pediatric population. The majority (85.7%) of patients were male, a significantly higher male/female ratio than adult BE patients (p < 0.001). No pediatric BE patients progressed to high-grade dysplasia (HGD) or EAC, although the eldest patient was aged 34 years by the end of follow-up.
Conclusions
This is the largest series of pediatric BE ever reported. It demonstrates that pediatric BE is rare. The male preponderance of this condition is more apparent in childhood compared with adult cases. No children developed HGD/EAC during follow-up, suggesting that regular surveillance is not required, at least until adulthood.


Similar content being viewed by others

References
Fitzgerald RC, di Pietro M, Ragunath K, et al. British Society of Gastroenterology guidelines on the diagnosis and management of Barrett’s oesophagus. Gut. 2014;63:7–42.
Anderson LA, Monaghan P, Murray L, et al. Risk factors for Barrett’s oesophagus and oesophageal adenocarcinoma: results from the FINBAR study. World J Gastroenterol. 2007;13:146–151.
Coleman HG, Bhat S, Murray LJ, McManus D, Gavin AT, Johnston BT. Increasing incidence of Barrett’s oesophagus: a population-based study. Eur J Epidemiol. 2011;26:739–745.
Ford AC, Forman D, Reynolds PD, Cooper BT, Moayyedi P. Ethnicity, gender, and socioeconomic status as risk factors for esophagitis and Barrett’s esophagus. Am J Epidemiol. 2005;162:454–460.
Andrici J, Cox MR, Eslick GD. Cigarette smoking and the risk of Barrett’s esophagus: a systematic review and meta-analysis. J Gastroenterol Hepatol. 2013;28:1258–1273.
Winberg H, Lindblad M, Lagergren J, Dahlstrand H. Risk factors and chemoprevention in Barrett’s esophagus—an update. Scand J Gastroenterol. 2012;47:397–406.
Hassall E. Columnar-lined esophagus in children. Gastroenterol Clin N Am. 1997;26:533–548.
Ronkainen J, Pertti A, Storskrubb T, et al. Prevalence of Barrett’s esophagus in the general population: an endocscopic study. Gastroenterology. 2005;129:1825–1831.
Jeurnink SM, van Herwaarden-Lindeboom MY, Siersema PD, Fischer K, Houwen RH, van der Zee DC. Barrett’s esophagus in children: does it need more attention? Dig Liver Dis. 2011;43:682–687.
Johnston BT, Carré IJ, Thomas PS, Collins BJ. Twenty to forty year follow-up of infantile hiatal hernia. Gut. 1995;36:809–812.
Singendonk MM, Tabbers MM, Benninga MA, Langendam MW. Pediatric gastroesophageal reflux disease: systematic review on prognosis and prognostic factors. J Pediatr Gastroenterol Nutr. 2018;66:239–243.
Hassall E. Barrett’s esophagus: new definitions and approaches in children. J Pediatr Gastroenterol Nutr. 1993;16:345–364.
Hassall E, Weinstein WM, Ament ME. Barrett’s esophagus in childhood. Gastroenterology. 1985;89:1331–1337.
Raicevic M, Sazena A. Barrett’s esophagus in children: what is the evidence? World J Pediatr. 2018;14:330–334.
Dahms B, Greco M, Stranfjord S, Rothstein F. Barrett’s Esophagus in three children after antileukaemia chemotherapy. Cancer. 1987;60:2896–2900.
Lindahl H, Rintala R, Sariola H, Louhimo I. Cervical Barrett’s Esophagus: a common complication of gastric tube reconstruction. J Pediatr Surg. 1990;25:446–448.
Bhat S, Coleman HG, Yousef F, et al. Risk of malignant progression in Barrett’s esophagus patients: results from a large population-based study. J Natl Cancer Inst. 2011;103:1049–1057.
Bhat SK, McManus DT, Coleman HG, et al. Oesophageal adenocarcinoma and prior diagnosis of Barrett’s oesophagus: a population-based study. Gut. 2015;64:20–25.
van Putten M, Johnston BT, Murray LJ, et al. ‘Missed’oesophageal adenocarcinoma and high-grade dysplasia in Barrett’s oesophagus patients: a large population-based study. United Eur Gastroenterol J. 2018;6:519–528.
Kearney T, Donnelly C, Kelly J, O’Callaghan E, Fox C, Gavin A. Validation of the completeness and accuracy of the Northern Ireland Cancer Registry. Cancer Epidemiol. 2015;39:401–404.
Northern Ireland Statistics and Research Agency (NISRA). Northern Ireland Population Projections 2001. Accessed at https://www.nisra.gov.uk/statistics/population on 5th Nov 2019.
Asanuma K, Iijima K, Shimosegawa T. Gender difference in gastro-esophageal reflux diseases. World J Gastroenterol. 2016;22:1800.
Beddow E, Wilcox D, Drake D, Pierro A, Kiely E, Spitz L. Surveillance of Barrett’s esophagus in children. J Pediatr Surg. 1999;34:88–91.
Forssell L, Cnattingius S, Bottai M, Lagergren J, Ekbom A, Akre O. Risk of esophagitis among individuals born preterm or small for gestational age. Clin Gastroenterol Hepatol. 2012;10:1369–1375.
Forssell L, Cnattingius S, Bottai M, et al. Risk of oesophageal adenocarcinoma among individuals born preterm or small for gestational age. Eur J Cancer. 2013;49:2207–2213.
El-Serag HB, Bailey NR, Gilger M, Rabeneck L. Endoscopic manisfestations of gastroesophageal reflux disease in patients between 18 months and 25 years with neurological deficits. Am J Gastroenterol. 2002;97:1635–1639.
Acknowledgments
This research has been conducted using data from the Northern Ireland Cancer Registry which is funded by the Public health Agency from NI. However, the interpretation and conclusions of the data are the sole responsibility of the author(s). The author(s) acknowledge the contribution of the NICR staff in the production of the NICR data. Like all Cancer Registries our work uses data provided by patients and collected by the Health service as part of their care and support.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All the authors have no conflicts of interest regarding this paper.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Twohig-Bennett, L., Coleman, H.G., Cairnduff, V. et al. Esophageal Columnar Metaplasia in Childhood: A Population-Based Case Series Analysis. Dig Dis Sci 66, 2317–2322 (2021). https://doi.org/10.1007/s10620-020-06462-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-020-06462-5