
Abstract
Background and aims
Linked color imaging (LCI) improved the visibility of gastric cancer and colorectal flat lesions. This study aimed to investigate the usefulness of LCI in detecting superficial esophageal squamous cell carcinomas (SESCC).
Methods
We enrolled 37 consecutive SESCC patients (46 SESCCs) diagnosed using LCI and blue laser imaging bright mode (BLI-BRT) and treated in Hiroshima University Hospital between April 2018 and November 2018. Eight professional endoscopists compared images obtained on non-magnifying BLI-BRT and LCI versus conventional white light imaging (WLI). Identification and boundary diagnosis of SESCC with LCI and BLI-BRT were compared with WLI. Changes in lesion visibility were clarified. Interobserver agreement was assessed. Clinicopathological features of lesion that influence visibility with LCI were assessed.
Results
In LCI, 37% (17/46) of cases had improved visibility and 63% (29/46) had unchanged visibility (interobserver agreement = 0.74). Among cases with multiple lugol voiding lesions (LVLs), ΔE between the lesion and background mucosa was significantly higher in LCI than in WLI (20.8 ± 7.9 vs 9.2 ± 6.1, P < 0.05). No significant differences were found in tumor size, morphological type, color, depth, and smoking or drinking history. However, multiple LVLs were significantly higher among cases with improved versus unchanged visibility. On BLI-BRT, 39% (18/46) of cases had improved visibility and 61% (28/46) had unchanged visibility (interobserver agreement = 0.60).
Conclusion
Almost the same as BLI-BRT, LCI improves SESCC visibility compared with WLI. This is useful for cases with multiple LVLs. In cases without background coloration (BGC), LCI may make SESCC more visible than BLI-BRT.



Similar content being viewed by others


References
Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136:E359–E386386.
Takeuchi H, Miyata H, Gotoh M, et al. A risk model for esophagectomy using data of 5354 patients included in a Japanese nationwide web-based database. Ann Surg. 2014;260:259–66.
Hashimoto CL, Iriya K, Baba ER, et al. Lugol’s dye spray chromoendoscopy establishes early diagnosis of esophageal cancer in patients with primary head and neck cancer. Am J Gastroenterol. 2005;100:275–82.
Sreedharan A, Rembacken BJ, Rotimi O. Acute toxic gastric mucosal damage induced by Lugol's iodine spray during chromoendoscopy. Gut. 2005;54:886–7.
Gono K, Obi T, Yamaguchi M, Ohyama N, et al. Appearance of enhanced tissue feature in narrow-band endoscopic imaging. J Biomed Opt. 2004;9:568–77.
Osawa H, Yamamoto H. Present and future status of flexible spectral imaging color enhancement and blue laser imaging technology. Dig Endosc. 2014;26:105–15.
Takenaka R, Kawahara Y, Okada H, et al. Narrow-band imaging provides reliable screening for esophageal malignancy in patients with head and neck cancers. Am J Gastroenterol. 2009;104:2942–8.
Kaneko K, Oono Y, Yano T, et al. Effect of novel bright image enhanced endoscopy using blue laser imaging (BLI). Endosc Int Open. 2014;2:E212–E219219.
Tomie A, Dohi O, Yagi N, et al. Blue laser imaging-bright improves endoscopic recognition of superficial esophageal squamous cell carcinoma. Gastroenterol Res Pract. 2016;6140854:1.
Morita FH, Bernardo WM, Ide E, et al. Narrow band imaging versus lugol chromoendoscopy to diagnose squamous cell carcinoma of the esophagus: a systematic review and meta-analysis. BMC Cancer. 2017;17:54.
Mizumoto T, Hiyama T, Quach DT, et al. Magnifying endoscopy with narrow band imaging in estimating the invasion depth of superficial esophageal squamous cell carcinomas. Digestion. 2018;98:249–56.
Mizumoto T, Hiyama T, Oka S, et al. Diagnosis of superficial esophageal squamous cell carcinoma invasion depth before endoscopic submucosal dissection. Dis Esophagus 2018;31.
Yoshifuku Y, Sanomura Y, Oka S, et al. Evaluation of the visibility of early gastric cancer using linked color imaging and blue laser imaging. BMC Gastroenterol. 2017;17:150.
Fukuda H, Miura Y, Hayashi Y, et al. Linked color imaging technology facilitates early detection of flat gastric cancers. Clin J Gastroenterol. 2015;8:385–9.
Suzuki A, Hara T, Kitagawa Y, et al. Linked-color imaging improves endoscopic visibility of colorectal nongranular flat lesions. Gastrointest Endosc. 2017;86:692–7.
Ninomiya Y, Oka S, Tanaka S, et al. Clinical impact of dual red imaging in colorectal endoscopic submucosal dissection: a pilot study. Therap Adv Gastroenterol. 2016;9:679–83.
Kuehni RG. Color-tolerance data and the tentative CIE 1976 Lab formula. J Opt Soc Am. 1976;66:497–500.
Sato Y, Sagawa T, Hirakawa M, Ohnuma H, et al. Clinical utility of capsule endoscopy with flexible spectral imaging color enhancement for diagnosis of small bowel lesions. Endosc Int Open. 2014;2:E80–87.
Muto M, Hironaka S, Nakane M, et al. Association of multiple Lugol-voiding lesions with synchronous and metachronous esophageal squamous cell carcinoma in patients with head and neck cancer. Gastrointest Endosc. 2002;56:517–21.
Minami H, Isomoto H, Nakayama T, et al. What causes the color change? PLoS ONE. 2014;9:e85553.
Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33:159–74.
Slaughter DP, Southwick HW, Smejkal W. “Field cancerization” in oral stratified epithelium. Cancer. 1953;6:963–8.
Matsubara T, Yamada K, Nakagawa A. Risk of second primary malignancy after esophagectomy for squamous cell carcinoma of the thoracic esophagus. J Clin Oncol. 2003;21:4336–411.
Urabe Y, Kagemoto K, Nakamura K, et al. Construction of a risk model for the development of metachronous squamous cell carcinoma after endoscopic resection of esophageal squamous cell carcinoma. Esophagus. 2019;16:141–6.
Urabe Y, Hiyama T, Tanaka S, et al. Metachronous multiple esophageal squamous cell carcinomas and Lugol-voiding lesions after endoscopic mucosal resection. Endoscopy. 2009;41:304–9.
Katada C, Yokoyama T, Yano T, et al. Alcohol consumption and multiple dysplastic lesions increase risk of squamous cell carcinoma in the esophagus, head, and neck. Gastroenterology. 2016;151(860–869):e7.
Goda K, Dobashi A. Perspectives on narrow-band imaging endoscopy for superficial squamous neoplasms of the orohypopharynx and esophagus. Dig Endosc. 2014;1:1–11.
Den P, Min M, Dong T, et al. Linked color imaging improves detection of minimal change esophagitis in non-erosive reflux esophagitis patients. Endosc Int Open. 2018;6:E1177–E1183183.
Minami H, Isomoto H, Nakayama T, et al. Background coloration of squamous epithelium in esophago-pharyngeal squamous cell carcinoma: what causes the color change? PLoS ONE. 2014;9:e85553.
Tsunoda M, Miura Y, Osawa H, et al. New diagnostic approach for esophageal squamous cell neoplasms using linked color imaging and blue laser imaging combined with iodine staining. Clin Endosc. 2019;52:497–501.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Statement
This study was approved by the Ethics Review Board at Hiroshima University Hospital on April 5, 2018.
Conflict of interest
The authors declare no conflicts of interest associated with this manuscript.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
10388_2020_749_MOESM1_ESM.tiff
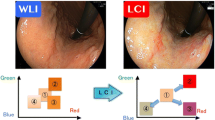
Figure S1. Linked color imaging is an image-enhanced endoscopic observation method that emphasizes slight redness differences by making strong red colors stronger and weaker reddish colors weaker (TIFF 94388 kb)
10388_2020_749_MOESM2_ESM.tiff
Figure S2: The Commission Internationale d’Eclairage (CIE) L*a*b* color space. The CIE L*a*b* color space is a color-opponent space with three dimensions: L* (i.e., lightness), a* (i.e., red to green), and b* (i.e., yellow to blue). The color difference between the lesion and surrounding mucosa (i.e., ΔE) is calculated in the L*a*b* space as the distance between two points (black double arrow). The formula of the color difference is as follows: ΔE*①②=[ (ΔL*)2+(Δa*)2+(Δb*)2 ]1/2. It approximates the visual differences detected by the human eye (TIFF 94388 kb)
10388_2020_749_MOESM3_ESM.tiff
Figure S3. (a) The color scores are (1) L*55 a*29 b*28 in the cancerous part and (2) L*53 a*28 b*19 in the non-cancerous part. The color difference between (1) and (2) in the left white light image is 43. (b) The color score is (3) L*42 a*38 b*8 in the cancerous part and (4) L*56 a*9 b*0 in the non-cancerpart. The color difference between (1) and (2) in the left white light image is 551 (TIFF 94388 kb)
Rights and permissions
About this article

Cite this article
Nakamura, K., Urabe, Y., Oka, S. et al. Usefulness of linked color imaging in the early detection of superficial esophageal squamous cell carcinomas. Esophagus 18, 118–124 (2021). https://doi.org/10.1007/s10388-020-00749-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10388-020-00749-2