
Abstract
Aims
The aim of this study was to identify subgroups of type 2 diabetes mellitus patients with distinct hemoglobin A1c (HbA1c) trajectories. Subgroup characteristics were determined and the prevalence of microvascular complications over time was investigated.
Study design and setting
Data from a cohort of 5,423 type 2 diabetes patients from a managed primary care system were used [mean follow-up 5.7 years (range 2–9 years)]. Latent class growth modeling was used to identify subgroups of patients with distinct HbA1c trajectories. Multinomial logistic regression analyses were conducted to determine which characteristics were associated with different classes.
Results
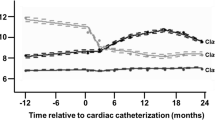
Four subgroups were identified. The first and largest subgroup (83 %) maintained good glycemic control over time (HbA1c ≤53 mmol/mol), the second subgroup (8 %) initially showed severe hyperglycemia, but reached the recommended HbA1c target within 2 years. Patients within this subgroup had significantly higher baseline HbA1c levels but were otherwise similar to the good glycemic control group. The third subgroup (5 %) showed hyperglycemia and a delayed response without reaching the recommended HbA1c target. The fourth subgroup (3.0 %) showed deteriorating hyperglycemia over time. Patients within the last two subgroups were significantly younger, had higher HbA1c levels and a longer diabetes duration at baseline. These subgroups also showed a higher prevalence of retinopathy and microalbuminuria.
Conclusion
Four subgroups with distinct HbA1c trajectories were identified. More than 90 % reached and maintained good glycemic control (subgroup one and two). Patients within the two subgroups that showed a more unfavorable course of glycemic control were younger, had higher HbA1c levels and a longer diabetes duration at baseline.



Similar content being viewed by others

References
UK Prospective Diabetes Study (UKPDS) Group (1998) Intensive blood glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 352:837–853
UK Prospective Diabetes Study Group (1998) Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. BMJ 317:703–713
Ismail-Beigi F, Moghissi E, Tiktin M, Hirsch IB, Inzucchi SE, Genuth S (2011) Individualizing glycemic targets in type 2 diabetes mellitus: implications of recent clinical trials. Ann Intern Med 154:554–559
Kassai B, Erpeldinger S, Wright JM, Gueyffier F, Cornu C (2011) Effect of intensive glucose lowering treatment on all cause mortality, cardiovascular death, and microvascular events in type 2 diabetes: meta-analysis of randomised controlled trials. BMJ 343:d4169
Dailey G (2011) Overall mortality in diabetes mellitus: where do we stand today? Diabetes Technol Ther 13(Suppl. 1):S65–S74
Inzucchi SE, Bergenstal RM, Buse JB et al (2012) Management of hyperglycemia in type 2 diabetes: a patient-centered approach: position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 35:1364–1379
Raz I, Riddle MC, Rosenstock J et al (2013) Personalized management of hyperglycemia in type 2 diabetes: reflections from a diabetes care editors expert forum. Diabetes Care 36:1779–1788
Twisk J, Hoekstra T (2012) Classifying developmental trajectories over time should be done with great caution: a comparison between methods. J Clin Epidemiol 65:1078–1087
Zavrelova H, Hoekstra T, Alssema M et al (2011) Progression and regression: distinct developmental patterns of diabetic retinopathy in patients with type 2 diabetes treated in the diabetes care system West-Friesland, the Netherlands. Diabetes Care 34:867–872
The Expert Committee on the Diagnosis and Classification of Diabetes Mellitus (2003) Follow-up report on the diagnosis of diabetes mellitus. Diabetes Care 26:3160–3167
Aldington SJ, Kohner EM, Meuer S, Klein R, Sjolie AK (1995) Methodology for retinal photography and assessment of diabetic retinopathy: the EURODIAB IDDM complications study. Diabetologia 38:437–444
Rutten GEHM, De Grauw WJC, Nijpels G et al (2006) NHG-standaard diabetes mellitus type 2. Huisarts Wet 49:137–152
Pani L, Nathan DM, Grant RW (2008) Clinical predictors of disease progression and medication initiation in untreated patients with type 2 diabetes and A1c <7%. Diabetes Care 31:386–390
Blumenthal K, Larkin M, Winning G, Nathan D, Grant R (2010) Changes in glycemic control from 1996 to 2006 among adults with type 2 diabetes: a longitudinal cohort study. BMC Health Serv Res 10:158
Shorr RI, Franse LV, Resnick HE, Di Bari M, Johnson KC, Pahor M (2000) Glycemic control of older adults with type 2 diabetes: findings from the Third National Health and Nutrition Examination Survey, 1988–1994. J Am Geriatr Soc 48:264–267
Benoit S, Fleming R, Philis-Tsimikas A, Ji M (2005) Predictors of glycemic control among patients with type 2 diabetes: a longitudinal study. BMC Public Health 5:36
Blaum CS, Velez L, Hiss RG, Halter JB (1997) Characteristics related to poor glycemic control in NIDDM patients in community practice. Diabetes Care 20:7–11
Ali MK, McKeever Bullard K, Saaddine JB, Cowie CC, Imperatore G, Gregg EW (2013) Achievement of goals in U.S. diabetes care, 1999–2010. N Engl J Med 368:1613–1624
Ekström N, Miftaraj M, Svensson A-M et al (2012) Glucose-lowering treatment and clinical results in 163 121 patients with type 2 diabetes: an observational study from the Swedish national diabetes register. Diabetes Obes Metab 14:717–726
Liebl A, Mata M, Eschwege E (2002) Evaluation of risk factors for development of complications in type II diabetes in Europe. Diabetologia 45:S23–S28
Yurgin N, Secnik K, Lage MJ (2007) Antidiabetic prescriptions and glycemic control in German patients with type 2 diabetes mellitus: a retrospective database study. Clin Ther 29:316–325
van der Heijden A, de Bruijne M, Feenstra T et al (2014) Resource use and costs of type 2 diabetes patients receiving managed or protocolized primary care: a controlled clinical trial. BMC Health Serv Res 14:280
Saaddine JB, Cadwell B, Gregg EW et al (2006) Improvements in diabetes processes of care and intermediate outcomes: United States, 1988–2002. Ann Intern Med 144:465–474
Duckworth W, Abraira C, Moritz T et al (2009) Glucose control and vascular complications in veterans with type 2 diabetes. N Engl J Med 360:129–139
UK Prospective Diabetes Study (UKPDS) Group (2008) Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med 358:2560–2572
Stratton IM, Kohner EM, Aldington SJ et al (2001) UKPDS 50: risk factors for incidence and progression of retinopathy in type II diabetes over 6 years from diagnosis. Diabetologia 44:156–163
Avery CL, Kucharska-Newton A, Monda KL et al (2012) Impact of long-term measures of glucose and blood pressure on the retinal microvasculature. Atherosclerosis 225:412–417
Cheung N, Mitchell P, Wong TY (2010) Diabetic retinopathy. Lancet 376:124–136
Levin SR, Coburn JW, Abraira C et al (2000) Effect of intensive glycemic control on microalbuminuria in type 2 diabetes. Veterans Affairs Cooperative Study on glycemic control and complications in type 2 diabetes feasibility trial investigators. Diabetes Care 23:1478–1485
Daniele G, Guardado Mendoza R, Winnier D et al (2014) The inflammatory status score including IL-6, TNFa, osteopontin, fractalkine, MCP-1 and adiponectin underlies whole-body insulin resistance and hyperglycemia in type 2 diabetes mellitus. Acta Diabetol 51:123–131
Fiorentino TV, Prioletta A, Zuo P, Folli F (2013) Hyperglycemia-induced oxidative stress and its role in diabetes mellitus related cardiovascular diseases. Curr Pharm Des 19:5695–5703
Acknowledgments
We thank all general practitioners in the West-Friesland region for there obliging contributions to the study, the research assistants and staff of the Diabetes Care System for the enormous amount of work to collect all the data and the PHARMO network for the opportunity to compare the medication data. This project is supported by a Bridges grant from the International Diabetes Federation. Bridges, an International Diabetes Federation project, is supported by an educational grant from Lilly Diabetes.
Conflict of interest
G.N. received unrestricted grants from Novo Nordisk and Sanofi-Aventis and is member of the advisory board of Eli Lilly. For the other authors, no potential conflicts of interest relevant to this article were reported.
Ethical standard
All human studies have been performed by the appropriate ethics committee and have therefore been performed in accordance with the ethical standards lay down in an appropriate version of the 1964 version of the declaration of Helsinki.
Human and animal rights disclosure
All patients were informed on the use of the data for research purposes.
Informed consent disclosure
Informed consent was obtained from all patients for being included in the study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Managed by Massimo Federici.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Walraven, I., Mast, M.R., Hoekstra, T. et al. Distinct HbA1c trajectories in a type 2 diabetes cohort. Acta Diabetol 52, 267–275 (2015). https://doi.org/10.1007/s00592-014-0633-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00592-014-0633-8