
Abstract
Objectives
To construct models for predicting reintervention after thoracic endovascular aortic repair (TEVAR) of Stanford type B aortic dissection (TBAD).
Methods
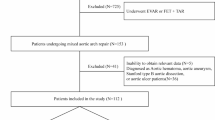
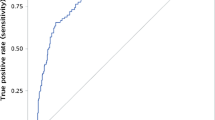
A total of 192 TBAD patients who underwent TEVAR were included; 68 (35.4%) had indications for reintervention. Clinical characteristics, aorta characteristics on pre- and postoperative computed tomography angiography, and aorta characteristics on immediate postoperative aortic digital subtraction angiography were collected. The least absolute shrinkage and selection operator (LASSO) regression was applied to identify the risk factors for reintervention. Eight classifiers were used for modeling. The models were trained on 100 train-validation random splits with a ratio of 2:1. The performance was evaluated by the receiver operating characteristic curve.
Results
Seven predictors of reintervention were identified, including maximum false lumen diameter, aortic diameter measured at the level of approximately 15 mm distal to the left subclavian artery, aortic diameter measured at the level of the diaphragm, false lumen diameter measured at the level of the celiac artery, number of bare-metal and covered stents, number of bare-metal stents, and residual perfusion of the false lumen. Logistic regression (LR) yielded the highest performance, with an area under the curve of 0.802. A nomogram built for clinical use showed good calibration. The cutoff value for dividing patients into low- and high-risk subgroups was 0.413. Kaplan-Meier curves showed that the overall survival of high-risk patients was significantly shorter than that of low-risk patients (both p < 0.05).
Conclusion
Our nomogram could predict the reintervention after TEVAR in patients with TBAD, which may facilitate patient selection and surveillance strategies.
Key Points
• Seven risk factors of reintervention after TEVAR of TBAD were identified for modeling.
• Logistic regression performed best in predicting reintervention with an AUC of 0.802.
• Patients with a high risk of reintervention had shorter OS than those with a low risk.






Similar content being viewed by others

Abbreviations
- AdaBoost:
-
Adaptive boosting
- AUC:
-
Area under the curve
- BPNN:
-
Back propagation neural networks
- CI:
-
Confidence interval
- CTA:
-
Computed tomography angiography
- DSA:
-
Digital subtraction angiography
- IQR:
-
Interquartile range
- KNN:
-
K-nearest neighbor
- k-SVM:
-
Kernel support vector machine
- LASSO:
-
Least absolute shrinkage and selection operator
- LR:
-
Linear regression
- NB:
-
Naive Bayes
- NPV:
-
Negative predictive value
- OS:
-
Overall survival
- PPV:
-
Positive predictive value
- RF:
-
Random forest
- RTAD:
-
Retrograde type A aortic dissection
- TBAD:
-
Type B aortic dissection
- TEVAR:
-
Thoracic endovascular aortic repair
- XGBoost:
-
Extreme gradient boosting
References
Zhang L, Zhao Z, Chen Y et al (2016) Reintervention after endovascular repair for aortic dissection: a systematic review and meta-analysis. J Thorac Cardiovasc Surg 152:1279–1288
Ray HM, Besho JM, Au J et al (2019) The role of ascending aortic size in outcomes of patients with uncomplicated acute type B aortic dissection. J Vasc Surg 69:1011–1020
Ruan ZB, Zhu L, Yin YG, Chen GC (2014) Risk factors of early and late mortality after thoracic endovascular aortic repair for complicated Stanford B acute aortic dissection. J Card Surg 29:501–506
Lou X, Chen EP, Duwayri YM et al (2018) The impact of thoracic endovascular aortic repair on long-term survival in type B aortic dissection. Ann Thorac Surg 105:31–38
Nienaber CA, Rousseau H, Eggebrecht H et al (2009) Randomized comparison of strategies for type B aortic dissection: the INvestigation of STEnt Grafts in Aortic Dissection (INSTEAD) trial. Circulation 120:2519–2528
Qin YL, Wang F, Li TX et al (2016) Endovascular repair compared with medical management of patients with uncomplicated type B acute aortic dissection. J Am Coll Cardiol 67:2835–2842
Xiang D, Kan X, Liang H et al (2019) Comparison of mid-term outcomes of endovascular repair and medical management in patients with acute uncomplicated type B aortic dissection. J Thorac Cardiovasc Surg. https://doi.org/10.1016/j.jtcvs.2019.11.127
Thrumurthy SG, Karthikesalingam A, Patterson BO et al (2011) A systematic review of mid-term outcomes of thoracic endovascular repair (TEVAR) of chronic type B aortic dissection. Eur J Vasc Endovasc Surg 42:632–647
Li Z, Zhang L, Jing Z, Zhou J (2017) Reintervention after thoracic endovascular aortic repair deserves more attention. J Thorac Dis 9:E529–E530
Nienaber CA, Kische S, Ince H et al (2011) Thoracic endovascular aneurysm repair for complicated type B aortic dissection. J Vasc Surg 54:1529–1533
Patterson B, Holt P, Nienaber C et al (2013) Aortic pathology determines midterm outcome after endovascular repair of the thoracic aorta: report from the Medtronic Thoracic Endovascular Registry (MOTHER) database. Circulation 127:24–32
Scali ST, Feezor RJ, Chang CK et al (2013) Efficacy of thoracic endovascular stent repair for chronic type B aortic dissection with aneurysmal degeneration. J Vasc Surg 58:10–17
Boufi M, Patterson BO, Grima MJ et al (2017) Systematic review of reintervention after thoracic endovascular repair for chronic type B dissection. Ann Thorac Surg 103:1992–2004
Khan S, Caputo FJ, Trani J et al (2015) Secondary interventions after endovascular repair of aortic dissections. Ann Vasc Surg 29:1160–1166
Botsios S, Fromke J, Walterbusch G et al (2014) Secondary interventions after endovascular thoracic aortic repair of aortic dissections. J Card Surg 29:66–73
Sailer AM, van Kuijk SM, Nelemans PJ et al (2017) Computed tomography imaging features in acute uncomplicated Stanford type-B aortic dissection predict late adverse events. Circ Cardiovasc Imaging 10. https://doi.org/10.1161/CIRCIMAGING.116.005709
Zhu Y, Luo S, Ding H et al (2019) Predictors associated with an increased prevalence of postimplantation syndrome after thoracic endovascular aortic repair for type B aortic dissectiondagger. Eur J Cardiothorac Surg 55:998–1005
Erbel R, Aboyans V, Boileau C et al (2014) 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur Heart J 35:2873–2926
Hsieh RW, Hsu TC, Lee M et al (2019) Comparison of type B dissection by open, endovascular, and medical treatments. J Vasc Surg 70:1792–1800.e3
Faure EM, Canaud L, Agostini C et al (2014) Reintervention after thoracic endovascular aortic repair of complicated aortic dissection. J Vasc Surg 59:327–333
Chen Y, Zhang S, Liu L et al (2017) Retrograde type A aortic dissection after thoracic endovascular aortic repair: a systematic review and meta-analysis. J Am Heart Assoc. https://doi.org/10.1161/JAHA.116.004649
Xue Y, Sun L, Zheng J et al (2015) The chimney technique for preserving the left subclavian artery in thoracic endovascular aortic repair. Eur J Cardiothorac Surg 47:623–629
Boufi M, Guivier-Curien C, Deplano V et al (2015) Risk factor analysis of bird beak occurrence after thoracic endovascular aortic repair. Eur J Vasc Endovasc Surg 50:37–43
Marcheix B, Rousseau H, Bongard V et al (2008) Stent grafting of dissected descending aorta in patients with Marfan’s syndrome: mid-term results. JACC Cardiovasc Interv 1:673–680
Schwartz SI, Durham C, Clouse WD et al (2018) Predictors of late aortic intervention in patients with medically treated type B aortic dissection. J Vasc Surg 67:78–84
Durham CA, Cambria RP, Wang LJ et al (2015) The natural history of medically managed acute type B aortic dissection. J Vasc Surg 61:1192–1198
Song JM, Kim SD, Kim JH et al (2007) Long-term predictors of descending aorta aneurysmal change in patients with aortic dissection. J Am Coll Cardiol 50:799–804
Manning Brian J, Nuno D, Thomas O et al (2009) Endovascular treatment for chronic type B dissection: limitations of short stent-grafts revealed at midterm follow-up. J Endovasc Ther 16:590–597
Evangelista A, Salas A, Ribera A et al (2012) Long-term outcome of aortic dissection with patent false lumen: predictive role of entry tear size and location. Circulation 125:3133–3141
Kamman AV, Brunkwall J, Verhoeven EL et al (2017) Predictors of aortic growth in uncomplicated type B aortic dissection from the Acute Dissection Stent Grafting or Best Medical Treatment (ADSORB) database. J Vasc Surg 65:964–971
Funding
This work was supported by the National Key Research and Development Program of China (2018YFC1002600); the Science and Technology Planning Project of Guangdong Province, China (No. 2017A070701013, 2017B090904034, 2018B090944002, 2019B020230003); and the Guangdong Peak Project (DFJH201802).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Guarantor
The scientific guarantor of this publication is Meiping Huang.
Conflict of interest
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Statistics and biometry
Weiqi Chen performed the statistical analyses of this paper.
Informed consent
Written informed consent was waived from all subjects (patients) in this study.
Ethical approval
Institutional Review Board approval was obtained.
Methodology
• Retrospective
• Diagnostic or prognostic study
• Performed at single institution
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Dong, Y., Que, L., Jia, Q. et al. Predicting reintervention after thoracic endovascular aortic repair of Stanford type B aortic dissection using machine learning. Eur Radiol 32, 355–367 (2022). https://doi.org/10.1007/s00330-021-07849-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-021-07849-2