
Abstract
Purpose
There is currently no consensus on the optimal drilling direction of the fibular bone tunnel for anterior talofibular ligament (ATFL) reconstruction, and few studies have investigated the potential injury to the peroneus longus and brevis tendons and the possibility of fibular fractures during the drilling process. The aim of this study was to assess the potential risk of drilling the tunnel from different directions and determine the most appropriate tunnel direction. The hypothesis was that drilling the tunnel in the 45-degree direction would be the safest and most suitable for the fibular tunnel.
Methods
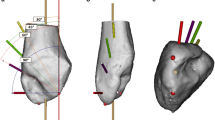
Forty-eight fibular tunnels were drilled on fresh ankle specimens using a K-wire guide and a 5.0 mm hollow drill. Three tunnel orientations were created, parallel to the sagittal plane of the long axis of the fibula and angled 30°, 45°, and 60° to the coronal plane. The length of the fibular tunnel and the distances from the outlet of the K-wire to the peroneus longus and brevis tendons were measured. The occurrence of a fibula fracture was also observed.
Results
The lengths of the bone tunnels in the three groups were 32.9 ± 6.1 mm (30°), 27.2 ± 4.4 mm (45°) and 23.6 ± 4.0 mm (60°). The length of the tunnel drilled at 30° was the longest when compared with that of the tunnels drilled at 45° and 60° (all p values < 0.05). The distances from the outlet of the K-wire to the peroneus longus tendon were 3.0 ± 3.8 mm (30°), 3.8 ± 3.2 mm (45°) and 5.3 ± 1.8 mm (60°), and the distances to the peroneus brevis tendon were 4.2 ± 4.0 mm (30°), 6.1 ± 3.8 mm (45°), 7.9 ± 3.5 mm (60°). In terms of protecting the peroneus longus and brevis tendons, drilling in the 60° direction was better than drilling in the 30° and 45° directions (all p values < 0.05). The risk of injury to the peroneal longus and brevis tendons was 62.5% (30°), 31.3% (45°), and 0% (60°). Although no fibular fractures were observed in any of the three directions, drilling the bone tunnel in the 60° direction disrupted the lateral cortex of the fibula.
Conclusion
This study shows that drilling the tunnel in the 45° direction is less likely to cause injury to the peroneus longus and brevis tendons, while ensuring that the tunnel has a sufficient length and avoiding fracturing the distal fibula. Drilling a fibular bone tunnel in a 45° direction is safer and recommended for ATFL reconstruction.


Similar content being viewed by others


Data availability
Not applicable.
Code availability
Not applicable.
References
Corte-Real N, Caetano J (2021) Ankle and syndesmosis instability: consensus and controversies. EFORT Open Rev 6(6):420–431
Davda K, Malhotra K, O’Donnell P, Singh D, Cullen N (2017) Peroneal tendon disorders. EFORT Open Rev 2(6):281–292
de Vries JS, Krips R, Sierevelt IN, Blankevoort L, van Dijk CN (2011) Interventions for treating chronic ankle instability. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.CD004124.pub3
Dias S, Lewis TL, Alkhalfan Y, Ahluwalia R, Ray R (2022) Current concepts in the surgical management of chronic ankle lateral ligament instability. J Orthop 33:87–94
DiGiovanni BF, Fraga CJ, Cohen BE, Shereff MJ (2000) Associated injuries found in chronic lateral ankle instability. Foot Ankle Int 21(10):809–815
Drakos M, Hansen O, Kukadia S (2022) Ankle instability. Foot Ankle Clin 27(2):371–384
Guillo S, Bauer T, Lee JW, Takao M, Kong SW, Stone JW, Mangone PG, Molloy A, Perera A, Pearce CJ, Michels F, Tourné Y, Ghorbani A, Calder J (2013) Consensus in chronic ankle instability: aetiology, assessment, surgical indications and place for arthroscopy. Orthop Traumatol Surg Res 99(8S):S411–S419
Kawaguchi K, Taketomi S, Mizutani Y, Inui H, Yamagami R, Kono K, Kage T, Takei S, Fujiwara S, Ogata T, Tanaka S (2022) Dynamic postural stability is decreased during the single-leg drop landing task in male collegiate soccer players with chronic ankle instability. Orthop J Sport Med 10(7):23259671221107344
Mercer NP, Azam MT, Davalos N, Kaplan DJ, Colasanti CA, Chen JS, Kanakamedala AC, Dankert JF, Stone JW, Kennedy JG (2022) Anterior talofibular ligament augmentation with internal brace in the office setting. Arthrosc Tech 11(4):e545–e550
Michels F, Cordier G, Burssens A, Vereecke E, Guillo S (2016) Endoscopic reconstruction of CFL and the ATFL with a gracilis graft: a cadaveric study. Knee Surg Sports Traumatol Arthrosc 24(4):1007–1014
Michels F, Cordier G, Guillo S, Stockmans F (2016) Endoscopic ankle lateral ligament graft anatomic reconstruction. Foot Ankle Clin 21(3):665–680
Michels F, Pereira H, Calder J, Matricali G, Glazebrook M, Guillo S, Karlsson J, Acevedo J, Batista J, Bauer T, Calder J, Carreira D, Choi W, Corte-real N, Glazebrook M, Ghorbani A, Giza E, Guillo S, Hunt K, Karlsson J, Kong SW, Lee JW, Michels F, Molloy A, Mangone P, Matsui K, Nery C, Ozeki S, Pearce C, Pereira H, Perera A, Pijnenburg B, Raduan F, Stone J, Takao M, Tourné Y, Vega J (2018) Searching for consensus in the approach to patients with chronic lateral ankle instability: ask the expert. Knee Surg Sports Traumatol Arthrosc 26(7):2095–2102
Michels F, Matricali G, Guillo S, Vanrietvelde F, Pottel H, Stockmans F (2020) An oblique fibular tunnel is recommended when reconstructing the ATFL and CFL. Knee Surg Sports Traumatol Arthrosc 28(1):124–131
Pawik Ł, Pawik M, Wysoczańska E, Schabowska A, Morasiewicz P, Fink-Lwow F (2022) In patients with Grade I and II ankle sprains, dynamic taping seems to be helpful during certain tasks, exercises and tests in selected phases of the rehabilitation process: a preliminary report. Int J Environ Res Public Health. https://doi.org/10.3390/ijerph19095291
Takao M, Oae K, Uchio Y, Ochi M, Yamamoto H (2005) Anatomical reconstruction of the lateral ligaments of the ankle with a gracilis autograft: a new technique using an interference fit anchoring system. Am J Sports Med 33(6):814–823
Usuelli FG, Indino C, Di Silvestri CA, Manzi L, Maffulli N (2021) Clinical outcomes and return to sport after minimally invasive reconstruction of the lateral ligament complex with semitendinosus tendon autograft in chronic lateral ankle instability. J Am Podiatr Med Assoc. https://doi.org/10.7547/19-012
Vega J, Malagelada F, Manzanares Céspedes M-C, Dalmau-Pastor M (2020) The lateral fibulotalocalcaneal ligament complex: an ankle stabilizing isometric structure. Knee Surg Sports Traumatol Arthrosc 28(1):8–17
Vilá-Rico J, Cabestany-Castellà JM, Cabestany-Perich B, Núñez-Samper C, Ojeda-Thies C (2019) All-inside arthroscopic allograft reconstruction of the anterior talo-fibular ligament using an accesory transfibular portal. Foot Ankle Surg 25(1):24–30
Walt J, Massey P (2023) Peroneal tendon syndromes. StatPearls
Yang K-C, Chen P-Y, Loh C, Tzeng I-S, Chang S-M, Wang C-C (2022) Chronic lateral ankle instability treated with tendon allografting: a preliminary comparison of arthroscopic and open anatomic ligament reconstruction. Orthop J Sport Med 10(10):23259671221126692
Yokoe T, Tajima T, Yamaguchi N, Nagasawa M, Ota T, Morita Y, Chosa E (2021) Orthopaedic medical examination for young amateur athletes: a repeated cross-sectional study from 2014 to 2018. BMJ Open 11(1):e042188
Youn H, Kim YS, Lee J, Choi WJ, Lee JW (2012) Percutaneous lateral ligament reconstruction with allograft for chronic lateral ankle instability. Foot Ankle Int 33(2):99–104
Acknowledgements
Thank all participants of this study for their active participation and cooperation in this study.
Funding
This study was supported by Sun Yat-sen Clinical Research Cultivating Program (SYS-Q-202005) and Natural Science Foundation of Guangdong Province (2020A1515011322, 2022A1515010215).
Author information
Authors and Affiliations
Contributions
C-XL and Z-ZZ equally contributed to this study. C-XL and Z-ZZ put forward the conceptions of the work, conducted the experiments, and drafted the manuscript. BS, W-PL and PW made detailed designs of the work and revised the manuscript. J-SW assisted with revising the manuscript. Y-FZ and D-ZX assisted in the conduct of experiments. Y-FM, X-YL, T-YL and X-HD assisted with collecting experimental data and analysed data. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Conflict of interest
The authors have no relevant financial or non-financial interests to disclose.
Ethical approval
This is a cadaveric study. All experimental protocols are approved by the ethics committee of our hospital (No. SYSEC-KY-KS-2021-276). For this type of study, formal consent is not required.
Consent to participate
Not applicable.
Consent to publish
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Liu, CX., Zhang, ZZ., Wang, JS. et al. Optimal fibular tunnel direction for anterior talofibular ligament reconstruction: 45 degrees outperforms 30 and 60 degrees. Knee Surg Sports Traumatol Arthrosc 31, 4546–4550 (2023). https://doi.org/10.1007/s00167-023-07452-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-023-07452-6