
Abstract
Purpose
The purpose of the study was to evaluate the frontal gait patterns in patients with chronic patellofemoral instability compared to healthy controls. The hypothesis was that internal-rotation–adduction moment of the knee as altered dynamic Q-angle is evident in patients and correlates positively with increased femoral torsion.
Methods
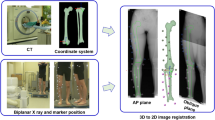
Thirty-five patients with symptomatic recurrent patellofemoral instability requiring surgical treatment were matched for average age, sex, and body mass index with 15 healthy controls (30 knees). Several clinical and radiographic measurements were taken from each participant: internal and external rotation (hipIR, hipER), Q-angle, tubercle sulcus angle (TS-angle), femoral antetorsion (femAT), tibial tubercle–trochlear groove (TT-TG) distance, and frontal leg axis. Additionally, three frontal gait patterns were defined and recorded: (1) internal-rotation–adduction moment of the knee during normal walking, (2) dynamic valgus of the knee, and (3) Trendelenburg’s sign in a single-leg squat. Randomized videography was evaluated by three independent blinded observers. Statistical analysis was performed using regression models and comparisons of gait patterns and clinical and radiological measurements. Furthermore, observer reliability was correlated to gradings of radiological parameters.
Results
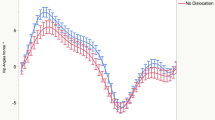
Patients showed altered dynamic Q-angle gait pattern during normal walking (p < 0.001) compared to healthy controls (interrater kappa = 0.61), whereas highest observer agreement was reported if femAT was greater than 20° (kappa = 0.85). Logistic regression model revealed higher femAT (18.2° ± 12.5 versus 11.9° ± 7.0 (p = 0.004) as a significant variable, as well as lower TT–TG distance (23.6 mm ± 2.8 vs. 16.6 mm ± 4.9, p = 0.004) on evident dynamic Q-angle gait pattern. Dynamic valgus in a single-leg squat was observed significantly more often in patients (p < 0.001) compared to controls (interrater kappa = 0.7). However, besides the static measured Q-angle as the only significant variable on evident dynamic valgus pattern (13.6° ± 4.6 vs. 10.3° ± 5.2, p = 0.003), no radiological parameter was detected to correlate significantly with dynamic valgus and Trendelenburg's sign (n.s.).
Conclusions
Clinical detection of pathologic torsion and bony alignment may be difficult in patients with patellofemoral instability. The present study demonstrated that dynamic Q-angle gait pattern is significantly altered in patients with chronic patellofemoral instability compared to healthy controls. Moreover, dynamic Q-angle correlates positively with higher femoral torsion and negatively with higher TT–TG distance. Therefore, clinical and radiological assessment of maltorsion should be added to the standard diagnostic workup in cases of patellofemoral instability.
Level of evidence
Level II.

Similar content being viewed by others

Data availability
Available from first author if asked.
References
Brattström H (1964) Shape of the intercondylar groove normally and in recurrent dislocation of patella: a clinical and X-Ray anatomical investigation. Acta Orthop Scand 35:1–148
Bruderer-Hofstetter M, Fenner V, Payne E, Zdenek K, Klima H, Wegener R (2015) Gait deviations and compensations in pediatric patients with increased femoral torsion. J Orthop Res 33:155–162
Claiborne TL, Armstrong CW, Gandhi V, Pincivero DM (2006) Relationship between hip and knee strength and knee valgus during a single leg squat. J Appl Biomech 22:41–50
Dickschas J, Harrer J, Pfefferkorn R, Strecker W (2012) Operative treatment of patellofemoral maltracking with torsional osteotomy. Arch Orthop Trauma Surg 132:289–298
Diederichs G, Kohlitz T, Kornaropoulos E, Heller MO, Vollnberg B, Scheffler S (2013) Magnetic resonance imaging analysis of rotational alignment in patients with patellar dislocations. Am J Sports Med 41:51–57
Feller JA, Amis AA, Andrish JT, Arendt EA, Erasmus PJ, Powers CM (2007) Surgical biomechanics of the patellofemoral joint. Arthroscopy 23:542–553
Franciozi CE, Ambra LF, Albertoni LJ, Debieux P, Rezende FC, Oliveira MA et al (2017) Increased femoral anteversion influence over surgically treated recurrent patellar instability patients. Arthroscopy 33:633–640
Graf KH, Tompkins MA, Agel J, Arendt EA (2018) Q-vector measurements: physical examination versus magnetic resonance imaging measurements and their relationship with tibial tubercle-trochlear groove distance. Knee Surg Sports Traumatol Arthrosc 26:697–704
Greene CC, Edwards TB, Wade MR, Carson EW (2001) Reliability of the quadriceps angle measurement. Am J Knee Surg 14:97–103
Gwynne CR, Curran SA (2018) Two-dimensional frontal plane projection angle can identify subgroups of patellofemoral pain patients who demonstrate dynamic knee valgus. Clin Biomech (Bristol, Avon) 58:44–48
Hinman RS, May RL, Crossley KM (2006) Is there an alternative to the full-leg radiograph for determining knee joint alignment in osteoarthritis? Arthritis Rheum 55:306–313
Imhoff FB, Cotic M, Liska F, Dyrna FGE, Beitzel K, Imhoff AB et al (2019) Derotational osteotomy at the distal femur is effective to treat patients with patellar instability. Knee Surg Sports Traumatol Arthrosc 27:652–658
Imhoff FB, Funke V, Muench LN, Sauter A, Englmaier M, Woertler K et al (2020) The complexity of bony malalignment in patellofemoral disorders: femoral and tibial torsion, trochlear dysplasia, TT-TG distance, and frontal mechanical axis correlate with each other. Knee Surg Sports Traumatol Arthrosc 28(3):897–904
Irger M, Achtnich A, Imhoff AB, Schmitt A (2020) Diagnosis and therapy of chronic patellofemoral instability. Orthopade 49:73–84
Kaiser P, Schmoelz W, Schoettle P, Zwierzina M, Heinrichs C, Attal R (2017) Increased internal femoral torsion can be regarded as a risk factor for patellar instability—A biomechanical study. Clin Biomech (Bristol, Avon) 47:103–109
Kibler WB, Press J, Sciascia A (2006) The role of core stability in athletic function. Sports Med 36:189–198
Kolowich PA, Paulos LE, Rosenberg TD, Farnsworth S (1990) Lateral release of the patella: indications and contraindications. Am J Sports Med 18:359–365
Liebensteiner MC, Ressler J, Seitlinger G, Djurdjevic T, El Attal R, Ferlic PW (2016) High femoral anteversion is related to femoral trochlea dysplasia. Arthroscopy 32:2295–2299
Livingston LA (2002) The accuracy of Q angle values. Clin Biomech (Bristol, Avon) 17:322–323 (author reply 323-324)
Nelitz M, Dreyhaupt J, Williams SR, Dornacher D (2015) Combined supracondylar femoral derotation osteotomy and patellofemoral ligament reconstruction for recurrent patellar dislocation and severe femoral anteversion syndrome: surgical technique and clinical outcome. Int Orthop 39:2355–2362
Paulos L, Swanson SC, Stoddard GJ, Barber-Westin S (2009) Surgical correction of limb malalignment for instability of the patella: a comparison of 2 techniques. Am J Sports Med 37:1288–1300
Post WR, Teitge R, Amis A (2002) Patellofemoral malalignment: looking beyond the viewbox. Clin Sports Med 21:521–546
Powers CM (2003) The influence of altered lower-extremity kinematics on patellofemoral joint dysfunction: a theoretical perspective. J Orthop Sports Phys Ther 33:639–646
Radler C, Kranzl A, Manner HM, Hoglinger M, Ganger R, Grill F (2010) Torsional profile versus gait analysis: consistency between the anatomic torsion and the resulting gait pattern in patients with rotational malalignment of the lower extremity. Gait Posture 32:405–410
Schmidt E, Harris-Hayes M, Salsich GB (2019) Dynamic knee valgus kinematics and their relationship to pain in women with patellofemoral pain compared to women with chronic hip joint pain. J Sport Health Sci 8:486–493
Schneider B, Laubenberger J, Jemlich S, Groene K, Weber HM, Langer M (1997) Measurement of femoral antetorsion and tibial torsion by magnetic resonance imaging. Br J Radiol 70:575–579
Schoettle PB, Zanetti M, Seifert B, Pfirrmann CW, Fucentese SF, Romero J (2006) The tibial tuberosity-trochlear groove distance; a comparative study between CT and MRI scanning. Knee 13:26–31
Seitlinger G, Moroder P, Scheurecker G, Hofmann S, Grelsamer RP (2016) The contribution of different femur segments to overall femoral torsion. Am J Sports Med 44:1796–1800
Smith TO, Hunt NJ, Donell ST (2008) The reliability and validity of the Q-angle: a systematic review. Knee Surg Sports Traumatol Arthrosc 16:1068–1079
Staheli LT, Corbett M, Wyss C, King H (1985) Lower-extremity rotational problems in children. Normal values to guide management. J Bone Joint Surg Am 67:39–47
Strecker W (2006) Planning analysis of knee-adjacent deformities. I. Frontal plane deformities. Oper Orthop Traumatol 18:259–272
Wallace DA, Salem GJ, Salinas R, Powers CM (2002) Patellofemoral joint kinetics while squatting with and without an external load. J Orthop Sports Phys Ther 32:141–148
Funding
Grant (FG-PRJ-418) from Deutsche Arthrose-Hilfe, 2018.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Imhoff FB received fees from mediCAD, Fa. Hectec, Germany, not related to this work. Cotic M: no conflict to report. Achtnich A: no conflict to report. Dyrna F: no conflict to report. Cote M receives personal fees from Arthroscopy Association of North America (AANA), outside the submitted work. Imhoff A is consultant for Arthrex Germany and medi Bayreuth, not related to this work. Beitzel K is consultant for Arthrex Germany.
Ethical approval
17/18S Technical University of Munich.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Investigation performed at Department of Orthopaedic Sports Medicine, Technical University, Munich, Germany.
Rights and permissions
About this article

Cite this article
Imhoff, F.B., Cotic, M., Dyrna, F.G.E. et al. Dynamic Q-angle is increased in patients with chronic patellofemoral instability and correlates positively with femoral torsion. Knee Surg Sports Traumatol Arthrosc 29, 1224–1231 (2021). https://doi.org/10.1007/s00167-020-06163-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-020-06163-6