
Abstract
Background
There is ongoing controversy as to the indications for and extent of lateral cervical lymphadenectomy for patients with papillary thyroid cancer (PTC). While most now agree that prophylactic lymph node dissections (LND) play no role, at the University of California, San Francisco (UCSF) we limit LND selectively on a level by level basis, and resect only the levels thought to harbor disease or to be at increased risk of metastases. This initial ‚selective LND’ usually includes levels III and IV (due to the well-documented increased likelihood of metastases to these levels) and levels I, II, and V are included when there is clinical or radiological evidence of disease or increased risk of it.
Methods
A retrospective review of the clinical charts and hospital records of 106 consecutive patients who had metastatic PTC and who underwent at least one lateral cervical LND at UCSF between January 1995 and December 2003 was carried out. Data were collected to assess which patients had levels I, II, and/or V included in their initial ipsilateral and/or contralateral LND and to determine the recurrence rates at these levels if they had previously been excised compared with if they had not. Chi-squared and Fisher exact tests were utilized for statistical comparison, where appropriate.
Results
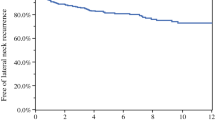
A total of 140 initial lateral LND were performed: 104 ipsilateral and 36 contralateral. In these initial LND, 3.9%, 72.5%, and 18.6% of patients had levels I, II, and V resected on the ipsilateral side, and 2.9%, 60.0%, and 37.1% of patients had levels I, II, and V resected on the contralateral side. Recurrence at levels I and V was uncommon in all patient populations. Recurrence at level II was 19% ipsilaterally and 10% contralaterally when the level was previously resected and 21% ipsilaterally and 14% contralaterally when the level was not previously resected. There was no statistically significant difference in recurrence at level II when the level had previously been resected compared with when it had not.
Conclusions
If utilized in the appropriate patient population, a selective approach to lateral cervical LND for PTC can be a successful alternative to the routine modified radical LND. Levels I and V do not require resection unless there is clinical or radiological evidence of disease. Guidelines for which patients may be considered for this less aggressive approach to level II nodal metastases are suggested.
Similar content being viewed by others


References
Kebebew E, Clark OH. Differentiated thyroid cancer: “complete” rational approach. World J Surg 2000;24:942–951
Robbins J, Merino MJ, Boice JD Jr., et al. Thyroid cancer: a lethal endocrine neoplasm. Ann Intern Med 1991;115:133–147
Bhattacharyya N. Surgical treatment of cervical nodal metastases in patients with papillary thyroid carcinoma. Arch Otolaryngol Head Neck Surg 2003;129:1101–1104
Caron NR, Clark OH. Papillary thyroid cancer: surgical management of lymph node metastases. Curr Treat Options Oncol 2005;6:311–322
Sivanandan R, Soo KC. Pattern of cervical lymph node metastases from papillary carcinoma of the thyroid. Br J Surg 2001;88:1241–1244
Kupferman ME, Patterson M, Mandel SJ, et al. Patterns of lateral neck metastasis in papillary thyroid carcinoma. Arch Otolaryngol Head Neck Surg 2004;130:857–860
Caron NR, Clark OH. Well differentiated thyroid cancer. Scand J Surg 2004;93:261–271
Machens A, Hinze R, Thomusch O, et al. Pattern of nodal metastasis for primary and reoperative thyroid cancer. World J Surg 2002;26:22–28
Cheah WK, Arici C, Ituarte PH, et al. Complications of neck dissection for thyroid cancer. World J Surg 2002;26:1013–1016
Mann B, Buhr HJ. Lymph node dissection in patients with differentiated thyroid carcinoma—who benefits? Langenbecks Arch Surg 1998;383:355–358
Shaha AR. Prognostic factors in papillary thyroid carcinoma and implications of large nodal metastasis. Surgery 2004;135:237–239
Musacchio MJ, Kim AW, Vijungco JD, et al. Greater local recurrence occurs with “berry picking” than neck dissection in thyroid cancer. Am Surg 2003;69:191–196; discussion 196–197
Wada N, Duh QY, Sugino K, et al. Lymph node metastasis from 259 papillary thyroid microcarcinomas: frequency, pattern of occurrence and recurrence, and optimal strategy for neck dissection. Ann Surg 2003;237:399–407
Takami H, Sasaki K, Ikeda Y, et al. Detection of sentinel lymph nodes in patients with papillary thyroid cancer. Asian J Surg 2003;26:145–148
Fukui Y, Yamakawa T, Taniki T, et al. Sentinel lymph node biopsy in patients with papillary thyroid carcinoma. Cancer 2001;92:2868–2874
Noguchi S, Murakami N. The value of lymph-node dissection in patients with differentiated thyroid cancer. Surg Clin North Am 1987;67:251–261
Noguchi S, Noguchi A, Murakami N. Papillary carcinoma of the thyroid. I. Developing pattern of metastasis. Cancer 1970;26:1053–1060
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Caron, N., Tan, Y., Ogilvie, J. et al. Selective Modified Radical Neck Dissection for Papillary Thyroid Cancer—Is Level I, II and V Dissection Always Necessary?. World J. Surg. 30, 833–840 (2006). https://doi.org/10.1007/s00268-005-0358-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-005-0358-5