
Abstract
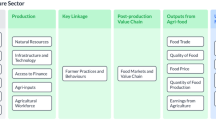
The second goal of Sustainable Development Agenda set in 2015 by the United Nations General Assembly seeks to end hunger and all forms of malnutrition, and double agricultural productivity by 2030. It has been laid down that sustainable access to nutritious food would require sustainable agricultural production and practices. The pathways through which agriculture affects nutritional outcomes have been well-documented; the linkages operate through improving access to food, affecting agricultural incomes and prices, and ‘feminising’ the agricultural workforce.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others

1 Introduction
The second goal of Sustainable Development Agenda set in 2015 by the United Nations General Assembly seeks to end hunger and all forms of malnutrition, and double agricultural productivity by 2030. It has been laid down that sustainable access to nutritious food would require sustainable agricultural production and practices. The pathways through which agriculture affects nutritional outcomes have been well-documented; the linkages operate through improving access to food, affecting agricultural incomes and prices, and ‘feminising’ the agricultural workforce (Gillespie & Kadiyala, 2011; Kadiyala et al., 2012). An important pathway from agriculture to nutrition operates through the increased empowerment of women. Increasing feminization of agricultural labour empowers women and enables them to exercise greater bargaining power in household decision-making. This in turn leads to better health and nutrition for women and children. Recent literature highlights the need to empirically examine this pathway in India (Rao & Pingali, 2018). Comparison and validation of various measures and concepts of women’s empowerment merit attention both from academic and policy perspectives.
Undernutrition among women in India is higher than that in many Sub-Saharan African countries that are poorer and have lower rates of growth (Coffey, 2015). Moreover, nutrition of women in India is characterized by the ‘dual burden’; while the proportion of underweight women has been declining, that of overweight and obesity has been increasing, even among the poor and in rural areas. Data shows that health and nutrition outcomes for women and children have been systematically worse in rural India. The percentage of underweight women was 22.9 at all-India level and 26.7 in the case of rural areas in 2015–16. At the national level, 20.6% of women were overweight. The corresponding figure was 15% for rural India. While the percentage of underweight women declined, the percentage of overweight women increased in both rural and urban India between 2005–06 and 2015–16. The latest round of NFHS, which was conducted in the year 2019–20, shows the same trend for most of the states for which the figures are available.
Studies have shown that health outcomes vary systematically across different dimensions of social power (such as sex, region of residence, religion, caste, and class) and their intersections in India (Mukhopadhyay, 2015, 2016; Sen et al., 2009). Intersectional inequality, a notion that was popularized within the realm of feminist studies, has only recently captured the attention of quantitative enquiries. Different dimensions of social power have been shown to simultaneously interact in a complex web, with an individual being placed at a mix of advantages and disadvantages that are associated with different identities. It has been shown that nutrition in India is characterized not only by single-axis inequalities but also by intersectional inequalities (Mukhopadhyay & Chakraborty, 2018).
This study intends to focus on women in agricultural households and examine how their empowerment varies across the social spectrum. It asks how the intersections of the different dimensions of social power shape empowerment outcomes of women belonging to agricultural households. We measure empowerment using three indices, the Survey-based Women's emPowERment index (SWPER) (Ewerling et al., 2017), Index of Women’s Empowerment (IWE) and the Index of Women’s Empowerment in Nutrition (IWEN). While the first is a concise measure using fewer items, the second is more conventional and uses a larger number of items. The third includes many more items and is formulated following recent studies pointing out the need for a nutrition-focused index of women’s empowerment. Recent literature has shown how the traditional indicators of women’s empowerment fail to uncover the relationship between women’s intra-household status and child nutrition. The construction of IWEN draws heavily from the Women’s Empowerment in Nutrition Index, which tries to capture the processes that enable women to be well-nourished and healthy and has been shown to be a better indicator than the conventional measures (Narayanan et al., 2019).
The paper also intends to conduct validation exercises by examining how women’s empowerment is associated with their health in agricultural households, given their intersectional positionalities in the social spectrum. We use unit-level data from India Human Development Survey (IHDS) 2012 and ask if using the more comprehensive and nutrition-focused indicator of women’s empowerment yields additional insights.
The next section briefly discusses the relevant literature. The third section discusses the data and the methods. The fourth section discusses the results and the fifth section concludes the paper.
2 Background
This paper refers to two sets of literature, which use both theoretical and empirical methods. The first comprises studies which seek to understand if benefits leveraged from advantageous social positions can offset or are offset by the disadvantages stemming from other simultaneous social positions. While comparison of outcomes of the extreme social groups (for instance non-poor upper caste and poor backward caste) often lead to expected results, studying the middle part of the social spectrum often yields interesting findings. Also, one may question if social group affiliation, such as caste-identity plays a significant role within a particular class or vice versa. Quantitative attempts to understand these processes comprise frontier literature in social sciences.
The second set of literature that this study refers to engages with the notion of women’s empowerment. Recent studies have proposed newer methods of measuring women’s empowerment. This paper aims to understand the agriculture–nutrition pathways operating through the channel of women’s empowerment, at the intersections of the different axes of social power.
2.1 Intersectional Inequality
While the importance of identities associated with particular group affiliations is irrefutable with regard to well-being (in our context health) outcomes, the complex interactions of multiple identities have also attracted scholarly attention, particularly within the realm of feminist studies (Davis, 2008). Different axes of social power, such as gender, economic class, ethnicity, and caste are often simultaneously operative, with significant interactions among each other. Crenshaw (1989) coined the term ‘intersectionality’ to capture the multifaceted discriminations (associated with gender and race) faced by Black women to defy to the ‘single-axis framework’ that implicitly assumed all women to be White and all Blacks to be men. A growing body of research has addressed the issue of intersectionality (Weber & Parra-Medina, 2003), mostly adopting qualitative methodologies. Sen et al. (2009) have devised a simple and powerful methodology for quantitative analysis of the interactions of different axes of social power. Using this method, recent literature has asked important questions to analyse multidimensional inequalities in healthcare-seeking behaviour of individuals (Iyer et al., 2007; Sen & Iyer, 2012; Sen et al., 2007, 2009). Rigorous statistical testing has helped identify the varying importance of different social inequalities in different social settings.
Mukhopadhyay and Chakraborty (2018) point out that in India child undernutrition is characterized by an absent sex gap, though the country is infamous for gender disparity, reflected in indicators such as sex ratio, child mortality, and son preference. They invoke the framework of intersectionality to investigate the variations in the nutritional status of children across the intersections of the two axes, sex, and caste.
2.2 Alternative Ways of Measuring Women’s Empowerment
The conceptual framework for computing women’s empowerment put forth by Kabeer (1999) paved the way for most of the work in this realm. The framework consists of three interlinked dimensions: resources, agency, and achievements. Resources are referred to as the preconditions or endowments which help in facilitating women’s empowerment. This includes economic resources and human and social resources, which strengthen the capacity to make choices. The dimension of agency is defined as: ‘the ability of the woman to define her goals and act upon them, often measured through decision-making power’. (Kabeer, 1999). Finally, the achievements are defined as: ‘the extent to which potential is realised and whether it has transformative power’ (Kabeer, 1999, 2005).
One of the recent applications of this framework to formulate a measure of women’s empowerment can be found in the WEI Report (UNICEF, 2020). It has considered four domains pertaining to the resources and agency. The domains are Economic Domain, Human and Social Resources, Household and Sexual/Reproductive Decision-Making, and Attitude towards Socio-Cultural Norms. The first two domains are associated with the resources component, whereas the last two are related to the agency component of empowerment.
Ewerling et al. (2017) formulate a parsimonious index of women’s empowerment, Survey-based Women's emPowERment index (SWPER) using only 15 survey questions in three domains: social independence, decision-making, and attitude to violence. This index has been validated and shown to reflect the effect of empowerment on health outcomes better than other indices in low- and middle-income countries (Ewerling et al., 2020). This index can be conveniently constructed and used for cross-sectional and temporal comparisons.
The recently formulated Women’s Empowerment in Nutrition Index (WENI) emphasizes that women’s nutritional statuses matter in their own right (Narayanan et al., 2019). This framework identifies four dimensions of nutritional empowerment: resources, agency, achievement, and knowledge. The first three dimensions are derived from the conceptual framework of Kabeer (1999). Knowledge, resources, and agency are the dimensions of empowerment and would be used in computing WENI. There are three domains relevant to nutritional empowerment—food, health, and institutions. Another sub-domain, fertility, is incorporated in the list as a critical aspect of nutritional empowerment for women of reproductive age.
This paper uses three indices of women’s empowerment (details provided in the next section), similar to the ones described above, and explores how they are associated with intersectional positionalities of women in agricultural households. It then examines how these indices predict women’s BMI status, controlling for religion, caste, and class, and their intersections.
3 Data and Methods
3.1 Data
We use unit-level data from the second round of the India Human Development Survey (IHDS), a nationally representative panel survey, conducted jointly by the National Council of Applied Economic Research (NCAER) and the University of Maryland. So far, two rounds of IHDS have been conducted. IHDS-1, conducted in 2004–05, covered 41,554 households 1503 villages, and 971 urban neighbourhoods across India. The second round of IHDS re-interviewed most of these households in 2011–12. IHDS-2 covered 42,152 households in 1420 villages and 1042 urban neighbourhoods throughout India. There is an 85% re-interview rate between two surveys. IHDS-1 and 2 were designed to complement existing Indian surveys by covering a wide range of topics in a single survey. It covered topics concerning health, education, employment, economic status, marriage, fertility, gender relations, social capital, village infrastructure, wage levels, and panchayat composition. The data provides information on female members of the household belonging to the age range of 15–80 years. Since this paper intends to study the agriculture–nutrition pathway operating through women’s empowerment, the analysis is conducted only on women from households associated with agriculture. Thus, the analysis has been restricted to 15,688 women.
3.2 Methods
This paper understands class as economic class. Households are divided into quintiles of per capita income and the bottom two quintiles are considered poor. Class has been constructed as a dichotomous variable, with the three upper quintiles labelled ‘non-poor’. Social group affiliation is defined by intersecting religion and class. We consider seven social groups. The caste-based Hindu society is divided into Brahmins, Forward Castes, Other Backward Castes, Scheduled Castes and Scheduled Tribes. The other two social groups are Muslims and ‘Other Religions’. The latter have been clubbed together because of small sample size. The control variables used in our regression exercises are woman’s age, marital status, and number of household members. In the last block of Table 4, we consider the intersectional groups. To limit the number of groups and to facilitate interpretation, we club Brahmins, Forward Castes, and OBCs as Upper Castes (UC). We thus have five social groups (UC, SC, ST, Muslims, and Other Religions), two economic classes (poor and non-poor), and ten intersectional categories across the axes of social group affiliation and economic class (details in Table 5).
3.2.1 Construction of SWPER
Ewerling et al. (2017) have constructed a parsimonious index of women’s empowerment using 15 items, easily available in household surveys like the Demographic and Health Surveys. Most of the items are available in IHDS. The questions on attitude to wife-beating have been replaced with the question asking if wife-beating on the particular grounds was common in the community (Tables 1, 2, and 3).
Using these indicators, principal components analysis is conducted, following Ewerling et al. (2017). After an examination of the scree plot, the third component is taken to be SWPER.
3.2.2 Construction of IWE
This study uses a similar framework as the report by UNICEF (2020) in order to construct the IWE. Pertinent variables from the data were identified and added to each domain. An empowerment cut-off was set for each indicator; an individual having a value below the empowerment threshold was considered to be disempowered. Then, the variables were converted to binary variables and assigned the value of 1, indicating empowered, or 0, indicating disempowered.
Economic domain:
The WEI report included two indicators in this domain: paid employment and house or land ownership. IHDS has variables pertaining to these two indicators. IHDS asks if a woman is currently working for pay/wages. Home or land ownership is represented in IHDS by asking if a woman has her name enlisted on the ownership or rental papers for her home. Also, IHDS provides information on whether or not a woman’s name is on any bank account. This too is added to the economic domain. A woman is considered empowered in the indicator of ownership if she has her name on rental papers or any bank account.
Human and social resources:
In the original framework, this domain is represented by educational attainment, exposure to media, exposure to family planning, knowledge about modern contraception, knowledge about access to contraception, and knowledge about HIV/AIDS. Educational attainment can be found as years of education completed in IHDS. The variable is continuous but has been reconstructed as a binary variable based on a cut-off value in which a woman is considered empowered if she has completed primary education. How often women in a household read a newspaper is taken into consideration for the indicator on exposure to media. A woman is considered disempowered if she never reads the newspaper and anything otherwise is considered to empowering. IHDS does not provide any information regarding access to family planning information directly. However, it asks the women if they have any knowledge about post-sterilization weakness in men. This has been used as a proxy for the access to family planning information indicator. A woman is considered empowered if she has apt knowledge about it, if she is aware of the fact that sterilization does not cause weakness in men. IHDS asked a woman about what method of contraception she was using to prevent or delay pregnancy. This has been used for the indicator of knowledge about modern methods of contraception. A woman is considered empowered if she uses any kind of contraceptive method and disempowered if she does not use anything. IHDS enquired about what method of contraception the woman was using. This has been used for the indicator of knowledge about access to contraception. A woman is considered empowered if she uses condom. It is assumed that if she uses the method, she has knowledge about how to access it. IHDS provides information on whether or not a woman is aware of HIV/AIDS. This has been used for the indicator of knowledge about transmission of HIV/AIDS. A woman is considered empowered if she has heard of it and disempowered if she is not aware of the illness.
Household and sexual/reproductive decision-making:
From WEI Report (2020), the indicators for this domain include birth spacing and limiting, decision-making power on large household purchases, own health care, visiting family or relatives, husband/partner’s earnings, ability to refuse sex, and freedom/ability to ask partner to use condom during sexual intercourse. IHDS asks a woman if she has any say in the number of children she wants to have. This is an indicator for the say in birth spacing and limiting. A woman is considered empowered if she has a say in the number of children she wants to have. For the next four indicators of decision-making power on large household purchases, own health care, vising family and husband/partner’s earnings, IHDS provides information on whether or not a woman has a say in buying expensive items for the household (T.V., Fridge)/land or property, what to do when she falls sick, she needs to ask for permission before visiting relatives or friends and if she discusses with her husband about what to spend money, respectively. A woman is considered empowered if she can make decisions herself or jointly with her partner or does not need to take permission and disempowered if she does not have a say in any decision-making process. No data concerning the last two indicators could be found in IHDS. Thus, these two were not incorporated into the index.
Attitude towards socio-cultural norms and phenomena:
This domain has six indicators: whether the woman justifies wife beating in the following five situations (1) if she goes out without telling him, (2) if the wife neglects the children, (3) if the wife argues with the husband, (4) if the wife refuses to have sex with the husband, (5) if the wife burns food. Information on the woman’s attitude to wife beating is not available in IHDS data. IHDS has asked if wife-beating is common at the community level due to certain reasons, namely, if it is usual for the husband to beat his wife when she goes out without telling him, when she neglects the house or children, when the wife does not respect elders in the family, when she is suspected of having relation with other men. A woman is considered empowered if she is not used to wives getting beaten up in her community in the aforesaid situations and considered disempowered otherwise.
Using these indicators, principal components analysis is conducted, following Ewerling et al. (2017), so that the indices are comparable. After an examination of the scree plot, the third component is taken to be IWE.
3.2.3 Construction of IWEN
Following this framework of Narayanan et al. (2019), we have seven domain-dimensions (D-D) for women and ten for women of reproductive age. For each D-D, relevant indicators are identified, modified, and incorporated in the formulation of the index. An empowerment cut-off was set for each indicator, women having a value below the empowerment threshold were considered to be disempowered. Then, the variables were converted to binary variables and assigned the value of 1, indicating empowered, or 0, indicating disempowered. The D-D-specific variables are discussed elaborately as follows:
Food:
Food Knowledge: It includes knowledge of calcium and iodine. IHDS does not provide any information on this. However, it has information on whether or not a woman has any knowledge about the impact of the smoke from wood/dung burning traditional chulha. This has been used as a proxy indicator of health knowledge. A woman is considered empowered if she is aware of the fact that the smoke is harmful and disempowered if she has no knowledge about it. In addition to this, two more relevant indicators were added to this D-D from IHDS data. It also provides information on awareness regarding drinking milk (1–2 glasses every day) during pregnancy and the first yellow milk that comes out post-delivery of a child. A woman is considered empowered if her answer to these questions is correct.
Food Resources: Originally this D-D includes nine indicators: does paid work, participation in non-agriculture, participation in agriculture, aid for crop and livestock production, financial support for business, access to food aid and employment scheme, asset owned by individual, no imposed dietary restrictions and eating together. IHDS provides information on whether woman has her name on rental papers or any bank account. This has been used for the indicator of asset ownership. A woman is considered empowered if she has any bank account or has her name on ownership or rental papers of her home. IHDS provides information on the dietary practices of the household members. It asks if any member of the household consumes non-vegetarian food items. This has been used as a proxy for dietary restrictions. IHDS provides information regarding the eating order of household members. It is considered to be empowering when all the family members eat together and the woman eating last is disempowering.
Food Agency: This D-D includes six indicators: say in cultivation decision, kitchen garden production, major/minor decision regarding household enterprise, rent or sell of own asset, expenditure of own contribution to income, and purchasing food items. Say in cultivation decision is represented by whether or not the wife discusses with the husband about the things that happen on farm/work. A woman is considered empowered if she discusses farm/work-related things with her husband. Say in kitchen garden production could not be included because IHDS does not provide any information on the same. IHDS provides information on whether or not a woman has a say in the decision of how much money to spend on social functions such as marriage, to buy an expensive item such as TV, fridge, and land or property. These are used as proxies for say in major/minor decisions regarding household enterprise and rest or sell off own assent. A woman is considered empowered if she has a say in the decision-making process in the aforementioned situations. IHDS asks who has the most say in decisions about a woman’s work and this has been used as a proxy for expenditure of own contribution to income. A woman is considered empowered if she herself has the most say in the decision regarding her work and disempowered if others make the decision for her. IHDS provides information on who does the food and vegetable shopping in the household and this is used as a proxy for the indicator of say in purchasing food items. A woman is considered empowered if she herself does the vegetable shopping assuming that this would mean she has a say in purchasing food items for the house. Three additional indicators were added to this D-D: say in livestock production, farm decision, and what to cook on daily basis. IHDS provides information on whether or not a woman has any say in decision regarding livestock production and farm-related work. IHDS also provides information on whether or not the woman has any say in deciding what to cook on daily basis. A woman is considered empowered in all of the three indicators if she has any say in the decision-making process related to livestock production, farm work, and cooking.
Health:
Health Knowledge: This includes: knowledge of anaemia, ORS, and Malaria. IHDS does not provide any information on anaemia and it has been dropped from the D-D. How much should be given to drink when children have diarrhoea is used for the indicator of knowledge of ORS. A woman is considered to be empowered, that is, has ORS knowledge, if she knew that more than usual quantity of drinks were to be given during diarrhoea. IHDS also provides information on whether or not a woman is aware of what illness spreads through drinking impure water -TB, Typhoid, or Cancer. This too is included in this D-D. How malaria spreads is used for the indicator of knowledge of malaria.
Health Resources: The D-D includes questions asking if the woman does no activity, paid or unpaid, which is heavy, does no activity, paid or unpaid, with risk of injury or health problems, has help with domestic and care work, was not ill in past 30 days (chronic or otherwise) or sought treatment when ill, has help with housework when ill, has access to improved water, sanitation, and smoke-free kitchen. There is no data available related to the first two indicators in IHDS. IHDS provides information on whether or not a household employs any help or servants for cleaning, cooking, and childcare. This has been used for the indicator of household help. For the indicator of treatment-seeking when ill, information regarding treatment seeking behaviour of an individual in case of major morbidities in the last 12 months from IHDS has been used. A woman is considered empowered if she receives any treatment or advice from the doctor. The rest of the indicators were dropped from the computation of the index due to the lack of data availability.
Health Agency: This D-D includes indicators on if a woman can go alone to the health care centre, does not need to take permission for going to healthcare centre, and can take decision on own health. These are represented by the respective indicators from IHDS, if a woman can go alone to the health centre, and if she has any say in the decision about what to do when she falls sick. A woman is considered empowered if she can go alone or does not have to ask for permission before going to the health centre and also if she herself has a say in deciding what to do when she falls sick. Another relevant indicator from IHDS data was added to this D-D: If a woman has any say in deciding what to do when her child falls sick. A woman is considered empowered if she has a say in what to do in case her child falls sick. For the indicators of access to improved water and sanitation, IHDS has information regarding the household’s accessibility to water and toilet. A woman is considered empowered if the household has access to water and toilet facilities. Access to smoke-free kitchen has been represented by two pertinent variables from IHDS. It provides information on what kind of chulha a household uses and if there is a window or vent in the cooking area. A woman is considered empowered in these indicators if she has access to a kitchen with chimney and if there is a window or vent present in the kitchen area.
Institutions:
This D-D includes seven indicators: membership (member or non-membership of groups out of their own volition), access to information about government schemes, intimate partner violence: freedom of movement, no risk of sexual harassment in paid or other work, veil use, and public/civic engagement.
IHDS provides information on whether or not a woman is a member of mahila mandal/SHG/credit or saving group/political organization. A woman is considered empowered if she is associated with any of the groups. Information on access to information about government schemes is not available in the IHDS dataset and is dropped from the calculation.
Intimate partner violence is represented by a series of questions in IHDS: if it is usual in the community for the husband to beat his wife if she goes out without telling him/having relation with other men/natal family does not give money or jewellery/neglects the house or children/does not respect elders of the family/does not cook properly. A woman is considered to be empowered if she finds it unusual when the husband beats the wife in the aforementioned situations. IHDS provides information on whether or not a woman can go alone to the home of relatives or friends/kirana shop/short distance by train or bus. These are used for the indicator of freedom of movement. A woman is considered empowered if she can go to these places alone. There is no information available workplace harassment in IHDS. However, the data provides information on how frequently are unmarried girls harassed in your village or neighbourhood. This has been used as a proxy for sexual harassment at workplace. It is considered to empowering when unmarried girls are rarely harassed in the village or neighbourhood.
IHDS provides information on whether or not a woman practices any sort of veil: ghunghat/burkha/purdah/pallu. A woman is considered to be empowered if she does not practice any kind of veil. Finally, whether or not a woman has attended public meeting/gram sabha/nagarpallika/ward committee in the last year has been taken into consideration for the indicator of public or civic engagement. A woman is considered to be empowered if she engaged herself in any of these pubic or civic meetings.
Fertility:
Fertility Knowledge: The D-D is represented by two indicators: knowledge of menstrual cycle and pregnancy and knowledge of different diets during pregnancy. IHDS provides information on whether or not a woman has adequate knowledge about menstrual cycle and pregnancy. It asks a woman if she knows in which part of her menstrual cycle she is most likely to get pregnant.
Fertility Resources: The D-D includes Ability to secure an adequate, appropriate, and diverse diet during pregnancy, if the woman did not undertake heavy physical activity after the eighth month of pregnancy, did not do heavy physical activity after a month of delivery, received support in housework during pregnancy, had at least one antenatal check-up and at least one postnatal check-up. IHDS provides information on whether or not a woman received any meals from ICDS and this has been used as an indicator of ability to secure adequate diet during pregnancy. IHDS does not provide any information pertinent to the next three indicators. Thus, they have been dropped from the index. IHDS has information on antenatal and postnatal check-up. A woman is considered empowered in these two indicators if she receives any antenatal and postnatal check-ups.
Fertility Agency: The D-D includes four indicators: say in use/not use of contraceptives, say in the choice of facility for delivery, say in total no of children, say in spacing of children. Say in use/not use of contraceptives is obtained from the IHDS variable which provides information on whether or not a woman and her husband is using any method of contraception. Assuming that she has a say in it (empowered) if the couple is currently using any method of contraception. IHDS also asks who motivated a woman to go to the health facility for delivery. A woman is considered to have a say in the choice of facility for delivery if she herself is the motivator. IHDS asks a woman if she has any say in the number of children she wants to have. This is an indicator for the say in total number of children a woman wants to have. A woman is considered empowered if she has a say in the number of children she wants to have. IHDS also provides information regarding a woman’s preference on when to have the next child and this is considered an indicator for say in spacing of children. A woman is considered to be empowered if she has any preference in this matter.
Using these indicators, principal components analysis is conducted, following Ewerling et al. (2017), so that the indices are comparable. After an examination of the scree plot, the third component is taken to be IWEN.
3.2.4 Econometric Analysis
Following Sen et al. (2009) and Mukhopadhyay and Chakraborty (2018), this study will use the regression approach to capture intersectionality quantitatively. This method has been pioneered in the last decade as a simple and elegant tool to capture intersectionality quantitatively (Sen et al., 2009). The method requires creation of a set of dummy variables for each intersecting category. With two dimensions, for example, economic class (categorized into poor and non-poor) and caste (taken as a dichotomous variable, with two castes, backward and other), there would be four categories in the heuristic matrix: d1 = poor backward caste; d2 = non-poor backward caste, d3 = poor, other caste and d4 = non-poor other castes. The differences between the dummies can be then tested using regression, where empowerment status is regressed on a list of covariates and these intersectional dummies. We run quantile regression since the empowerment scores have asymmetric distributions.
For the second research question (how empowerment is associated with women’s BMI status), we include these intersectional dummies as covariates in an ordered logistic model. The dependent variable is BMI status (grouped into three categories, underweight normal, and overweight) and the woman’s empowerment scores (SWPER, IWE, and IWEN) are used as regressors in three different models.
4 Results and Discussion
We discuss our findings on the factors associated with IWE and IWEN in the agricultural households of rural India. We examine if the statistical significance of social group affiliation, class, and intersectional positionalities differs when we use the nutrition-specific indicator of women’s empowerment. We also intend to see if the pattern of association between women’s empowerment and caste, class, and their intersections differs across the distribution of empowerment.
Another objective of the paper is to find out if the two indices differentially affect maternal health, measured in terms of body mass index. We examine this by controlling for the positionalities along social group affiliation and class.
4.1 The Correlates of Women’s Empowerment
Following the method outlined in Sect. 3, SWPER, IWE, and IWEN are taken to be the third components after an examination of the scree plots following the respective principal component analysis. Figures 1, 2, and 3 represent the Kernel Density Plots of SWPER, IWE, and IWEN respectively. While SWPER has a bimodal distribution with a median score of 0.04, IWE and IWEN both have multimodal, positively skewed distributions, with median scores of −0.12 and 0.01, respectively.

Source: Author’s calculations from NFHS unit-level data
Kernel density plot of SWPER

Source: Author’s calculations from NFHS unit-level data
Kernel density plot of IWE

Source: Author’s calculations from NFHS unit-level data
Kernel density plot of IWEN
The nature of the distributions suggests that quantile regression may have its advantages over OLS regression, when we intend to find out the correlates of empowerment of women. We also intend to see if the degree of association of a correlate (particularly the caste-class intersections) vary across the distribution of empowerment.
The Association of Religion, Caste, Class, and their Intersections with SWPER
Table 4 shows that women from poorer agricultural households have lower SWPER scores. However, compared to Brahmins, all other social groups have significantly higher SWPER scores. Testing the differences within categories, we find that women from backward castes and Muslim women do not have significantly different scores compared to Non-Brahmin Forward Castes and OBCs. There is a large body of literature which suggests that women from Brahmin households may be less empowered (Chakravarti, 2018/2003). The institution of Brahmanical patriarchy operates by upper caste women subjecting themselves to dominance, since they often have greater stakes in the market and lesser fallback options outside the marriage. Mukhopadhyay (2016) has shown that while a significant sex disparity is absent in child nutrition in India, girls from upper caste households are more likely to be stunted than boys.
Model 2 in Table 4 shows that among the intersectional groups, women from poor Scheduled Tribe households and poor upper caste households have significantly lower empowerment than the reference group comprising non-poor upper caste women. While within Scheduled Castes and Scheduled Tribes, poor women are less empowered than non-poor women, there is no significant class advantage among Muslims.
When we model the conditional quartiles, we find that our major results remain unaltered for the first and third quartiles (results not reported).
The Association of Religion, Caste, Class, and their Intersections with IWE
Table 4 shows the results of the quantile regression of IWE. Model 1 shows that controlling for age, marital status, and household size of women, we find that the poor have significantly lower IWE scores than the non-poor. However, once we consider IWE instead of SWPER, Brahmins have significantly higher empowerment scores than all other social groups, except Non-Brahmin forward caste Hindus and ‘Other Religions’. This may be because IWE includes a longer list of items pertaining to resource and access. We test the statistical significance of the differences between the other social groups and find that Scheduled Tribe women have significantly lower IWE scores than Scheduled Caste and Muslim women.
Model 2 shows how IWE differs across the caste-class intersections. We find that all the intersectional categories have significantly lower IWE scores compared to non-poor upper castes. We also find that within each social category in the caste-based Hindu society and within Muslims, there are significant class differences, with the non-poor having significantly higher IWE than the poor. This result, however, does not hold for the ‘Other Religions’.
Quantile regression shows that class and social group affiliation have similar patterns of association with IWE along the distribution of IWE. To wit, the non-poor and the Upper Caste Hindus have significantly higher IWE scores both at the first and the third quartiles of IWE. As in the case of the median regression, when we model the conditional quartiles, we find that the last result does not hold for ‘Other Religions’. Again, at both the first and third quartiles, we find that within each social group, the class difference is significant (results not reported).
Using IWEN as the Regressand
Table 4 also shows the results of quantile regression of IWEN. Model 1 shows that when we consider the nutrition-specific index of women’s empowerment instead of the general index, the class advantage is retained. Compared to women from poor agricultural households, those from non-poor agricultural households are more likely to be nutrition-empowered. The results with respect to social group affiliation are also similar to that for IWE, presumably due to the same reason.
The main findings regarding the significance of the intersectional positionalities of women in agricultural households remain unaltered when we consider IWEN scores instead of IWE scores as the regressand. Again, modelling the conditional quartiles of IWEN instead of IWE, we find that the results remain unchanged (not reported).
Robustness Checks
We run OLS regressions of SWPER, IWE, and IWEN using the same set of covariates and see that our findings are robust (results not reported).
4.2 The Association Between Women’s Empowerment (SWPER, IWE, and IWEN) and Health
Controlling for women’s age, marital status, number of household members, class, and caste, we find that a lower SWPER score is associated with a higher likelihood of a woman in an agricultural household being underweight (Table 5). Likewise, a higher SWPER score is associated with a higher likelihood of being overweight and obese. Poorer women and women from SC and ST households are more likely to be underweight and less likely to be overweight.
Irrespective of how we choose to measure empowerment (using IWE or IWEN instead of SWPER), we find that women with higher empowerment scores in agricultural households are less likely to have a body mass index below the cut-off level. However, they are the ones who have a greater likelihood of being overweight and obese. It is somewhat surprising that even IWEN, the nutrition-specific indicator of women’s empowerment, which includes domains like food knowledge is positively associated with the likelihood of being overweight or obese.
Robustness Check
We check the association of the empowerment scores with BMI, taken as a continuous indicator, and find that our results are robust (results not reported).
Explaining Morbidity
As an additional exercise in validation of the empowerment indices, we also check the association of the empowerment indices and find that all three are significantly associated with the likelihood of being indisposed for more than 15 days in a year. To wit, a woman with higher empowerment scores (according to all three indices) is less likely to be suffering from a chronic ailment due to which she was indisposed for more than 15 days during the last year. This strengthens our scepticism regarding the usefulness of more elaborate measures of measurement for empirical evaluations (Table 6).
5 Conclusion
This study shows that the choice of the index of women’s empowerment may be crucial to the substantive conclusions. Caution needs to be exercised by policymakers and analysts when they choose an index as the summary measure of women’s status. This paper finds that SWPER is higher for women from backward castes, compared to those from Brahmin agricultural households, corroborating the findings of historical and sociological studies on the operations of Brahmanical patriarchy. However, this finding no longer remains once SWPER is replaced by alternative and broader indices like IWE and IWEN. This may be because the latter includes a number of items on access and resource, which are compromised for disadvantaged social groups.
With respect to the association of women’s empowerment with their health in agricultural households, the three indices lead to an unambiguous result: body mass index is significantly higher for women with higher empowerment scores. It is somewhat surprising that the likelihood of being overweight and obese is higher for women with higher IWEN, just as it is with SWPER and IWE. Higher scores of IWEN, the nutrition-specific index, which includes domains like food knowledge, are not associated with lower likelihoods of being overweight and obese. Likewise, all three indices are associated with the likelihood of a woman being indisposed due to a chronic morbidity. We thus question, if we should use more parsimonious indices like the SWPER, since it has been validated and requires much less resources for data collection.
Recent literature has pointed out that India has an immense potential in exploring the agriculture–nutrition pathways by making agriculture pro-poor and pro-nutrition (Kadiyala et al., 2012; Mukhopadhyay, 2012). Systematic disparities across historically and politically relevant identities and their intersections are normatively unacceptable and deserve immediate policy attention. Exploring how inequalities operate across the axes of caste and class and at their intersections thus has important policy relevance. This study contributes to the understanding of the role of agriculture in empowering women and how it varies across the social spectrum.
Overweight and obesity are rising at alarming rates in India, even among the rural poor. Since the IHDS is a panel dataset, the issue of weight gain of women over time can be addressed using the dataset in the future research. Also, recent work has examined the sustainability of women’s empowerment in terms of durability and diffusion using two rounds of IHDS data (Akter & Chindarkar, 2020). One limitation of the paper is that our empowerment indices are all static measures. Extending the framework of Akter and Chindarkar (2020) to conduct similar validation exercises would be interesting.
References
Akter, S., & Chindarkar, N. (2020). An empirical examination of sustainability of women’s empowerment using panel data from India. The Journal of Development Studies, 56(5), 890–906.
Chakravarti, U. (2018/2003) Gendering Caste Through a Feminist Lens. SAGE-Stree.
Coffey, D. (2015). Prepregnancy body mass and weight gain during pregnancy in India and sub-Saharan Africa. Proceedings of the National Academy of Sciences, 112(11), 3302–3307.
Crenshaw, K. (1989). Demarginalizing the intersection of race and sex: A black feminist critique of antidiscrimination doctrine, feminist theory and antiracist politics. University of Chicago Legal Forum, 1989(1), 139–167.
Davis, K. (2008). Intersectionality as buzzword: A sociology of science perspective on what makes a feminist theory successful. Feminist Theory, 9(1), 67–85.
Ewerling, F., Lynch, J. W., Victora, C. G., van Eerdewijk, A., Tyszler, M., & Barros, A. J. D. (2017). The SWPER index for women’s empowerment in Africa: Development and validation of an index based on survey data. Lancet Global Health, 5, e916–e923. https://doi.org/10.1016/S2214-109X(17)30292-9
Ewerling, F., Raj, A., Victora, C. G., Hellwig, F., Coll, C. V., & Barros, A. J. (2020). SWPER Global: A survey-based women’s empowerment index expanded from Africa to all low- and middle-income countries. Journal of Global Health, 10(2), 020343. https://doi.org/10.7189/jogh.10.020434
Gillespie, S., & Kadiyala, S. (2011, February 10–12). Exploring the agriculture-nutrition disconnect in India. In 2020 Conference Brief 20, Prepared for the IFPRI 2020 International Conference, “Leveraging Agriculture for Improving Nutrition and Health”.
Iyer, A., Sen, G., & George, A. (2007). The dynamics of gender and class in access to health care: Evidence from rural Karnataka. India, International Journal of Health Services, 37, 537–554.
Kabeer, N. (1999). Resources, agency, achievements: Reflections on the measurement of women’s empowerment. Development and Change., 30, 435–464.
Kabeer, N. (2005). Gender equality and women’s empowerment: A critical analysis of the third millennium development goal 1. Gender & Development, 13(1), 13–24.
Kadiyala, S., Joshi, P. K., Dev, S. M., Nanda Kumar, T., & Vyas, V. (2012). A nutrition secure India: Role of agriculture. Economic & Political Weekly, XLVII(8), 21–25.
Mukhopadhyay, S. (2012). Agriculture-nutrition pathways: Recognizing the obstacles. Economic and Political Weekly, XLVII(16), 79–80.
Mukhopadhyay, S. (2015). The intersection of gender, caste and class inequalities in child nutrition in India. Asian Population Studies, 11(1), 17–31.
Mukhopadhyay, S. (2016). On the apparent non-significance of sex in child nutrition in India. Journal of Biosocial Science, 48(2), 267–282.
Mukhopadhyay, S., & Chakraborty, A. (2018). Caste gender intersectionalities and the curious case of child undernutrition in India: A methodological exposition. In S. Banerjee & N. Ghosh (Eds.), Caste and Gender in Contemporary India: Power, Privilège and Politics (pp. 213–237). Routledge.
Narayanan, S., Lentz, E., Fontana, M., De, A., & Kulkarni, B. (2019). Developing the women’s empowerment in nutrition index in two states of India. Food Policy, 89, 101780. https://doi.org/10.1016/j.foodpol.2019.101780
Rao, T., & Pingali, P. (2018). The role of agriculture in women’s nutrition: Empirical evidence from India. PLoS ONE, 13(8), e0201115. https://doi.org/10.1371/journal.pone.0201115
Sen, G., & Iyer, A. (2012). Who gains, who loses and how: Leveraging gender and class intersections to secure health entitlements. Social Science and Medicine, 74(11), 1802–1811.
Sen, G., Iyer, A., & George, A. (2007). Systematic hierarchies and systemic failures: Gender and health inequities in Koppal District. Economic and Political Weekly, 42, 682–690.
Sen, G., Iyer, A., & Mukherjee, C. (2009). A methodology to analyse the intersections of social inequalities in health. Journal of Human Development and Capabilities, 10(3), 397–415.
UNICEF. (2020). Women’s empowerment in Kenya: Developing a measure, Kenya National Bureau of Statistics, United Nation’s Entity for Gender Equality and the Empowerment Women (UN Women) and United Nation’s Children Fund. Retrieved June 19, 2021, from https://www.unicef.org/esa/media/8466/file/UNICEF-Kenya-2020-Womens-Empowerment-in-Kenya-2020.pdf.
Weber, L., & Parra-Medina, D. (2003). Intersectionality and women’s health: Charting a path to eliminating health disparities. In: M. T. Segal, V. Demos, J. J. Kronenfeld (Eds.), Gender Perspectives on Health and Medicine (pp. 181–229). Elsevier Science Ltd.
Acknowledgements
This work has benefitted greatly from the comments and suggestions received at the two Workshops for the SPANDAN Grants, held on 14th February 2020 and 25 June 2021. I thank Prof. Alakh Sharma, the discussant of the paper, for his insightful suggestions on the paper. Thanks are also due to Prof. Achin Chakraborty for his comments and to Debopriti Bhattacharya for excellent research assistance.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2024 The Author(s)
About this chapter

Cite this chapter
Mukhopadhyay, S. (2024). Revisiting Women’s Empowerment as an Agriculture–Nutrition Pathway Using the Framework of Intersectionality. In: Dev, S.M., Ganesh-Kumar, A., Pandey, V.L. (eds) Achieving Zero Hunger in India. India Studies in Business and Economics. Springer, Singapore. https://doi.org/10.1007/978-981-99-4413-2_10
Download citation
DOI: https://doi.org/10.1007/978-981-99-4413-2_10
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-99-4412-5
Online ISBN: 978-981-99-4413-2
eBook Packages: Economics and FinanceEconomics and Finance (R0)