
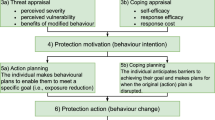
Abstract
Air pollution is often understood through a composition of different kinds of data that increasingly include personal exposure measurements. This chapter is based on our involvement in an interdisciplinary project in Delhi that is combining computational methods and embodied data to simultaneously map, know and respond to air pollution. We use the concept and method of figure, and specifically the figure of ‘the child with asthma’, to explore the tensions that emerge when participants are both objects (sensing bodies that measure air pollution) and subjects (knowing bodies that experience and respond to environmental exposures) of research. This dynamic relationship allows for different ways of figuring out exposure in public health, and thereby possibilities for approaching personalisation that go beyond individualised notions of risk and harm.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others

Keywords
Introduction
The epidemic of asthma and other non-communicable diseases triggered by air pollution has finally placed the environment firmly under the purview of global public health (WHO 2018). Clare Herrick (2020) argues this is an opportunity to shift the optics of health away from behavioural patterns of consumption and towards the complex causalities of toxic exposure. Yet, seductive ideas of technical fixes, awareness-raising and reified models of behaviour change continue to persist in policy and public debates. This is a conceptual and methodological challenge that requires finding new ways of rendering sensible the variegated, interconnected and inequitable geographies of environmental exposures and harm (Fortun 2012; Sultana 2021). Rather than producing more data, calls for ‘smarter’ sensing focus pollution monitoring in places of concern, hotspots and in relation to everyday practices like walking or cooking (Reis et al. 2015), often through participatory and experimental approaches (Lezaun et al. 2017). In this chapter, we discuss an interdisciplinary project that is taking up this task by combining computational methods and embodied data to simultaneously map, know and respond to air pollution. In the project, air pollution is figured through a composition of data practices that include the generation of exposure data by people with asthma. We use the concept and method of figure to explore the tensions that emerge when individuals are both objects and subjects of research. By involving the experience of people affected by air pollution, the project engages with a key concern in public health research and practice of how to best identify exposure risks and generate knowledge that can effectively inform action.
The effects of processes of computation and data science on daily life are being critically engaged with by researchers working in and across the domains of health and medicine (e.g., Day et al. 2017; Prainsack 2017; Radhakrishnan 2021; Ruckenstein et al. 2017), government and welfare services (e.g., Eubanks 2018: Khera 2019), cities and urban planning (e.g., Duarte and Priyanka deSouza 2020; Mattern 2017; Tironi and Sánchez Criado 2015), among many others. Sensing technologies in particular have been described as “a new extension of social control” and “a site where alternative modalities of power are being forged” (Nafus 2016: xiii). In their ethnographic work of a national programme for smart homes in Chile, Tironi and Valderrama (2021) detail the various explanatory logics of domestic sensors provided by government officials, technicians and the residents invited to monitor and quantify their energy use as part of a national programme. According to the authors, a central aim of the initiative is to improve the environmental performance of homes by no longer relying on what people say they do, but on what they actually do: participatory and live information is produced through continuous and recursive feedback from sensors installed in people’s homes (2021: 194). In this example of “sensing governmentality” (Tironi and Valderrama 2021), personalisation is not understood “in the sense of users shaping technologies within their own practice but as technologies that recognise their users and shape themselves accordingly” (Suchman 2012: 222). It is this ‘intelligent’ or ‘aware’ feature of sensing that concerns us in this chapter because it invites new interdisciplinary ways of doing environmental health research. To engage with these developments, we draw on social science and humanities studies of digital technologies that aim to extend the human body’s ‘innate’ capacities through informational means (Creager 2018; Viseu 2003; Viseu and Suchman 2010). We are going to focus specifically on the use of wearable technologies in the interdisciplinary field of air quality and exposure science, a research practice and approach that is increasingly common. By encouraging personal exposure monitoring, new and different relations between people and air are made available for computational calculation.
This chapter is based on ethnographic research of a UK-India funded research project using wearable sensing technologies to generate individualised data on air pollution in New Delhi, India (2018–2020).Footnote 1 We were both researchers on this project, Emma Garnett from the UK and Srishti Bhatnagar from India, and involved in some aspects of the fieldwork led by a multi-sited, interdisciplinary team of senior co-investigators in computer science, public health, digital design and sociology (based in a variety of institutional locations across the UK and India).Footnote 2 For Emma Garnett, the collaboration formed a component of a separate postdoctoral project examining air pollution sensing technologies in biomedical and public health research.Footnote 3 The project in Delhi is an interesting interdisciplinary case study because of its inclusion of social science research as a central work package, which is rather novel in air quality and exposure science. As an international research project, it also represents an aspiration in science, and often research led by the Global North, to expand data coverage of air pollution by monitoring ‘hyper-local’ or ‘micro-environments’ in cities in the Global South, and so encapsulates the geopolitical relations and historical legacies of public health, science, and biomedicine.
In the sensing project we discuss here, the project team also sought to include the experiences of people who bear the brunt of the health costs of air pollution and/or who might not be in a position to necessarily “claim clean air” (Negi and Srigyan 2021: 63, emphasis included): children with asthma. We conceptualise ‘the child with asthma’ as a key figure in contemporary air quality science and public health. It is a figure that brings together a concern to improve public health interventions through more granular measurements of air pollution exposure and its effects on the body by focussing on the people and communities who bear the greatest health burden. As a method, we use the figure of ‘the child with asthma’ to explore the tensions that emerge when involving people understood to be impacted by air pollution as both objects (sensing bodies that measure air pollution) and subjects (knowing bodies that experience and respond to environmental exposures) of research.
‘Person-Centred Environments’
The concept of ‘person-centred environments’ (PCEs) was coined and presented by computer scientists as a novel methodology that incorporates clinical knowledge, big data practices and analytics to track and quantify the embodied effects of air pollution. It can be understood as a practice of personalisation, in which the individual person is the object of study: the person wearing the sensor produces a radius of data points that quantifies exposure ‘inside the body’ through the linking of air pollution measurements, environmental variables, breathing rate and other vital responses. They are also subjects of research because self-produced geo-time stamped data and the self-reporting of daily trajectories are also considered important for understanding exposure. People participating in this study help provide information about social, environmental and genetic contexts from which multiple data points can be generated about air pollution’s health effects (e.g., a measure of air pollution and a quantified bodily response). Our ethnographic research studied this methodological approach in action and analysed how it influences the way in which the problem of air pollution is known and understood.
Recent evidence shows there is no safe level of exposure to many pollutants (Kelly and Fussel 2015). This challenge has ethical implications because if the spatial demarcations between healthy and unhealthy air are unclear, then efforts to improve health in an equitable manner are constrained. The practice of personalisation in scientific research is a response to this challenge because it enables new lines of difference to be stratified along social and biological lines. In our case of PCEs, new groupings of people in relation to air pollution are based on molecular profiles of disease and knowledge of the biological relationship between air pollution and asthma. If the ‘sensitivity’ of children with asthma to air pollution is known, then how they respond to different environmental settings and circumstances is turned into something to be further studied and quantified. In terms of public health efforts to improve health, personalisation articulates and locates exposure and risk in ways that have consequences on how the actions and responsibility to improve it are framed. Asthma and the anticipated differences in the air that it reveals in human bodies is one way in which new normativities and mechanisms of public health are being sought. As Lury and Day (2019) argue, personalisation is always a process of generalisation because entities (such as cancer, but also, as in this case, air pollution’s effects) are specified through the sorting and arranging (drawing lines of inclusion and exclusion) of classes of persons (e.g., people with asthma and children).
The body of research on asthma is huge. It remains a major research topic because it is among the most prevalent non-communicable diseases in childhood, and early life exposures to air pollution play a role in determining the disease in later life (The Global Asthma Report 2018). In our research, we found that focusing on the living environments of people with asthma was used as a way of starting to explain uncertainties in knowledge and the complex and non-linear causalities of air pollution and health (Fortun et al. 2014; Kenner 2018). The conceptual starting point of PCEs is that bodies are permeable, particularly those with asthma, and that living in polluted environments, like areas of urban Delhi, produces measurable perturbations on individuals’ internal physiologies. The hypothesis that follows is that these perturbations are also likely to be modified by other contextual factors, such as the built environment or variables related to socio-economic status. This way of accounting for the environment envisions a neat and all-encompassing way of translating incommensurable phenomena into actionable knowledge. Identifying these kinds of explanatory logics provides a lens from which the politics of environmental health shaping the interdisciplinary intersections of a ‘global’ air quality science and computational public health can be investigated (Landecker 2011).
Linking bodies to environments in this way turns ‘vulnerable bodies’ into objects of knowledge through which significant influences of ‘bad’ environments can be measured in relation to a normative ‘good’ (Choksey 2021). In the case of this project, analytical algorithms are being developed to extract relations of interest from the material contexts of exposure (Amoore and Piotukh 2015). However, by trying to establish more precise measurements of air pollution, computational methods also establish which individual, environmental, biological and social pathways are relevant (Lury and Day 2019: 19). The process of figuring out exposure in this way relies on setting aside some aspects of a person’s surroundings. As we will go on to show, the figure of the child with asthma was put to work in order to distinguish the environmental relations that matter for public health universally. In doing so, we show how personalisation and the ‘optimisation’ it promises can serve to limit the possibilities of situated actions and solutions. Advice to reduce pollution and exposure remains central to public health efforts, and more accurate data is often imagined as a tool to aid everyday decision-making. Yet the options available for people to avoid exposure or clean their breathing spaces are not equally shared in and across societies. We found that this conundrum is also embodied in the figure of ‘the child with asthma,’ which we use as a method and concept for unpacking how PCEs configure sociality and health.
Having introduced PCEs, in what follows we provide a brief overview of the wearable sensors involved in the study and how they work. We then describe the project’s interdisciplinary methods and the ways in which they provided a research context for our own ethnographic study of embodied data practices of personalisation. Following this, we detail two occasions in the early stages of the data collection in Delhi in 2019. Through the figure of ‘the child with asthma,’ we explore the tensions between participants as objects and subjects of research and how this relates to the methods of interdisciplinary research.
‘Experimental Entanglements’: The Wearable Sensors Study
The concept of PCE is integral to the interdisciplinary design of the project in Delhi, which was led by computer scientists in the UK. The wearable sensors used were developed in the UK and deployed in India to explore their potential as an alternative method of monitoring air pollution for public health. The intended participants were children medically recognised to be living with asthma. The protocol for using wearable sensors was adapted from another project led by one of the teams in the UK and which, until COVID-19, continued to be used and modified for related air pollution studies globally. This kind of flexibility in the conduct of monitoring projects is characteristic of global air pollution experiments, in which sensing and monitoring infrastructures are imagined as replicable in different places. It is an approach that reinforces a model of research shaped by a colonial legacy of technoscientific solutions being led by institutions in the Global North and applied to Global South settings. This is particularly significant to note given there are numerous air quality projects in Delhi that are led by Indian scholars and institutions (including projects involving our colleagues based in India and the UK) and are also exploring alternative systems of sensing, monitoring and managing the air (Gani et al. 2022). Indeed, sensors have helped facilitate new and innovative formats for doing science, open data formats and participation in cities globally, and are therefore objects that highlight (and challenge) the power relations and systems of privilege that structure the flow of knowledge, people and resources in a global air quality science (Negi and Srigyan 2021). Indeed, Emma Garnett was the only core team member who had not conducted research in India before but took on a significant project role.
Our main focus in this paper is on the practical work of generating data, because it allows us to better understand the end goal of research and how this might differ in an interdisciplinary research team. The wearable sensor technologies designed by computer scientists record personal exposure to outdoor and indoor air pollution. It was a clinical study design. Each participant in the study was provided with a set of air quality monitors that measure PM2.5, a heterogeneous pollutant made up of microscopic solid or liquid airborne matter. It is also a pollutant that is commonly used in air quality and exposure science as a proxy measure for human health risk. The wearable sensors consist of a GPS-enabled wearable sensor designed to record physiological changes (for instance, the participant’s breathing rate) and track movements. As well as mapping data at a more granular scale than is common in studies of air pollution, like other lower-cost sensing studies, the aim was to also pick up local sources of pollution and aspects of urban environments that mediate exposure (e.g., Hagan et al. 2019). The devices were packed in small sling-bags to carry the power adapter and phone that provide access to an app interface sharing the sensor readings. The breathing sensors were worn directly on the body. A clinical protocol using the molecular profiles of asthma was adapted to monitor the influence of exposures on children with asthma who are known to be susceptible to air pollution’s toxic effects (see, e.g., Vardoulakis and Osborne 2018). Participants were instructed to wear these sensors for a 48-hour period and to continue with their normal daily routines.
In addition to the sensor data and qualitative interviews, the project’s data collection strategy included a survey covering demographic details of each individual (age, educational status, class, caste, religion), the composition of family and household, medical history and asthma management. Other sets of questions sought to capture relevant features of the locality of the participant, such as fuel use and housing quality (e.g., ventilation). A participatory workshop led by digital designers formed the final project work package and was explicitly tasked with translating the qualitative and quantitative data of exposure into impactful knowledge and outcomes. The aim of the workshop was to develop personal stories about air pollution with the same participants who wore the sensors and to then develop these into a series of public-facing animated memes. Although air pollution is routinely figured through numbers, other ways of linking these figures and quantified accounts of air pollution through artistic and creative methods are increasingly recognised as important by researchers and policy makers. The interdisciplinary design of this project was therefore arranged in such a way that alternative, personal narratives of air pollution might be told.
We will now examine and unpick two moments of friction in the interdisciplinary team that relate to the air pollution sensing data practices. These tensions emerged in part because of the reflexive social science involvement in the study. However, they were also practical problems that are generative to think with because they articulate the specific occlusions of personalising air pollution—particularly in relation to understanding systems of marginalisation. The research in this chapter is based on ethnography of the research process, including our involvement in fortnightly team meetings, the conduct of interviews (by Srishti Bhatnagar) and facilitation of a workshop. By tracing how the interdisciplinary methods unfolded and played out in practice, we show that the combination of methods in the project generated very different kinds of data about air pollution that led to epistemological and ontological frictions which support reflexivity (Garnett 2017). Through a discussion of the experimental entanglements (Fitzgerald and Callard 2015) animated in PCEs, we delineate some of the fraught intentions and ambitions the figure of ‘the child with asthma’ produced (cf. Murphy 2017: 82).
Configuring Environmental Health ‘Pathways’
The design and implementation of wearable sensors that materialise a PCE and personalised model of exposure require two key features: (i) the participation of patients with asthma willing to measure their exposure as part of the research study and (ii) developing interpretive frameworks from which to determine significant environmental influences and thereby predictors of health. At the time of writing this chapter, the computer scientists on the project are sorting through the large amounts of data generated by the study to identify significant patterns and relationships. Here, however, we focus on the practical work involved in configuring a computational research environment from which data practices of personalisation in air pollution research could be conducted. We highlight how personalisation in PCEs relies on the embodied practices of sensing, in which wearing the sensors continually enfolds possible environmental (contextual) influences through real-time measurements. It was anticipated by the various researchers who contributed to the design of the research of PCEs (this research design is part of a longer-term vision and approach) that the monitored body contains measurable responses to air pollution. This starting point is based on evidence of the genetic and environmental factors that modulate susceptibility and response to air pollution. We draw on Lury and Day’s (2019) notion of “pathways” to account for how the increased sensitivity of people with asthma presumed an individualised response is measurable. By measuring exposure inside and outside the body, these already well-evidenced exposure pathways served as a background from which individualised health effects of air pollution could be studied in relation to public health. Put another way, the specific gene-environment pathways were not the object of study, rather they facilitated claims to personalisation because the individualised data could simultaneously refer to a generic classification, in this case of vulnerable groups or ‘at risk’ groups.
Negotiating Participation in Research
A core feature of the project was the recruitment of children with asthma to participate in monitoring their exposure. We were variously involved in project discussions of the recruitment process, working closely with colleagues in public health, liaising with doctors and health professionals providing care for asthma out-patients and speaking to parents and children about their involvement in the research. Early on in the recruitment process, several senior investigators in the team expressed concern that the individuals and communities most likely to suffer high levels of air pollution and associated health burdens could be missed because of the study’s protocol. It was argued that there are many young people who have asthma or asthma symptoms but are living without an asthma diagnosis. The implication was that by only recruiting via government and private hospital out-patient lists the project would likely fail to record a range of social and health experiences of air pollution. Following this discussion, one of the co-investigators contacted an environmental NGO working closely with people living in areas of Delhi that experience high levels of air pollution because of well-known emission sites nearby. The aim of making initial contact was to explore the possibility of the project potentially extending the recruitment process beyond formal medical centres in order to cover a range of urban areas. The NGO agreed to help and a couple of weeks later the research team working in Delhi (including the authors) was introduced to around 60 children attending an after-school club. During this meeting, the sociologists and public health researchers encouraged introductions, provided an overview of the project and initiated a lively conversation about air pollution and its health impacts.
Unsurprisingly to some of the team, no one claimed to be experiencing breathing difficulties and only a few reported occasional symptoms of asthma-like conditions. But this finding troubled others in the team. The field note extract below recounts discussions in the weekly project meeting following the visit, in which some of the difficulties involved in ‘finding people with asthma’ outside of biomedical health settings were identified:
The team discusses the previous week’s field visit to an after-school club in North Delhi run by [the NGO] and acknowledges how supportive they have been to the project. Those in the meeting who joined the visit assured the rest of the team that the children who attended the discussion were from a ‘low-income group’ with limited access to medical care [a criterion previously agreed for the three different socio-economic classifications prescribed by the project protocol]. The ‘happy news’ is that very few children attending the after-school club reported experiencing breathing difficulties. Despite living in an area often considered as suffering high air pollution (near waste sites with open burning, close to construction sites and vehicle pollution) the surrounding environmental conditions did not correlate with the children’s accounts of their own health. (Fieldnotes 19 February 2019)
The meeting discussion threw up two rudimentary findings that were hard to reconcile with the project’s protocol. First, air pollution and asthma are experienced as different phenomena with different social meanings and cultural associations. Second, the causes and experiences of health were not the same as biomedical interpretations of risk and harm in global health (Das 2015). The figure of ‘the child with asthma’ brought into focus an interdisciplinary tension concerning the best way to bring the problem of air pollution in relation to the problem of asthma so as not to occlude social marginalisation.
For the computer scientists, ‘the child with asthma’ was primarily a context from which air pollution could be studied anew. Participation was exclusionary, involving only people with asthma because diagnosis is a requirement for identifying ‘a personal pathway’: the strong evidence base of air pollution’s impacts on asthma meant ‘relations’ were understood to be largely imperceptible but ‘out there’ and therefore ready to be measured. For them, the relations opened up the possibility for air pollution to be understood in ‘novel’ ways. The identification of children with asthma was thus a necessary part of the project. In a conversation with one of the computer scientists, we were told that the breathing sensors do not have the sensitivity to pick up physiological responses to air pollution in a person without asthma. A person could only be figured as an object of research in PCEs through their capacity to reveal influences and contain potential correlations. In order to make air pollution perceptible in the big data sets of computational air quality science the person has to be ‘cut out’ (cf Amoore and Piotukh 2015) or provisionally produced. That is, personalising air pollution relies on the overdetermination of asthma which is then able to assume a causal relationship rather than a ‘merely’ contextual one (Sunder Rajan 2012: 6). This determination helps the computer scientists manage the sheer amount and complexity of environmental exposures, yet it also sets the stage within which only some forms of health and sociality can take shape.
As was recognised by the project team, identifying the environmental factors that trigger asthma or exacerbate symptoms by relying exclusively on biomedical categorisation resulted in overlooking some of the so-called upstream determinants of health. By upstream determinants we are pointing to what Nancy Krieger calls “the causes of causes,” in which the conjoining of “power over” and “power to do” structures people’s exposure to material and environmental health hazards (2008: 223). Setting criteria and exclusions is part of knowledge-making, but it is nonetheless significant that in this situation the criteria of asthma created a contradiction because it excluded the possibility of including the experiences of those often excluded from discussions about what to do about air pollution (children, marginalised social groups). Friction in the interdisciplinary team meant that the status of asthma as a biomedical category (a ground or context) for figuring out air pollution’s effects was contested, and the uneven geographies and unequal impacts of exposure difficult to approach as a problem of social justice and public health in the research.
(Personal) Data Frictions
In a second example of friction, in a rather tense team meeting during the first data campaign in summer 2019, the descriptions “add[itional]” and, later, “complement[ary]” were used by one of the senior scientific investigators to describe the role of the social research data in the project. In this framing, the narratives generated by the interviews were understood as providing supplementary variables of use only for interpreting or validating the quantitative sensor data. This description of the potential value of the data was refuted by several of the team involved in the qualitative research. It was argued that the narrative histories of asthma, practices of care and “the intimate knowledges of air through their bodies and their bodies through air” (Negi 2020: 20) generated in the interviews should also count as knowledge and evidence about air pollution.
This difference in valuation was in part structured by a temporal out of jointness (Fitzgerald and Callard 2015) between the “in real time” data of PCEs and the non-linear temporalities that characterised the qualitative assessments of living with asthma. In the quantitative data, the person is fixed in space and time, and the person only comes into view through analytical processes where the co-occurrence of particular data elements gives rise to them (Amoore and Piotukh 2015: 354). However, these data cannot necessarily account for other temporalities such as, for example, cycles of stress (although this is a known trigger for asthma) nor contingencies in everyday forms of decision-making. Tensions concerning the meaning of data are the result of disciplinary and epistemic hierarchies. They also resonate with what has been written about the practical challenges of developing explanatory and interpretive frameworks for making sense of environmental data in the fields of postgenomic science and informatics (Richardson and Hallam 2015; Prainsack 2017). By reducing the environment to a series of compartmentalised variables, the ‘sensing body’ (in our case study) supports a puzzle-solving process in which social and material relations of exposure are assembled into something comprehensible. This is aided by gene-environment links to established biological mechanisms of asthma, which seems to be setting the parameters for exploring new ways of thinking, working and explaining air pollution (cf Richardson and Hallam 2015: 234).
Ethnographic insights from other research emphasise the importance of the patient’s work of participation in scientific efforts to fill “data gaps” (Prainsack 2017: 24). In our case, the ways in which sensors were worn and mobilised, or not, also frequently undermined assumptions about the person as a unit of analysis in PCEs. Together these differences concerning data raised questions about who benefits from an expansive and “inclusive” approach to air pollution monitoring? When discussing their experiences of wearing the sensors and participating in the research, participants very often reported not wearing the devices as self-tracking devices. Many children told us they were wary of taking the sensor outside in case it was misplaced or broken. The parents of others explained that they were concerned about what some people might say about their child if they wore the sensors outside the home. These issues either came as a surprise for some of the computer scientists in the team or were framed as something that needed to be overcome. These interactions with the sensor are also a way to understand the differentiated experience of air pollution and disease, as we will continue to explore.
Efforts to evoke an ‘in real time’ response were hindered because it was not always possible, for those participants who were interested, to read the aggregated data on the app interface (although final reports were provided for each family by the team). Yet it was precisely this data, generated through sensing in everyday practices, like socialising outdoors or playing with friends in neighbouring areas, that the computer scientists wanted to understand to specify individual exposure pathways and, indeed, the kinds of data we thought might be interesting to explore with our social science colleagues further. In these moments the interviews were practically if not epistemologically valuable to the computer scientists because they aided the preliminary screening and interpretation of sensor data. For instance, the interviews and fieldwork helped to provide an explanation for static rather than mobile data collection, why there were long disruptions in data collection (as when families faced connection issues) or why there were sometimes two data sets for one individual (when a participant wanted to try the sensor out again). Although these errors could be managed through statistical technique, they also provide a juncture for attending to the interpretive processes of data practices of personalisation.
Indeed, the challenges of generating personal data are illustrative of the ways in which persons in PCEs always also stand in relation to other personal and nonpersonal environments of exposure (Lamoreaux 2016). These tensions encourage a shift in analytical focus, away from what makes environments ‘bad’ to how they are made ‘good’ by participants themselves. The interview transcripts collated a number of creative ways young people dealt with events that aggravated their asthma: not running around by playing batsman rather than a field position in games of cricket; working extra hard to overcome missing days from school; by trying and testing medicines to see what works in different situations; and tracking causes of symptoms and what improves them. As demonstrated in the reference to the team meeting discussing the role of qualitative data, the PCEs gestured towards other possible experimental entanglements where the object of research and its aims could be questioned by its subjects.
To further explore this point of unsettling the relations of subjects and objects we also want to consider a children’s workshop that was hosted by one of the collaborating institutions in North Delhi on a Saturday in early May 2019. It was originally intended as a knowledge translation activity, however, due to various logistical challenges, the workshop ended up taking place as the first data campaign was just getting started and therefore intervened in the conduct of the research rather than simply facilitating dissemination. It brought together the research team, parents and children, including the children who we met at the after-school club. The clinical protocol was put to one side and therefore who could participate was not predetermined beyond their being a child or young person.
The workshop sought to visualise personal, embodied narratives by exploring experiences of air pollution collectively, as this description of the process explains:
I mean that’s how it was also planned [to use different artistic mediums to develop the narratives] but giving it flexibility, that is also how it worked, that you start first with just playing with the idea of pollution. How can we experience it? What are the words to be able to experience it? Then what are the colours to be able to experience it? And then we moved to this idea of, like, a character who is experiencing pollution; then that character’s setting, which is kind of taken from their experience of their environment, and then it comes to be personal, drawing from personal experience. (Group Interview, 11 May 2019)
The mixed media approach proposed provides a different form of participation in which the purpose is to encourage descriptions and depictions of it and to go beyond, as one facilitator put it, ‘generic accounts’ of the problem. By characterising a person with asthma which is relatable to the participants, and potentially wider publics, the ‘person with asthma’ becomes a subjective storytelling device in which the objects of air pollution, asthma, and inequality are held together without one displacing the other. This not only affected the objects of research but the power dynamics assumed in the clinical research because participants were not there to understand their own risks but rather to consider what actions people and communities can take to ensure more breathable air for children with asthma. In one instance, some of the children shared a specific verb to describe a feeling that breathing in pollution can create, like a trapped cough or having something stuck in your throat. The word was not known to any of the adults in the room, and it shifted the tone and dynamic of the dialogue because the children participating momentarily became the experts in how to describe and account for air pollution’s effects.
Following the workshop the visualisation created by the children was further developed in dialogue with the interview transcripts to create a series of animated memes (to be shared publicly) that linked the problems people face to calls for collective action (with the tagline “let me breathe”). PCEs were temporarily denaturalised, and the question of the future shown to be neither inevitable nor obvious; interventions by children with asthma as subjects of the research, not only as objects, were introduced. In working in the disconnections between the individual accounts of air pollution produced in the interviews and sensor data collection, how the figure of ‘the child with asthma’ would lead to the public health promises that underpinned its emergence was destabilised. This is not a gap in the data but a destabilisation which reveals the dynamics of inclusion and exclusion that characterise personalisation and which predetermine the parameters for knowing air pollution exposure.
Conclusions
Global inequalities in air pollution and uncertainties in health evidence have led to new methods, technologies and collaborations for studying the variegated environmental contexts of exposure in different places. Drawing on our participation in a computer science-public health-social science collaboration measuring embodied air pollution exposure in Delhi, we use the figure of “the child with asthma” as a concept and method for studying the interdisciplinary methods involved in making environments personal. The computational framework of PCEs meant research participants were approached as both research objects and subjects: measuring air pollution inside bodies stabilised the relationship between air pollution and health as an object, whilst the person wearing the sensor mediated air pollution through situated negotiations and engagement with it as a subject. However, this dynamic relationship caused tensions between the project’s team members during the setting up of the research process and when trying to determine the role and value of people’s involvement and the different data sets they produce. First, we showed how clinical representations of asthma result in personalised monitoring that influence which ‘environments’ are included in research. By invoking and requiring an asthma diagnosis, the places and contexts of exposure to pollution that the research also sought to get a handle on were excluded. Second, we showed how the different methods continually reconfigure the subjects and objects of research in ways that destabilise what the problem is (asthma or air pollution, public health or inequality) and how to approach it analytically (instrumentalising qualitative data or engaging with it in a critical manner as at the workshop). By tracing a series of subject-object relations we argue that practices of figuring air pollution as personal in interdisciplinary research create new biomedical categories—vulnerable or ‘at risk’ groups. However, the environmental and social “pathways” embodied sensing also materialise is limited by an associated narrow definition of exposure, despite the possibilities for its empirical expansion.
We therefore use the figure of ‘the child with asthma’ to investigate the possibilities and implications of computational methods (sensors, algorithms) for understanding the dynamic relations between embodiment (e.g., the figure) and context or practice (e.g., ground or background) in air pollution exposure. By figuring out exposure in this way it is anticipated that public health interventions can be specified and improved. We found the interdisciplinary tensions that emerged in the project generative to think with because of the ways personalisation indicates the possibility or necessity of action beyond the generation of scientific knowledge and data (Rajan 2006: 179)—although the sensors were ultimately only a tool of foresight, a way to manage probable futures (the environmental conditions that increase the likelihood of worsening asthma symptoms) rather than target the causes of exposure and delineate actions. Nonetheless, the introduction of personal air pollution monitoring is promising to capture societal and geographic differences in exposure that could make perceptible new causal pathways that are not only biological in nature. In our case, it is hoped by some of the computer scientists involved that even if not calculable individual knowledge and experiences can ultimately enlarge computational analysis. What stymies these efforts are pre-determined ideas of symptoms and disease that are stable across environmental and cultural contexts (even if their physical and experiential manifestation are recognised as situated). The figure of ‘the child with asthma’ has helped us elaborate some of these operations of inclusion/exclusion in data and algorithmic practices, that at once expand and contract ways of accounting for the embodied effects of air pollution and harm.
Supporting a more granular and targeted approach to data generation does not necessarily challenge the socio-political conditions and inequalities that allow environmental hazards to happen in the first place (Senier et al. 2017). As Michelle Murphy argues, granular studies of embodied health (e.g., air pollution personalisation) need to be interlinked with contestations over the physical production and distribution of chemical harm (2013: 698), including how prevalent public health and global health approaches might obfuscate these dynamics. Although the dynamic subject-object refiguring of embodied air pollution sensing in our case study did attempt such interlinking to address these complexities, the challenges involved in making commensurate the various roles and possibilities of personal data means how it actually influences approaches to exposure and risk is difficult to discern. The interdisciplinary methods that PCEs facilitate did help to disrupt the dominant idea that personal data or information about air pollution is necessary for public health knowledge and action, however. The actions carried out by young people and their families to manage their exposure highlight some of the ways in which ‘good’ environments are (as shown in the interviews) or could be (as explored in the workshops) achieved in different situations. By studying wearable sensors in research practices, we demonstrate the value of recognising these more ambivalent “interconnections between bodies and data” (Radhakrishnan 2021) as occasions when air pollution is figured differently. This research hopefully opens up further points of inquiry, in terms of who benefits from personal data and how future figurations of air pollution might incorporate the social and environmental causes of exposure that are not currently available to computation.
Notes
- 1.
Funded by a Global Challenges Research Fund grant.
- 2.
These institutional locations will remain anonymous in this chapter.
- 3.
Funded by an ESRC New Investigator Award: ES/R008612/1. The study sought ethical approval from King’s College London Ethics Ref: LRS-18/19-10426
References
Amoore, Louise, and Volha Piotukh. 2015. ‘Life beyond Big Data: Governing with Little Analytics’. Economy and Society 44 (3): 341–66. https://doi.org/https://doi.org/10.1080/03085147.2015.1043793.
Choksey, Lara. 2021. ‘Environmental Racialisation and Poetics of Influence in the Postgenomic Era: Fire, Soil, Spirit’. Medical Humanities 47 (2): 145–55. https://doi.org/https://doi.org/10.1136/medhum-2020-012061.
Creager, Angela N. H. 2018. ‘Human Bodies as Chemical Sensors: A History of Biomonitoring for Environmental Health and Regulation’. Studies in History and Philosophy of Science Part A, Experiencing the Global Environment, 70 (August): 70–81. https://doi.org/https://doi.org/10.1016/j.shpsa.2018.05.010.
Darling, Katherine Weatherford, Sara L. Ackerman, Robert H. Hiatt, Sandra Soo-Jin Lee, and Janet K. Shim. 2016. ‘Enacting the Molecular Imperative: How Gene-Environment Interaction Research Links Bodies and Environments in the Post-Genomic Age’. Social Science & Medicine (1982) 155 (April): 51–60. https://doi.org/10.1016/j.socscimed.2016.03.007.
Das, Veena. 2015. Affliction: Health, Poverty and Disease. New York, NY, USA: Fordham Press. https://www.fordhampress.com/9780823261819/affliction.
Day, Sophie, R. Charles Coombes, Louise McGrath-Lone, Claudia Schoenborn, and Helen Ward. 2017. ‘Stratified, Precision or Personalised Medicine? Cancer Services in the “Real World” of a London Hospital’. Sociology of Health & Illness 39 (1): 143–58. https://doi.org/https://doi.org/10.1111/1467-9566.12457.
Duarte, Fábio, and Priyanka deSouza. 2020. ‘Data Science and Cities: A Critical Approach’. Harvard Data Science Review, July. https://doi.org/https://doi.org/10.1162/99608f92.b3fc5cc8.
Eubanks, Virginia. 2018. Automating Inequality. How High-Tech Tools Profile, Police, and Punish the Poor. New York: St Martin’s Press.
Fitzgerald, Des, and Felicity Callard. 2015. ‘Social Science and Neuroscience beyond Interdisciplinarity: Experimental Entanglements’. Theory, Culture & Society 32 (1): 3–32. https://doi.org/https://doi.org/10.1177/0263276414537319.
Fortun, Kim. 2012. ‘Ethnography in Late Industrialism’. Cultural Anthropology 27 (3): 446–64. https://doi.org/https://doi.org/10.1111/j.1548-1360.2012.01153.x.
Fortun, Mike, Brendan Costelloe-Kuehn, Tahereh Saheb, Daniel Price, Alison Kenner, and Kim Fortun. 2014. ‘Asthma, Culture, and Cultural Analysis: Continuing Challenges’. In Heterogeneity in Asthma, 321–32. Boston MA: Humana Press.
Gani, Shahzad, Pallavi Pant, Sayantan Sarkar, Neha Sharma, Sagnik Dey, Sarath K Guttikunda, Krishna M AchutaRao, Jostein Nygard and Ambuj D Sargar. 2022. ‘Systematizing the approach to air quality measurement and analysis in low and middle income countries’. Environmental Research Letters. 17 (2): 021004. https://doi.org/10.1088/1748-9326/ac4a9e.
Garnett, Emma. 2017. ‘Air Pollution in the Making: Multiplicity and Difference in Interdisciplinary Data Practices’. Science, Technology, & Human Values 42 (5): 901–24. https://doi.org/https://doi.org/10.1177/0162243917699974.
Hagan, David H., Shahzad Gani, Sahil Bhandari, Kanan Patel, Gazala Habib, Joshua S. Apte, Lea Hildebrandt Ruiz, and Jesse H. Kroll. 2019. ‘Inferring Aerosol Sources from Low-Cost Air Quality Sensor Measurements: A Case Study in Delhi, India’. Environmental Science & Technology Letters 6 (8): 467–72. https://doi.org/https://doi.org/10.1021/acs.estlett.9b00393.
Herrick, Clare. 2020. ‘The Optics of Noncommunicable Diseases: From Lifestyle to Environmental Toxicity’. Sociology of Health & Illness 42 (5): 1041–59. https://doi.org/https://doi.org/10.1111/1467-9566.13078.
Kelly, Frank J., and Fussel, Julia C. 2015. ‘Air pollution and public health: emerging hazards and improved understanding of risk’. Environ Geochem Health 37(4):631-49.
Kenner, Alison. 2018. Breathtaking: Asthma Care in a Time of Climate Change. Minneapolis and London: University of Minnesota Press.
Khera, R. 2019. Dissent on Aadhaar: Big Data Meets Big Brother. Hyderabad: Orient Black Swan.
Krieger, Nancy 2008. ‘Proximal, distal, and the politics of causation: what’s level got to do with it?’. American journal of public health, 98(2): 221–230. https://doi.org/10.2105/AJPH.2007.111278.
Lamoreaux, Janelle. 2016. ‘What If the Environment Is a Person? Lineages of Epigenetic Science in a Toxic China’. Cultural Anthropology 31 (2): 188–214. https://doi.org/10.14506/ca31.2.03.
Landecker, Hannah. 2011. ‘Food as Exposure: Nutritional Epigenetics and the New Metabolism’. BioSocieties 6 (2): 167–94. https://doi.org/https://doi.org/10.1057/biosoc.2011.1.
Lezaun, Javier, Noortje Marres, and Manuel Tironi. 2017. ‘Experiments in Participation’. In The Handbook of Science and Technology Studies Edition: 4th edited, 195–222. MIT Press.
Lury, Celia, and Sophie Day. 2019. ‘Algorithmic Personalization as a Mode of Individuation’. Theory, Culture & Society 36 (2): 17–37. https://doi.org/https://doi.org/10.1177/0263276418818888.
Murphy, Michelle. 2013. ‘Distributed Reproduction, Chemical Violence, and Latency’. The Scholar and Feminist Online 11 (3): 1–7.
Murphy, Michelle. 2017. The Economization of Life. Durham and London: Duke University Press.
Nafus, Dawn. 2016. Quantified: Biosensing Technologies in Everyday Life. Cambridge MA: MIT Press.
Shannon Mattern. 2017. ‘A City Is Not a Computer’. Places Journal, February 2017. Accessed 15 Jul 2021. https://doi.org/10.22269/170207
Negi, Rohit. 2020. ‘Urban Air’. Comparative Studies of South Asia, Africa and the Middle East, 40(1): 17-23. doi https://doi.org/10.1215/1089201X-8185994
Negi, Rohit, and Prerna Srigyan. 2021. Atmosphere of Collaboration: Air Pollution Science, Politics and Ecopreneurship in Delhi. Routledge.
Prainsack, Barabara. 2017. ‘Personalized Medicine: Empowered Patients in the 21st Century’. NYU Press (blog). 2017. https://nyupress.org/9781479814589/personalized-medicine.
Radhakrishnan, Radhika. 2021. ‘Health Data as Wealth: Understanding Patient Rights in India within a Digital Ecosystem through a Feminist Approach’. Working Paper 19, Data Governance Network, Mumbai.
Rajan, Kaushik Sunder. 2006. Biocaptial: The Constitution of Postgenomic Life. Durham and London: Duke University Press.
Reis, Stefan, Edmund Seto, Amanda Northcross, Nigel W. T. Quinn, Matteo Convertino, Rod L. Jones, Holger R. Maier, et al. 2015. ‘Integrating Modelling and Smart Sensors for Environmental and Human Health’. Environmental Modelling & Software 74 (December): 238–46. https://doi.org/10.1016/j.envsoft.2015.06.003.
Richardson, Sarah, and Stevens Hallam. 2015. ‘Postgenomics: Perspectives on Biology after the Genome’. In Beyond the Genome. Durham; London: Duke University Press.
Ruckenstein, Minna, Schüll, Natasha. D. 2017. ‘The Datafication of Health’. Annual Review of Anthropology, 46: 261-278.
Senier, Laura, Phil Brown, Sara Shostak, and Bridget Hanna. 2017. ‘The Socio-Exposome: Advancing Exposure Science and Environmental Justice in a Post-Genomic Era’. Environmental Sociology 3 (2): 107–21. https://doi.org/10.1080/23251042.2016.1220848.
Suchman, Lucy. 2012. ‘Configuration’. In Inventive Methods: The Happening of the Social, Celia Lury and Nina Wakeford, 48–61. London: Routledge. https://doi.org/10.4324/9780203854921-8.
Sultana, Farhana. 2021. ‘Climate Change, COVID-19, and the Co-Production of Injustices: A Feminist Reading of Overlapping Crises’. Social & Cultural Geography, April, 1–14. https://doi.org/10.1080/14649365.2021.1910994.
The Global Asthma Report 2018. 2018. Auckland, New Zealand: Global Asthma Network. http://globalasthmareport.org/.
Tironi, Martin, and Tomás Sánchez Criado. 2015. ‘Of Sensors and Sensitivities. Towards a Cosmopolitics of “Smart Cities”?’.TECNOSCIENZA: Italian Journal of Science & Technology Studies 6 (1) pp. 89-108
Tironi, Martín, and Matías Valderrama. 2021. ‘Experimenting with the Social Life of Homes: Sensor Governmentality and Its Frictions’. Science as Culture 30 (2): 192–215. https://doi.org/10.1080/09505431.2021.1893682.
Vardoulakis, Sotiris, and Nicholas Osborne. 2018. ‘Air Pollution and Asthma’. Archives of Disease in Childhood 103 (9): 813–14. https://doi.org/10.1136/archdischild-2017-314543.
Viseu, Ana. 2003. ‘Simulation and Augmentation: Issues of Wearable Computers’. Ethics and Information Technology 5 (1): 17–26. https://doi.org/10.1023/A:1024928320234.
Viseu, Ana and Suchman, Lucy. 2010. Wearable Augmentations. In Jeanette Edwards, Penny Harvey & Peter Wade (Eds.), Technologized Images, Technologized Bodies: anthropological approaches to a new politics of vision. Oxford, New York: Berghahn Books.
World Health Organisation. 2018. ‘Time to Deliver: Report of the WHO Independent High-Level Commission on Noncommunicable Diseases’. Geneva: WHO.
Acknowledgements
The authors would like to thank the wider project team in the UK and India for their support and the young people and their parents in Delhi who participated in the research. An early presentation of this chapter at the Innovating Air Pollution Governance: Collaborations, Interruptions and Regenerations panel organised by Maka Suarez, Katie Cox and Rohit Negi during the 2019 4S conference in New Orleans helped develop our thinking. Many thanks to Celia Lury, Scott Wark and William Viney for their insightful and formative feedback on previous versions of this chapter.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2022 The Author(s)
About this chapter

Cite this chapter
Garnett, E., Bhatnagar, S. (2022). Figuring Out Exposure: Exploring Computational Environments and Personalisation in Interdisciplinary Air Pollution Research. In: Lury, C., Viney, W., Wark, S. (eds) Figure. Palgrave Macmillan, Singapore. https://doi.org/10.1007/978-981-19-2476-7_10
Download citation
DOI: https://doi.org/10.1007/978-981-19-2476-7_10
Published:
Publisher Name: Palgrave Macmillan, Singapore
Print ISBN: 978-981-19-2475-0
Online ISBN: 978-981-19-2476-7
eBook Packages: Social SciencesSocial Sciences (R0)