
Abstract
There is a multi-directional relationship between communication difficulties and mental health. A young person with a language disorder may fall behind at school, have difficulty maintaining appropriate peer relationships and have trouble expressing their internal experience. This can result in adverse mental health outcomes. Conversely, a mental health condition which leads to a young person not attending school and withdrawing from family and friends alters the environmental input they receive in terms of speech, language and social communication; they may therefore fall behind in these areas. It is also important to recognise that communication impairments are inherent in a number of mental health conditions—for example, marked changes to speech rate and language content in psychoses.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
A senior speech pathologist is a member of the multidisciplinary team (MDT) at the Walker Unit. The speech pathologist assesses the communication needs of the young people and diagnoses any potential communication impairments. They also collaborate with the MDT to modify the ward programme and materials, such as care plans, to ensure they are accessible for varying levels of communication ability. The speech pathologist acts as a consultant to the unit on communication matters, while also providing direct interventions to young people either individually or in groups.
The Walker Unit recognises the importance of determining any underlying communication difficulties and tailoring its service to the communication needs of an individual young person. This chapter will explore the work of speech pathologists on the unit. It should be noted that speech pathologists also assess and manage dysphagia (swallowing difficulties). Management of dysphagia is not a common requirement at the Walker Unit however and thus this chapter will focus on communication.
Signs of Communication Difficulty
Effective communication is the expression of wants, needs and feelings by the “sender” or “speaker” and the accurate interpretation or comprehension of these by a “receiver” or “listener”. Communication is not simply talking; other communication skills include hearing, listening, understanding, social skills, reading and writing (Speech Pathology Australia, 2010). Non-verbal communication is just as valid a means of communication as speaking and at times is easier for people to engage with.
When working with a young person the following may be signs of communication difficulty:
-
misinterpreting questions or instructions (i.e. giving “strange” or unrelated answers, doing a task differently than how they were told or not at all)
-
limited vocabulary when explaining their thoughts, opinions and feelings,
-
difficulty with school work or reluctance to attend school
-
requiring additional time to complete tasks
-
appearing to be behind in conversation, that is, seeming not to recognise when the topic has moved on
-
difficulty interpreting sarcasm, understanding jokes and reading the body language of others
-
not initiating any interactions and/or when asked questions giving one or two word responses
Why it Is Important to Recognise Communication Difficulties
Communication difficulties during childhood and adolescence can significantly impact on an individual’s psychosocial outcomes, educational attainment and wider social experience. Research has shown the links between communication abilities and education outcomes (Conti-Ramsden et al., 2009), self-esteem (Jerome et al., 2002), peer relationships (Durkin & Conti-Ramsden, 2007) and externalising behaviours (James et al., 2020; Maggio et al., 2014).
Those with a communication disorder in early life are at greater risk of particular mental health conditions (Arkkila et al., 2008; Charman et al., 2015). Furthermore, communication difficulties have implications for a young person’s ability to engage in mental health treatment (Conti-Ramsden et al., 2013).
Speech Pathology at the Walker Unit
At the Walker unit, the speech pathologist is part of the “in-house” team rather than an ad hoc referral service. This is an important point of difference compared to many other mental health services. When a speech pathologist is included in the team, they have greater opportunity to identify and support the communication needs of the young people. As such, the speech pathologist participates in all patient care meetings, ranging from daily handover to bi-monthly mini-team meetings. Due to the at times volatile or changeable nature of complex mental health admissions communication supports may be needed with little notice and having the speech pathologist onsite allows for a prompt intervention.
When a young person is admitted to the Walker Unit the speech pathologist screens their history to identify any information which could signify the need for communication supports, including but not limited to a consideration of mental health diagnosis, a prior diagnosis of a communication disorder, hearing ability, literacy, academic performance, and conditions that frequently present with communication differences or difficulties such as autism spectrum disorder (ASD), attention deficit hyperactivity disorder (ADHD), and intellectual disability.
Formal communication assessment may be required as part of the diagnostic work up. Formal and informal communication assessment will also occur if the speech pathologist identifies behaviours which could indicate previously undiagnosed difficulties. Assessment and intervention may need to be adapted for young people of culturally and linguistically diverse backgrounds. Examples of adaption include the use of interpreters, the exclusion of particular assessments which rely on background cultural knowledge or idioms, and/or the use of subtests from some standardised assessments used instead informally as sources of qualitative information rather than to get standard scores.
Formal assessment, where a young person can be compared to aged matched peers, may include the Clinical Evaluation of Language Fundamentals (Wiig & Secord, 2014; Wiig et al., 2013), the Test for Reception of Grammar (Bishop, 2003), the Peabody Picture Vocabulary test (Dunn, 2019), the Expressive Vocabulary test (Williams, 2019), and/or The Awareness of Social Inference Test—Revised (McDonald et al., 2011), and Social Language Development Test (Bowers et al., 2017), depending on the clinical question. None of the instruments listed were designed specifically for use with young people in a mental health setting. As such, speech pathologists must use their best clinical judgement to determine the most appropriate instrument for each young person.
Informal assessment refers to non-standardised non-normed observations and information collection. This can occur in a variety of ways and may gather information from a range of communication partners including family, teachers, nursing and other clinical staff. Methods can include semi structured interviews, pragmatic profiles (see e.g. Dewart & Summers, 1996), communication checklists, and observations made by the speech pathologist of the young person in different group settings, during different activities on the ward and with different people. Young people are always asked about their own view of their communication, including strengths and challenges. This includes who the young person finds it easy or easiest to communicate with and in what contexts. Self-report may be facilitated by the use of checklists such as those in the Talkabout manuals (Kelly & Bains, 2017; Kelly et al., 2019). Additionally, insight and motivation are important to ascertain at assessment to determine approach to intervention (i.e. direct or environmental). A long period of rapport building is often necessary to gain the trust of the young person, so that they will engage in these interactions.
At the Walker Unit, in addition to a comprehensive assessment report, a simple language version is created and shared with the carer and/or young person. This supports comprehension of the assessment results bearing in mind that families may also have communication difficulties (Kang & Drayna, 2011). Additionally, reports for disability support funding agencies (in Australia, the National Disability Insurance Scheme) may provide further support for access to the scheme and/or result in funding for the young person to continue receiving particular supports post discharge which may include seeing a speech pathologist.
The target for any direct intervention is determined in collaboration with the young person, working with their motivation. For example, a young person with a severe language disorder and social communication difficulties identified the most important thing for them was not being the “stupid” one in their grade. When this was explored further they were able to identify that they felt “stupid” when they did not understand what other people were laughing or joking about. The focus was therefore on vocabulary, in particular multi-meaning words and inferencing. This contributed to them feeling more comfortable around their peers and supported their wider receptive language skills.
The speech pathologist works collaboratively with the art and music therapists to support non-verbal expression and when appropriate, supports the young person to put words to their experience. At times, the speech pathologist may work with the young person to create or document their emotional “vocabulary”. This does not necessarily mean changing the words the young person uses for their experience. More often it will take the form of documenting what these words actually mean or signal for the young person so that those caring for them can understand what they are trying to communicate. For example, one young person may use the word “ok” to describe a sense of calm whilst for someone else this may mean “I’m feeling on the verge of self-harm”.
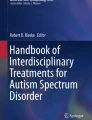
The speech pathologist often uses visual aids to support communication. Comic Strip Conversations (Gray, 1994) is an example of a visual approach that the speech pathologist may use with young people at the Walker Unit. The approach uses drawings and colours to visually represent different perspectives in social situations. Individuals can benefit from this as it makes the more abstract aspects of social communication easier to understand. The approach can be used to explore social difficulties that occur, considering what is said as well as thoughts and feelings (which are visually represented). It can also be used to consider different outcomes that could result from different ways of interacting (see Figs. 14.1a and 14.1b). Another visual aid is Talking Mats ™ (Murphy & Cameron, 2006), an interactive resource that can be used to support comprehension, and to facilitate expression of feelings and opinions. It uses sets of cards which show a picture and word relating to various topics. This resource can reduce the cognitive load required for communication and facilitate expression for those who find it difficult to verbalise, whether this be due to anxiety or a communication disorder. Furthermore, it does not require literacy skills which is beneficial, given well established links between literacy difficulties and emotional and behavioural conditions (Hurry et al., 2018).

Comic Strip Conversation, using the methodology of Carol Gray (1994) exploring an interaction with a young person and their Father. What was said is shown in speech bubbles, what was thought by the young person and potentially thought by the father is shown in thought bubbles and the way these things were said/potential feelings is shown by the colours. In this case green represents a friendly or relaxed feeling and blue represents an uncomfortable or stressed feeling

Following on from the event in Fig. 14.1a this image depicts what could have happened if the young person had said something different in the same situation
A diagnosis of a communication disorder or determination of particular communication needs can be new information for carers. Education on these topics can raise awareness and change behaviour in terms of interactions amongst family members. When needed, the speech pathologist works with carers to consider different communication profiles, provide communication partner education and/or training to facilitate more effective or enjoyable interactions.
A number of communication groups have been run by speech pathologists at the Walker Unit, which have targeted basic communication skills such as having an awareness of self and others, through to groups which focus on more complex pragmatic skills such as how to start and keep conversations going. Talkabout resources (Kelly & Bains, 2017; Kelly et al., 2019) are an example of resources used to support group content. In other circumstances, the speech pathologist contributes by advising how a ward group may need to adapt to the specific communication needs of young people.
Conclusion
A large number of young people with mental health conditions have communication difficulties. Staff at the Walker Unit have the skills and indeed a responsibility to use communication that is accessible to an adolescent cohort. The specific skills of the speech pathologist are required when a young person has additional communication needs.
References
Arkkila, E., Rasanen, P., Roine, R. P., & Vilkman, E. (2008). Specific language impairment in childhood is associated with impaired mental and social well-being in adulthood. Logopedics, Phoniatrics, Vocology, 33(4), 179–189. https://doi.org/10.1080/14015430802088289
Bishop, D. V. M. (2003). Test of reception of grammar version 2 (TROG-2.). Pearson Assessment.
Bowers, L., Huisingh, R., & Lo Giudice, C. (2017). Social language development test—Adolescent: normative update. Pro-ed.
Charman, T., Ricketts, J., Dockrell, J. E., Lindsay, G., & Palikara, O. (2015). Emotional and behavioural problems in children with language impairments and children with autism spectrum disorders. International Journal of Language & Communication Disorders, 50(1), 84–93. https://doi.org/10.1111/1460-6984.12116
Conti-Ramsden, G., Durkin, K., Simkin, Z., & Knox, E. (2009). Specific language impairment and school outcomes. I: Identifying and explaining variability at the end of compulsory education. International Journal of Language & Communication Disorders, 44(1), 15–35. https://doi.org/10.1080/13682820801921601
Conti-Ramsden, G., Mok, P. L., Pickles, A., & Durkin, K. (2013). Adolescents with a history of specific language impairment (SLI): Strengths and difficulties in social, emotional and behavioral functioning. Research in Developmental Disabilities, 34(11), 4161–4169. https://doi.org/10.1016/j.ridd.2013.08.043
Dewart, H., & Summers, S. T. (1996). The pragmatics profile of everyday communication skills in adults. NFER-NELSON.
Dunn, D. M. (2019). Peabody picture vocabulary test (5th ed.). NCS Pearson.
Durkin, K., & Conti-Ramsden, G. (2007). Language, social behavior, and the quality of friendships in adolescents with and without a history of specific language impairment. Child Development, 78(5), 1441–1457. https://doi.org/10.1111/j.1467-8624.2007.01076.x
Gray, C. (1994). Comic strip conversations: Illustrated interactions that teach conversation skills to students with autism and related disorders. Future Horizons.
Hurry, J., Flouri, E., & Sylva, K. (2018). Literacy difficulties and emotional and behavior disorders: Causes and consequences. Journal of Education for Students Placed at Risk, 23(3), 259–279. https://doi.org/10.1080/10824669.2018.1482748
James, K., Munro, N., Togher, L., & Cordier, R. (2020). The spoken language and social communication characteristics of adolescents in Behavioral schools: A controlled comparison study. Language, Speech, and Hearing Services in Schools, 51(1), 115–127. https://doi.org/10.1044/2019_lshss-18-0090
Jerome, A. C., Fujiki, M., Brinton, B., & James, S. L. (2002). Self-esteem in children with specific language impairment. Journal of Speech, Language, and Hearing Research, 45(4), 700–714. https://doi.org/10.1044/1092-4388(2002/056)
Kang, C., & Drayna, D. (2011). Genetics of speech and language disorders. Annual Review of Genomics and Human Genetics, 12, 145–164. https://doi.org/10.1146/annurev-genom-090810-183119
Kelly, A., & Bains, S. (2017). Talkabout for teenagers: Developing social and emotional communication skills (2nd ed.). Taylor & Francis Ltd..
Kelly, A., Tarshis, N., & Meringolo, D. (2019). Talkabout: A social communication skills package. Routledge.
Maggio, V., Grañana, N. E., Richaudeau, A., Torres, S., Giannotti, A., & Suburo, A. M. (2014). Behavior problems in children with specific language impairment. Journal of Child Neurology, 29(2), 194–202. https://doi.org/10.1177/0883073813509886
McDonald, S., Flanagan, S., & Rollins, J. (2011). The awareness of social inference test (revised). Pearson Assessment.
Murphy, J., & Cameron, L. (2006). Talking Mats: A resource to enhance communication. University of Stirling.
Speech Pathology Australia. (2010). Speech pathology in mental health services clinical guideline. Retrieved 28 Sept, 2021, from www.speechpathologyaustralia.org.au/SPAweb/Members/Clinical_Guidelines/spaweb/Members/Clinical_Guidelines/Clinical_Guidelines.aspx?hkey=f66634e4-825a-4f1a-910d-644553f59140
Wiig, E. H., & Secord, W. A. (2014). Clinical evaluation of language fundamentals, fifth edition metalinguistics (CELF®-5 metalinguistics). NCS Pearson.
Wiig, E. H., Semel, E., & Secord, W. A. (2013). Clinical evaluation of language fundamentals –fifth edition. NCS Pearson.
Williams, K. T. (2019). Expressive vocabulary test (3rd ed.). NCS Pearson.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2022 The Author(s)
About this chapter

Cite this chapter
Jones, K. (2022). Speech and Language Therapy. In: Hazell, P. (eds) Longer-Term Psychiatric Inpatient Care for Adolescents. Palgrave Macmillan, Singapore. https://doi.org/10.1007/978-981-19-1950-3_14
Download citation
DOI: https://doi.org/10.1007/978-981-19-1950-3_14
Published:
Publisher Name: Palgrave Macmillan, Singapore
Print ISBN: 978-981-19-1949-7
Online ISBN: 978-981-19-1950-3
eBook Packages: Social SciencesSocial Sciences (R0)