
Abstract
The use of technology to respond to the COVID-19 emergency is described. The sudden lockdown imposed by the government with just a four hours’ notice resulted in a paralysis of the healthcare system. World Health Partners (WHP) responded immediately to this crisis. WHP worked in partnership with the state governments of Bihar and Andhra Pradesh. The plan was that the state governments would provide the personnel and WHP would set-up a digitized system for providing health services to the people by using tele-medicine.
A quick-to-access dashboard was created to give details in real-time of the number of doctors and assistants who were logged-in, the number of calls received and were attended to, prescriptions issued, and COVID-19 suspects identified. Doctors’ absenteeism proved to be a challenge in Bihar. Consequently, the full potential of the project could not be realized in Bihar. In Andhra Pradesh, however, the project was very successful. Despite receiving less number of calls, more consultations were provided through the tele-medicine project in Andhra Pradesh. The major reason for this success was the high level of political commitment by the state government which led to the availability of trained medical personnel for the project. The entire process of the project was successfully transitioned by WHP to the state government of Andhra Pradesh.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Waking Up to a Crisis
By early March 2020, it was evident that a major health crisis was at India’s doorsteps. The only administrative perspective available for combating the rapid spread of the virus—a complete lockdown—was what the Chinese government had done in Wuhan. It was clear the Indian government would also move in that direction since it was the intervention most countries affected by the virus were implementing. While people were just digesting the idea of a life with restrictions, the total surprise in India was the four-hour deadline with which the government imposed the lockdown on March 24. Everyone was caught completely unprepared.
Professionals instinctively knew that this drastic step would hurt the migrants the most, especially those working in the informal sector. Bihar was one of the largest contributors to this sector, and our organization World Health Partners (WHP) has a deep knowledge of the constituents’ psychographics since it has been working in the state for long. A significant proportion of WHP’s senior management comes from a large Bihar-based organization called Janani that has been running extensive programs in the state since the mid-1990s.
The bureaucracy showed itself at its dysfunctional worst—the short deadline combined with poor assessment of its implications on the population was at the core of what followed. The political leadership should have known the administrative deficiencies of the bureaucracy since two bold and major decisions in the recent past—demonetization and Good and Service Tax (GST) reform—were handled without a factor of anticipation so essential for decisions that impact at scale and beyond the line of sight. Even some union ministers expressed deep concerns about how such momentous decisions suffered from a lack of implementation skills of the executive. The bureaucracy committed a fundamental miscalculation here too in believing that a ‘command and control’ way of issuing official edicts would lead people to automatically fall in line and stay indoors. It was instinctively known, however, that it would not be the case. The administration also did not have a Plan B. A predominant proportion of migrants from Bihar support their families with daily wages, and once the revenue flow was disrupted, desperation set in quickly as they really did not have the option to stay indoors. Their natural reaction was to head back to their villages where there would be a modicum of social and economic security.
With no support system in place, each migrant family was left to its own devices with the clamor to reach their villages through whatever means or modes of transport that they could get—trucks, tractors and, most often, by foot. It was distressing to see women carrying small children walking miles each day with no assurance about where their food, water, shelter, and emergency care would come from. There was also no reliable arrangement to handle medical emergencies which are inevitable in such situations.
World Health Partners’ (WHP’s) team wanted to respond to this crisis immediately. The focus was on figuring out how medical support could be provided by using some applications already available in its arsenal. The main problem was that the tele-medicine platforms were designed with a mediator in mind—a village-level entrepreneur or an auxiliary nurse midwife (ANM) in a government facility—who would facilitate consultations with a remotely located doctor after registering patients and generating vital parameters such as temperature, blood pressure, and pulse.
The migrant population needed to have a modified system which would enable it to bypass intermediation and establish contact directly with doctors. Market research firm techARC in December 2019 estimated that over 23% of subscribers in India still used ‘feature’ or dumb phones so there was a need to tailor the platform in suitable ways so migrant communities, who are likely to fall into the non-smart phone category, can also access the consultations with whatever phone they possessed. Finally, the system should also offer as many services as possible free of charge given the disrupted economic conditions of the migrants. This meant that the calls and consultations could be free but there was no way of delivering medicines and undertaking laboratory investigations.
Resource Crunch
Many actions were set in motion within WHP as soon as the gravity of the situation became evident. The tele-consultation application was reconfigured in a record time of two days for a direct interface between the doctor and the patient without the need for real-time intermediation. A system also needed to be developed by which the call charges would not be passed on to the patient. WHP fortunately had an easy-to-remember number (80 10 11 12 13) already available which was quickly reactivated for receiving calls. The employees of WHP, stranded at home in various parts of the country, were brought in as assistants. Most of them had a company-issued laptop with access to the Internet so setting up the assistants’ network could be done easily. But they needed to be trained remotely. However, the problem was that WHP did not have enough doctors who could be deployed for this large-scale program nor did it have the resources to hire them. In a tele-medicine program, doctors account for almost two-thirds of the cost. The only option was to ask for volunteers.
Using various channels, WHP issued a call for volunteer doctors who could speak Hindi to offer their services from their homes. While WHP would not be able to pay for their services, its system would enable them to connect with the patients without incurring call charges. Reaching out to a number of NGO networks was relatively easy. All social media channels were used to announce the plan to reach out to migrants. Concurrently, WHP started fine-tuning an education software. This software was developed by Beaconpath Foundation, a non-profit sister organization that had been set up to deliver quality education to rural children through tele-education for remotely training participants in large batches.
WHP started providing consultations on April 4, 2020, with three doctors who had worked for the organization in the past and whose training needs were limited. But the general appeal for a larger number of volunteer doctors barely produced any results. In the meantime, the initial estimate that the virus would be brought under control within days or weeks was slowly being replaced with concerns of a long haul. The major question was how to sustain a program in the long term as getting volunteer doctors even for short-term work was so difficult. WHP needed to go back to the drawing board and rework the approach.
This is where WHP’s operational strategies guided the program. For sustaining programs at scale, WHP believes that there are only two options: (1) make services economically viable so the client can absorb the costs and the organisation does not require donor funds or (2) get support from the state’s health budget. External donors will at best be able to kick start projects in the early stages by providing support for capital costs but will not be interested in absorbing recurring costs. This is true even in normal times, and in an uncertain period, such as a pandemic, the hesitation is more pronounced. If the organization is not able to offset costs through contribution from patients, as was the case with the migrant populations uprooted from homes and short of resources, the only other option is to partner with governments that have the ability and inclination to find a quick solution through emergency funding. The capital costs for the tele-medicine solution were minimal since most of the solution was ready and WHP’s own technical team was contributing its time voluntarily to reconfigure the solution. However, the government’s help was needed to sustain the project. Partnerships with governments are not easy. In the case of migrants, there would also be jurisdictional problems as Bihari migrants, for instance, would be transiting through other states and so many support services cannot be organized in a coordinated way.
WHP Makes the First Move
WHP’s first step was to refocus the target segment. Instead of paying attention to migrant populations moving across the whole swath of north India, in each state the focus would be on populations stranded at home within which a special window would be created to engage with migrants entering the state. This meant, for instance, that the focus in Bihar would be to provide ambulatory or outpatient (OPD) care to the general population including migrants moving in from other parts of the country.
Adopting this line, mails were sent to various states including to the Health Ministries of Bihar, Andhra Pradesh, Tamil Nadu, Gujarat, and West Bengal. In Bihar, where WHP has had a long presence and had been dealing with many senior officials who knew WHP’s work closely, a dynamic Principal Secretary responded immediately and asked for a presentation to be made to him and to the minister to explain the plan. Andhra Pradesh was approached through a retired Health Secretary of the Government of India who currently lives in Hyderabad and has close links with the state ministry. In Tamil Nadu, the contact was a former Chief Secretary—the highest position for a bureaucrat in a state—who had worked with WHP on a kala azar (visceral leishmaniosis) project under a leave of absence some years ago. The senior-most officials in the Health Ministries of Gujarat and West Bengal were sent mails with copies marked to some influential persons working closely with the ministries.
The plan outlined was simple: The state governments should provide all the personnel from their pool of employees stranded at home, and WHP would set up a system by which it would provide consultations from its own locations. WHP would use its current set of hardware including servers, trunk lines, and mobile telephony to link up all those involved and would also modify the application to suit the COVID-19 situation.
WHP is an NGO that has extensive experience in handling infectious diseases at scale through its program focused on early detection and treatment of tuberculosis cases among the poor. WHP has found that stigma plays a critical role in dampening the response of the community to seek care for infectious diseases. Privacy for the individual and his/her family becomes crucial, and all care must be taken to ensure that the client feels reassured that the services provided are confidential. Following this norm was the main reason why WHP’s program raised the number of annual tuberculosis (TB) patients’ notifications from 4000 to 83,000 within four years in Bihar.
Right from the beginning, therefore, the approach was to offer ambulatory or outpatient care for common morbidities and use it as an opportunity to identify COVID-19 cases. Inviting persons to call up just for COVID-19 would not be appropriate because of people’s fears of being marked. Since both the migrants and the people locked down at home in any case needed access to medical help for common morbidities, it became the right platform for isolating cases as per the Indian Council of Medical Research (ICMR) guidelines.
The problem with the guidelines, however, was they went far beyond medical aspects to include factors related to behavioral elements such as international travel, contact with an infected person, working as a healthcare professional, and contact with hot spots. It was also clear that overloading the doctors with non-medical responsibilities during the consultation process would impose a huge burden and translate into a significantly higher cost. So, the application needed to be further repurposed to handle the consultations in two parts: divert callers to non-medical assistants first, and, on fulfilment of initial formalities and the capture of relevant data for registration, re-route the calls to the doctors. The assistants would take symptoms as well as behavioral details and feed them into the system which, using powerful algorithms, would generate differential diagnoses for the doctors by the time the calls moved to them. This arrangement would minimize the doctor’s time for each consultation which was necessary to bring a higher degree of efficiency. Another critical feature was a flashing alert the consulting doctor would receive on the screen to indicate, on the basis of what the non-medical assistants had gathered, whether the caller had shown some symptoms or risky behavior related to COVID-19. Depending on the severity, it would be either an orange or red alert. The solution was programmed to give an orange alert for meeting one criterion and a red alert for meeting two or more criteria.
It was also important for the assistants to obtain the precise location of the caller because any suspected COVID-19 case would be referred to the nearest government facility for follow-up action such as confirmatory testing, contact tracing, quarantine, and hospitalization. In consultation with the ministry, it was decided to instruct the doctors not to inform the patient if COVID infection was suspected to avoid unnecessary panic. The doctors would probe for possible COVID-19 and check a box in case infection was suspected. This information was incorporated into a master list and broken-down location-wise. And, the patient was sent to the nearest primary health center for follow-up care. In order to locate the patient precisely, the system needed to be loaded with geographical data in a drop-down form that showed villages, hamlets, and urban wards for retrieval in real time when a caller was being registered. It is a miracle that within one day, the team building technology-related solution within WHP was set up by which all such information could be uploaded into the system.
Bihar Responds First
WHP never received a response from the administrations in Tamil Nadu, Gujarat, and West Bengal but Bihar proved to be different. The lockdown in Bihar had led to a complete shutdown of OPD services in all government facilities. Fortunately, almost all the doctors and non-medical employees had access to computers and to the Internet which provided a wonderful platform to address the need. The Principal Secretary in Bihar moved very quickly and gave the requisite go-ahead starting with a comprehensive presentation to his whole team that would work with WHP in mounting the operation. Since WHP already had its own team in place in the state capital Patna, where it was implementing a major tuberculosis project, coordination was easy. Using the application developed for remote classrooms by the Beaconpath Foundation, its sister organization that worked on rural education, WHP, explained in detail the application to all in the ministry ranging from the minister to the officials who would take day-to-day decisions. Later, WHP’s team used a sophisticated briefing arrangement that the State Health Society had created for remote engagement with its officials to impart training.
Despite the urgency, however, the ministry was firm on formalizing the relationship to safeguard against any possible mishap. Work could not begin until this formal paperwork was completed. WHP was asked to produce the draft of an agreement which was circulated among various departments of the government for approval. Finally, a Memorandum of Understanding titled ‘Providing e-Teleconsultancy Services for Medical Advice’ was signed between WHP and the Government of Bihar on April 11, 2020. And, training sessions began immediately.
The government decided to deploy doctors and assistants from the district hospitals in two shifts since they were already on emergency duty but were not providing OPD services due to the lockdown. On the request of WHP to provide the personnel who would work on a fixed schedule, the ministry fixed the consultation hours from 8.00 am to 8.00 pm every day, Sunday included.
WHP created a special Web site whose details were sent to the doctors and assistants through the channels already available with the government. Training modules were prepared overnight, and the doctors and assistants were batched in groups of 50 for the training. Training was first given to the civil surgeons of all districts explaining the tele-consultation module and the role of each constituent. This became critical since the civil surgeons were tasked with follow-up services to COVID-19 suspects.
In its earlier attempts to integrate tele-medicine in government programs, WHP had faced the greatest resistance from doctors. In Bihar, doctors always showed a tendency for a high degree of absenteeism ostensibly because of their involvement in their own private practice. But COVID-19 had placed them in harm’s way since healthcare providers are among the most vulnerable to the virus. WHP felt this was a huge opportunity to digitize service delivery which in the post-COVID period would address a number of management problems that had been found to be intractable in the analogue world.
Training of the doctors and assistants went off smoothly. Since many parts of the solution were taken from the tried-and-tested application already in use for rural healthcare delivery, the interactions helped to lay down the foundation for intuitive solutions for the doctors and other personnel. The interest that the Health Minister showed provided the impetus for the team of officials to move forward rapidly and the project was formally launched on April 17, 2020.
WHP offered its own easy-to-remember number to the project (80 10 11 12 13), and the government released prominent advertisements in the largest circulating newspapers promoting the service. The response was instantaneous. Within the first week, this number received 11,830 calls. The system also needed to accommodate a number of features to ensure that the callers and providers did not incur any expenses for calls. Equally important was the need to manage the medical and support resources in a way that minimized waiting time for callers. WHP realized that while digital connectivity had many advantages, it also posed a major disadvantage for callers. Unlike patients waiting at the reception of a physical facility, the waiting time in a tele-medicine context was always magnified in the caller’s mind. It felt longer than what it really was since the caller had no other element distracting his or her attention.
While the project got off to a good start by eliciting a sizable response from the community, the old bugbear of the public sector—absenteeism—became a major hurdle. Even though 248 doctors and 260 assistants were enrolled through the website, very few would report for duty by logging in at the appointed time. Even worse, a number of them would log out within a few minutes without realizing that in a digital system every step was remotely trackable. While the assistants too showed indiscipline in this regard, it was the most pronounced among the doctors.
The call flow started in right earnest within a week when news about the service spread through word of mouth. While the attendants handled 99% of the calls, the doctors completed only 15% of the consultations. By five months, the project had received over 126,000 calls of which over 17,400 consultations were done and 272 suspects identified. There were two reasons for this dichotomy. A significant number of calls were just inquiring about symptoms, and only a few doctors logged in regularly during their scheduled hours to provide consultation. Both the senior administrators and WHP were concerned that the doctors’ unresponsiveness would automatically undermine the reputation of the project and result in tapering-off of calls in due course. The administration issued stern verbal warnings through the civil surgeons’ office to the doctors, and a formal notice was sent later that action would be taken for dereliction (Fig. 3.1).

Consultation process flow
Bihar had indicated right from the beginning that the state would not be able to bear the costs of servers and other hardware and expected WHP to absorb this cost. For WHP, this was an inopportune time since most of its projects had ended or were on the verge of ending and so it had limited resources. WHP made an urgent request to many donors and also requested the Bihar government to recommend its case to donors. Since the Gates Foundation had a large presence in Bihar and WHP had a strong relationship with the organization, there was a response by which a grantee, that had unspent money, was instructed to pay it to WHP to offset the costs.
Every consultation ended with a prescription being issued to the caller, and a medical record was created under a unique ID, in most cases the same as the mobile phone number. While persons using smartphones would get a regular prescription with doctor’s registration and qualification details as prescribed by law, the ones with non-smart feature phones would only get the highlights of the prescription consisting of name, diagnosis, and medicine details. A URL which was part of the message could be used by the caller to access the full prescription from the website. This information was needed because the callers had to buy the medicines from private pharmacies which fortunately were allowed to stay open during the lockdown.
A quick-to-access dashboard was created to give details in real time of the number of doctors and assistants who were logged in, the number of calls received and attended to, prescriptions issued, and COVID-19 suspects identified. Details of suspects with demographic and locational data were forwarded to the government for follow-up steps including confirmatory tests and contact tracing.
WHP implemented the project in earnest, and there was perceptible improvement of doctors’ and assistants’ participation as the project progressed but WHP staff were not sure whether the full potential was realized, especially in comparison with the Andhra Pradesh project where the same solution was used.
Chief Minister Gives the Push in Andhra Pradesh
The mail sent to a former Health Secretary to the Government of India, now retired and settled in Hyderabad, was the trigger that started the program in Andhra Pradesh. Within a day of sending the mail, WHP received a call from the Special Chief Secretary, Health, Medical and Family Welfare, who is the administrative head of the Ministry, asking about details of the WHP solution. Since Bihar had already started the program and WHP had a sense of what modifications were needed to make its application relevant in a public sector context, the presentation to the Andhra Pradesh ministry was highly focused on the problem and an effective solution.
Andhra Pradesh moved very fast because the Chief Minister took a keen interest in the Ministry’s planned response. WHP received the support of the Chief Minister who understood the need for providing comprehensive primary health care through a tele-medicine system and using the interface as an opportunity to isolate COVID suspects. The Chief Minister also authorized the release of medicines to the patients from the nearest primary health center of the government each of which, fortunately, already had access to the Internet so the prescriptions could be downloaded to cross verify the details when the patients presented their prescriptions. Initially, the medicine delivery success rate was around 63% because people needed to come to the PHC which could often be quite a distance away, making it difficult for a locked down population to negotiate. The Chief Minister, during his regular review, wanted to increase the delivery rate and ordered the involvement of the auxiliary nurse midwife (ANM) posted at the sub-center to enable doorstep delivery. The sub-centers are the last mile service delivery government resource and using them meant reconfiguring the solution accordingly.
Andhra Pradesh created a team of 435 doctors and 357 assistants who were largely drawn from a government-supported private network. This ensured a higher degree of efficiency since these personnel adhered to the schedule and also provided good quality services. WHP decided that the best way to train them would be in Telugu, but the only experienced WHP manager fluent in Telugu was located in Ahmedabad, Gujarat. WHP managed to rope in a Telugu-speaking retired engineer of the National Thermal Power Corporation (NTPC) residing in NOIDA as a volunteer. With the WHP support teams located in Faridabad, Haryana, Ghaziabad, Uttar Pradesh, and Delhi and the Andhra Pradesh, government’s supervisors located in Amravati and Vijayawada and the participants connecting from various interior districts, a new model of training emerged. Despite the initial glitches, mainly due to the Internet connectivity, the training program got off to a great start. Within three weeks, WHP organized 56 training sessions where 792 health personnel (435 doctors and 357 assistants) were trained.
All the training sessions were recorded and later reviewed with the supervisors to incorporate revisions which would improve their quality. The supervisors also conducted random surveys post-training to assess comprehension so more attention could be paid to the difficult parts. Since WHP did not have resources to hire servers and trunk lines, the Andhra Pradesh government, which runs a state-of-the-art data center in the state, stepped forward to provide these facilities. A technical team was appointed to coordinate with their counterparts in WHP so that all client-related data could be stored on the state-owned server. However, WHP had to maintain its application on its own server due to restrictions posed by use of third-party applications that did not allow sharing of the solution, under a contractual obligation.
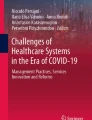
The involvement of the Chief Minister not only provided a great impetus to the project but his willingness to spend political capital on the approach resulted in the project being launched as ‘Dr. YSR Tele-medicine’ with a five-digit easy to remember number (14410) which was specially obtained by the government to ensure that the transition in a fully owned system could happen without problems in due course. The Andhra Pradesh tele-medicine project was launched at a special function by the Chief Minister on April 13, 2020. A dashboard was created which provided a quick overview of the number of calls received, consultations provided, and the number of COVID suspect cases who received free medicines from government facilities (Fig. 3.2).

Dashboard provided to state leadership to review project progress in real-time
The Andhra Pradesh project, despite receiving less number of calls, provided more consultations due to the availability of the doctors and the energy infused into the system by the direct involvement of senior leadership. The project until it was administered by WHP received 66,900 calls in five months. Over 33,500 (50%) were for consultation and 1,873 suspects were identified. Besides medical consultations for common morbidities, general counseling was provided to patients wanting information on COVID-19.
Since WHP could not transition its application to the Andhra Pradesh team, an arrangement was made by which the WHP’s team would provide the necessary support and guidance for the government’s special team to develop a solution. Since the processes were already under implementation, the government team had an easier task of identifying suitable software which could be duplicated. WHP also referred various third-party vendors whose solutions it had used in its application to enable the Andhra Pradesh government to expedite the development of its own solution. This process was finally completed by August after which WHP took on the role of providing advisory support to the project that had been transitioned to the government.
An important positive outcome of this exercise was that the Chief Minister became interested in digitizing the entire healthcare delivery system in the state for which a special six-member committee was set up. WHP was invited to join as a member of the committee. It was a high-level committee that included as its members the Executive Vice Chairman of Dr. YSR Aarogyasri Health Care Trust; CEO Real-Time Governance Society (RTGS), the Director of Public Health and Family Welfare (DPH and FW), an external public health specialist with deep interest in digital health systems, and the additional Chief Executive Officer (CEO), Dr. YSR Aarogyasri Health Care Trust.
Comparison of the Bihar and Andhra Pradesh Projects
While the Bihar and Andhra Pradesh projects were started almost at the same time during the nationwide lockdown, the Andhra Pradesh project showed better results in comparison with the Bihar project. Table 3.1 shows that the number of consultations in Andhra Pradesh was significantly higher than the number of consultations in Bihar even though Bihar received more calls.
Phase-Out
The Andhra Pradesh state government made all the arrangements with its own resources and also developed an application in coordination with the WHP team. The entire system of caring for patients remotely was transitioned smoothly by August 2020. WHP continued to provide advisory support but was not involved in operations.
The Bihar project took its time. Since WHP had run out of resources, it requested the state to take over the solution as had been done in Andhra Pradesh or allow WHP to close down the project since the government facilities had started functioning on a normal schedule. This permission was finally granted on October 19, 2020, which enabled WHP to close its emergency operation in Bihar on October 20, 2020.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2022 The Author(s)
About this chapter

Cite this chapter
Gopalakrishnan, G. (2022). Using Technology to Harness Existing Resources for an Emergency: COVID-19 Response. In: Pachauri, S., Pachauri, A. (eds) Health Dimensions of COVID-19 in India and Beyond. Springer, Singapore. https://doi.org/10.1007/978-981-16-7385-6_3
Download citation
DOI: https://doi.org/10.1007/978-981-16-7385-6_3
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-16-7384-9
Online ISBN: 978-981-16-7385-6
eBook Packages: Social SciencesSocial Sciences (R0)