
Abstract
Since many of the patients who receive adoptive immunotherapy also receive chemotherapy and/or radiation therapy, evaluation of the curative effect of adoptive immunotherapy itself is difficult. To overcome this, I perform immune monitoring to examine how much individual immunotherapies contribute to the curative effects. As a result, I found that higher whole blood levels of Th1 cytokines prodicing potential may be used to predict better clinical responses. In addition, I showed that the naïve T-cell adoptive therapy, which we developed, has superior clinical efficacy when compared to other immunotherapies. This chapter also describes the results of our clinical trial. In addition, I describe the application of hyperthermia, which can influence the immune-response of a tumor tissue. Basic experiments showed that hyperthermia could be applied to strengthen a patient’s immune system. Next, we performed naïve T-cell adoptive immunotherapy combined with hyperthermia. Finally, I will describe a case of advanced gastric cancer that showed complete remission after treatment with naïve T-cell adoptive immunotherapy combined with hyperthermia.
Similar content being viewed by others


Keywords
1 Immune Monitoring of Adoptive Cell Transfer (ACT) Immunotherapy
In our study, we demonstrated that adoptive T cell therapy had a strong potential to enhance whole blood production of the Th1 cytokine, interferon (IFN)-γ, in advanced pancreatic cancer patients in whom immunosuppression and immune escape mechanisms may be present [1]. Immune function was tested using venous blood obtained from patients prior to the administration of cultured cells (baseline) and during the follow up, which occurred 4 weeks after the 2nd and 6th cultured cell infusion. Methods for quantifying IFN-α production in whole human blood have been described previously [2]. Other cytokines were also quantified according to procedures described previously [3, 4].
A multivariate Cox proportional hazards analysis identified the increase of whole blood IFN- γ levels after adoptive T cell therapy as a predictive factor of the clinical response to the therapy; this factor was independent of the baseline IFN- γ levels and the performance status of the patients. Moreover, in agreement with previous studies [5–8], the number of peripheral regulatory T cells (Tregs) at baseline was an independent prognostic marker of overall survival (OS).
It is generally accepted that CD-8 T cell responses are an important indicator of the effectiveness of cancer immunotherapies, such as cancer vaccines. Immunological assays, such as the enzyme-linked immunospot (ELISPOT) assay or the human leukocyte antigen (HLA)-peptide multimer assay, are very efficient at detecting antigen-specific CD-8 T cells. Subsequently, they are frequently used to detect immunizing antigen-specific T cells after immunotherapy for validating surrogate endpoints that correlate with clinical outcomes. However, with a few exceptions, there have been poor correlations between the magnitude of the immunizing antigen-specific T-cell responses measured by these immunological assays and improvements in clinical outcomes [9, 10]. The most obvious explanation for this phenomenon is that the immune-monitoring assays measured irrelevant T-cell responses that had no effect on tumor destruction. Another possible explanation is that the assays were unable to detect how the T cells responded to different tumor-rejection antigens other than the immunizing antigen; this could result from immunotherapy-induced tumor lysis and endogenous priming with new tumor-derived antigens. Some recent immunotherapy trials have provided supporting evidence that the immunological phenomenon of determinant antigen or epitope spreading may play an important role in clinical responses to immunotherapy [9, 11, 12]. Butterfield et al. reported that new post-vaccine responses to non-vaccine antigens were observed in clinical responders, while non-responders did not display reactivity to epitopes other than those used for the vaccination [9, 12]. Although the ELISPOT and HLA-peptide multimer assays are quite efficient at detecting antigen-specific effector T cells, these assays are limited in their ability to assess post-immunotherapy responses to new tumor-derived antigens. To accurately predict clinical responses after immunotherapy, it is necessary to apply more comprehensive and functional assays in addition to these antigen-specific assays.
It is important to use structure-based assays, such as the HLA-peptide multimer assay, to dissect the antitumor responses and predict clinical outcomes after immunotherapy; it is also equally important to analyze the function of effector cells [13]. Analysis of the antigen-driven expression of cytokines can be used to determine the functional property of effector T cells. IFN-γ expression has been shown to be highly reproducible and sensitive enough to detect effector T-cell function [14]. Recently, June et al. have demonstrated that the clinical response of patients treated with genetically engineered T cells was accompanied by a delayed increase in the serum levels of cytokines, i.e., interleukin (IL)-6, IFN-γ, IL-8, and IL-10 [15, 16]. In their study, IFN-γ peaked on day 17 after adoptive cell therapy, when it showed the largest relative change when compared with baseline levels. This result in the study by June et al. showing that IFN-γ plays an important role in adoptive T-cell therapy emphasizes the relevance of our results.
The whole blood IFN-γ production assay used in our study has several advantages. Uno et al. reported that the value of IFN-γ production in whole blood often differs from that in peripheral blood mononuclear cells (PBMC). Serum factors, such as IL-10, can affect IFN-γ production. As IFN-γ production values that are determined from isolated PBMC would lack information about the influence of serum on the cells, our whole blood method is likely a more comprehensive tool for evaluating the actual immune responses of patients [17, 18]. Moreover, whole blood IFN-γ production assays are already available for immune monitoring of multiple cancer immunotherapies against unknown tumor antigens.
One of the limitations of our study is whether the increase in whole blood IFN-γ production truly reflected treatment-induced immune responses. Thus, when the immunogenic antigens are known, antigen-specific assays, such as ELISPOT or HLA-peptide multimer assays, should be used. This would allow researchers to assess the relationship between the assay results and whole blood IFN-γ levels to validate the reliability of the assay as a surrogate marker of clinical outcome. By combining whole blood IFN-γ assays and antigen-specific immunological assays, we believe it may be possible to construct a novel assay system for monitoring the immune response of patients to cancer immunotherapy. We demonstrated that adoptive T-cell therapy increased the whole blood level of the Th1 cytokine, IFN-γ, in advanced pancreatic cancer patients, who were in a strong immunosuppressive state. The increase in whole blood IFN-γ levels after adoptive T-cell therapy was shown to be independently related to OS in a multivariate Cox proportional hazards analysis. These findings indicated that the assay for whole blood IFN-γ levels offers promise as a convenient and efficient method for evaluating clinical responses to cancer immunotherapies.
2 Clinical Trial of Naïve T Cell Therapy
T-cell differentiation is a progressive process characterized by phenotypic and functional changes. Previous mouse studies and clinical trials have demonstrated that naïve and early differentiated T cells may be the optimal population for ACT-based immunotherapies due to their in vivo persistence, high proliferative potential, receptiveness to homeostatic and costimulatory signals, homing to secondary lymphoid tissues, and ability to secrete IL-2 [19–22]. In addition to this, Yu et al. have reported that a recombinant human fibronectin fragment, FN-CH296, acting with anti-cluster of differentiation (CD) 3 induces naïve and early differentiated T-cell proliferation. These evidences suggest that FN-CH296/anti-CD3 stimulation may be an efficient way to generate a large number of naïve and early differentiated T cells suitable for ACT with higher and longer persistence in vivo [23]. We built on these prior results by assessing the safety and efficacy of FN-CH296/anti-CD3-stimulated T-cell therapy, which we called naïve T-cell therapy, in patients with advanced cancer. The primary objective of this Phase I clinical trial was to assess the safety and adverse-event profiles of FN-CH296-stimulated T-cell therapy in patients with advanced cancer. Our secondary objective was to assess the antitumor activity of ACT therapy. This study was conducted with a standard 3 + 3 Phase I design that investigated the dose-limiting toxicities (DLTs) occurring over a 28-day period after the second infusion of cultured lymphocytes. We used an accelerated titration design to assess the safety of the number of adoptive lymphocytes at 1 × 109 (cohort 1), 3 × 109 (cohort 2), and 9 × 109 (cohort 3) lymphocytes per person. Written informed consent was obtained from all patients. This study is registered in the UMIN Clinical Trials Registry with the identifier UMIN000001835. Patients enrolled in this trial fulfilled the following eligibility criteria: histologically or cytologically confirmed esophageal cancer, gastric cancer, colorectal cancer, pancreatic cancer, biliary tract cancer, or non-small lung cancer; residual disease after standard treatment with no other curative treatment options available; a life expectancy of at least 3 months; and at least 4 weeks since their last chemotherapy or radiation therapy. Immune function was tested using venous blood obtained from the patients prior to the administration of cultured cells (baseline) and during the follow up, which occurred 4 weeks after the 2nd and 6th cultured cell infusion. Cytokine levels in the samples were measured with a Bio-Plex Multiplex Cytokine Array System (Bio-Rad Laboratories, CA, USA) according to the manufacturer’s instructions. The Multiplex Th1/Th2 Bead Kit (Bio-Rad Laboratories) was used to measure the following cytokines: IL-2, IL-4, IL-5, IL-10, IL-12 (p70), IL-13, tumor necrosis factor (TNF)-α, IFN-γ, and granulocyte-monocyte colony-stimulating factor (GM-CSF). Data acquisition and analysis were conducted with the Bio-Plex Manager Software, version 5.0. Since the levels of cytokines without PHA-P stimulation were extremely low (data not shown), we only assessed those with PHA-P stimulation in this study. The median age was 60 years (range, 43 to 75 years) and all patients had an ECOG performance score of 0 or 1. Three patients had colorectal cancer, two patients had bile duct cancer, and one patient each had pancreatic cancer, gastric cancer, hepatocellular carcinoma, or lung cancer. All patients underwent two infusions of cultured cells, and eight patients, who wished to continue treatment, completed four further T-cell infusions. Non-hematological events, including fatigue and anorexia, were observed, but no ACT-related severe or unexpected toxicities were observed. As for the clinical outcomes, of the nine patients, one (11.1%) exhibited complete remission (CR), one (11.1%) had partial remission (PR), four (44.4%) had stable disease (SD) and three (33.3%) had progressive disease (PD). The response rate was 22.2% and the disease control rate (DCR = CR + PR + SD) was 66.7%. To determine the immune responses in patients receiving novel ACT, whole blood cytokine assays were performed using venous blood obtained from the patients. The levels of IFN-γ treatment; in particular, the levels of IFN-γ, IL-12, and GM-CSF increased by a multiple of 10 or more times. Next, we evaluated whole blood cytokine levels according to objective tumor response. The levels of IFN-γ, IL-2, IL-12, and GM-CSF in patients with PR/CR increased by more than two times after the treatment, while the levels in patients with SD or PD decreased or did not change significantly after the treatment. The results presented in this study indicated that FN-CH296-stimulated T-cell therapy was very well tolerated in our patient sample. No significant ACT-related grade 3 or 4 adverse events occurred in any patient and the ACT resulted in tumor regression in two patients: CR in one patient with rectal cancer and PR in another with bile duct cancer. The response rate was 22.2% and the DCR was 66.7%. Despite the small size of the sample, these results are promising. Previous studies have demonstrated that IFN-γ plays an important role in cancer immunotherapy and IFN-γ expression in T cells is considered to be highly correlated with therapeutic success. We have also demonstrated that the assay of whole blood IFN-γlevels was an efficient method for evaluating clinical response to cancer immunotherapies [24, 25]. In this study, the whole blood IFN-γ levels in cohort 3 increased by up to 10 or more times after six infusions of cultured cells. Whole blood IFN-γ levels in PR or CR cases increased by more than two times, whereas those in PD or SD cases showed no significant increase after the treatment. The finding in our prior study [20] showing that the increase in whole blood IFN-γ levels after ACT was independently related to overall survival in cancer patients emphasizes the relevance of the results gained in this study. In addition to IFN-γ, the levels of other Th1 cytokines, such as IL-2, IL-12, and TNF-α, also increased in the patients of cohort 3 and in patients with PR/CR; in contrast, the levels of Th2 cytokines, such as IL-4, IL-5, and IL-13, decreased after the treatment. In addition, the whole blood GM-CSF level increased in the patients of cohort 3 and in patients who experienced PR/CR. It was previously reported that cell-mediated immunity is preferentially activated by Th1 cytokines, whereas Th2 cytokines suppress cell-mediated immunity [26]. GM-CSF is a pleiotropic cytokine that stimulates dendritic cells (DCs) and promotes the uptake of tumor antigens by DCs, leading to T-cell cross-priming and activation of the immune system against specific antigens [27]. Consequently, based on the results from the immune monitoring performed in this present study, we are inclined to believe that fibronectin CH296-stimulated T-cell therapy may exert anti-tumor effects by activating cell-mediated immunity.
3 The Effect of Hyperthermia on the Immune System
It has been shown that hyperthermia in the range of 39°C to 44°C can arrest cancer cell proliferation and kill cells in vitro and in vivo. The effects are dependent on two factors, namely, the temperature and duration of hyperthermia, which are collectively referred to as thermal dose [28]. When cancer cells are heated, the heat alters the characteristics of the membrane [29–31], proteins, which are the most sensitive biomolecules [28], and DNA repair mechanisms. A positive correlation between thermal dose and cytotoxicity has been known historically [32, 33], so it is believed that inducing hyperthermia by increasing the heating temperature results in an increased anti-tumor effect.
Recently, clinical local hyperthermia is used either for ablation purposes as an alternative to surgery or in combination with chemotherapy and/or radiation therapy to enhance the tumoricidal effects of those therapies [34]. It has been reported that many clinical cases treated with hyperthermia at the temperature of 39°C to 45°C showed unexpected benefits, including improvement of anti-tumor immunity [35]. As it has become apparent that activating the immune system is crucial to successfully treating metastatic cancer, the potential of boosting anti-tumor immunity by heating tumors has become a growing area of cancer research. In this section, several mechanisms by which heating tumors can elicit anti-tumor immune responses, including tumor cell damage, tumor surface molecule changes, production of heat-shock proteins (HSPs), and the direct effects on immune cells, are discussed.
It was becoming clear that different mechanisms of immune activation occur at different temperatures within the range of 39°C to 45°C. Hyperthermia can increase the visibility of tumor cells to the immune system. It was reported that heating tumor cells in vitro at 39.5°C for 6 h increased the surface expression of major histocompatibility complex (MHC) class I polypeptide-related sequence A (MICA), an NKG2D ligand, but not MHC class I, making the cells more sensitive to lysis by natural killer (NK) cells [36], and that tumor cells heated in vitro at 43°C for 30 min had increased surface MHC class I levels [37], which allows better recognition by CD8+ T cells.
It is well known that hyperthermia can induce HSPs in heated tumor tissue. These HSPs also contribute to hyperthermia-induced anti-tumor immunity. HSPs are usually divided into subgroups based on their molecular size. Among them, Hsp70 is the most recognized HSP that can stimulate the immune system. Hsp70 has an epitope that is recognized by NK cells and stimulates NK cell proliferation and cytolytic activities [38–40]. Hsp70 is also released by heat-stressed cancer cells and directly binds to toll-like receptor (TLR) 2 and TLR4 on antigen-presenting cells (APCs), such as DCs, to activate cytokine production and antigen uptake by the APCs [41–44]. HSPs can transfer potential tumor antigens to APCs [45]. It is reported that those APCs are able to cross-present tumor antigens from HSP complexes to CD8+ T cells via MHC class I and thus elicit tumor-specific CD8+ T-cell responses [46, 47].
When tumors are treated with local hyperthermia, tumor-infiltrating immune cells will also be exposed to heat. Fever is a natural immune stimulatory mechanism associated with fighting infections, so it is not surprising that fever-level hyperthermia has stimulatory effects on leukocytes. According to in vitro study results, heating human NK cells at 39.5°C for 6 h does not alter the surface expression level of NKG2D, but it does result in NKG2D clustering, as seen on NK cells activated with IL-2, leading to better lysis activity [36]. The results also showed that heating killer CD8+ T cells in vitro at 39.5°C for 6 h enhances their antigen-specific IFN-γ production and target tumor cell-killing ability [48]. Almost all relevant literature agrees that activation of immune cells by direct heating is only observed in the fever-range of temperatures, and not at higher temperatures above 41°C [49].
4 Combination Therapy with Hyperthermia and Naïve T Cell Therapy
It is likely that hyperthermia amplifies the effects of other immunotherapies, such as checkpoint blockade and adoptive T-cell therapies, as indicated by some studies [50]. Hyperthermia cannot always be applied uniformly when a cancer tissue is heated. Therefore, the actual immunological modification resulting from hyperthermia may differ depending on the intratumoral environment. Although uniform heating would be ideal, there are many factors, such as the blood flow inside of a tumor, which may prevent uniform heating.
Despite these challenges, we performed combined treatment of hyperthermia with the naïve T-cell adoptive immunotherapy that we developed. Similar to chemotherapy or radiotherapy patients, the patients treated with hyperthermia and naïve T-cell adoptive immunotherapy are often also treated with other therapies. However, the response rate, DCR, and overall survival period have yet to be sufficiently investigated to determine the validity of this combined therapy. Immune monitoring was performed in patients treated with naïve T-cell adoptive immunotherapy alone or with the naïve T-cell adoptive immunotherapy combined with hyperthermia. The methods of immune monitoring were the same as those mentioned above for the clinical trial on the naïve T-cell adoptive immunotherapy.
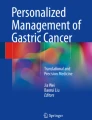
Whole blood cytokine assays were performed using venous blood obtained from the patients. We investigated 85 cases that were treated with the naïve T-cell adoptive immunotherapy alone, and 158 cases that were treated with the naïve T-cell adoptive immunotherapy combined with hyperthermia. First, we compared the carcinomas between the two groups. Figure 32.1 shows the levels of each cytokine; these were calculated as a ratio of the value measured 14 days after the 4th cultured cell infusion (10 weeks after the start of the naïve T-cell adoptive immunotherapy) to the baseline level measured before starting the naïve T-cell adoptive immunotherapy. Although the levels of IFN-γ, TNF-α, GM-CSF, and IL-4 were higher in the combination group when compared to the naïve T-cell adoptive immunotherapy alone group, the differences were not statistically significant.

Immune monitoring of cytokine levels in all cases. RIT: naïve T-cell adoptive immunotherapy, HT: hyperthermia (RIT alone: 85 cases, RIT + HT: 158 cases)
Next, we examined a hepatocellular carcinoma and a metastatic liver cancer. The levels of IFN-α, IFN-γ, TNF-α, and IL-5 were higher in the combination group when compared to those of the naïve T-cell adoptive immunotherapy alone group (Fig. 32.2). The levels of Th2 cytokines also increased slightly, likely in response to the increase in Th1 cytokines resulting from the naïve T-cell adoptive immunotherapy. When hypothermia was applied, the levels of each cytokine increased, although a similar pattern to that seen with the naïve T-cell adoptive immunotherapy alone was maintained. As mentioned above, the Phase I trial of our naïve T-cell adoptive immunotherapy showed that the levels of IFN-γ, IL-2, IL-12, and GM-CSF in patients with PR/CR increased by more than two times after the treatment, while the levels in patients with SD or PD decreased or did not change significantly after the treatment. Therefore, using hyperthermia together with naïve T-cell adoptive immunotherapy may contribute to a further improvement in tumor reduction. Effects on the overall survival period are presently under investigation.

Immune monitoring of cytokine levels in liver cancer cases. RIT: naïve T-cell adoptive immunotherapy, HT: hyperthermia (RIT alone: 6 cases, RIT + HT: 16 cases)
5 Case Presentation
The case of a patient with advanced gastric cancer, who rejected standard chemotherapy and received combined hyperthermia and naïve T cell transfer therapy is described herein. The patient was a 62-year-old man. He experienced abdominal discomfort and went to a clinic in his neighborhood. In that clinic, he underwent gastric endoscopy and computed tomography (CT). The results showed advanced gastric cancer with liver metastases and ascites. From a cytological examination of the ascites, the patient was diagnosed with peritonitis carcinomatosa. At first, he agreed to receive titanium silicate (TS)-1 + cisplatin combination therapy, which is a standard chemotherapy, and he received TS-1 for 1 week. However, he experienced very severe adverse effects and refused further chemotherapy. Thereafter, he received the naïve T cell transfer therapy once every 2 weeks and the hyperthermia therapy once a week from August 3rd, 2013, to March 17th, 2014. We performed gastric endoscopy and CT again on April 23rd, 2014. Surprisingly, the advanced gastric cancer and the ascites had completely disappeared. The liver metastasis was almost completely cured (Figs.32.3, 32.4). Two years after the initial diagnosis, the advanced gastric cancer, ascites, and liver metastasis remained undetectable as of April, 2015.

Gastric endoscopy image of the patient before and after 8 months of treatment with hyperthermia + naïve T-cell adoptive immunotherapy

Computed tomography image of the patient before and after 8 months of treatment with hyperthermia + naïve T-cell adoptive immunotherapy
References
Liyanage UK, Goedegebuure PS, Moore TT, et al. Increased prevalence of regulatory T cells (Treg) is induced by pancreas adenocarcinoma. J Immunother. 2006;29:416–24.
Uno K, Nakano K, Maruo N, Onodera H, Mata H, et al. Determination of interferon-alpha-producing capacity in whole blood cultures from patients with various diseases and from healthy persons. J Interferon Cytokine Res. 1996;16:911–8.
Ishikawa T, Kokura S, Sakamoto N, Matsumoto T, Funaki J, Adachi S, et al. Adoptive cellular therapy enhances the helper T cell response and reduces the number of regulatory T cells. Exp Ther Med. 2011;2:737–43.
Ishikawa T, Kokura S, Sakamoto N, Okajima M, Matsuyama T, et al. Relationship between circulating cytokine levels and physical or psychological functioning in patients with advanced cancer. Clin Biochem. 2012;45:207–11.
Liyanage UK, Moore TT, Joo HG, et al. Prevalence of regulatory T cells is increased in peripheral blood and tumor microenvironment of patients with pancreas or breast adenocarcinoma. J Immunol. 2002;169:2756–61.
Curiel TJ, Coukos G, Zou L, et al. Specific recruitment of regulatory T cells in ovarian carcinoma fosters immune privilege and predicts reduced survival. Nat Med. 2004;10:942–9.
Sasada T, Kimura M, Yoshida Y, et al. CD41CD251 regulatory T cells in patients with gastrointestinal malignancies: possible involvement of regulatory T cells in disease progression. Cancer. 2003;98:1089–99.
Kono K, Kawaida H, Takahashi A, et al. CD4(1)CD25high regulatory T cells increase with tumor stage in patients with gastric and esophageal cancers. Cancer Immunol Immunother. 2006;55:1064–71.
Butterfield LH, Ribas A, Dissette VB, et al. Determinant spreading associated with clinical response in dendritic cell-based immunotherapy for malignant melanoma. Clin Cancer Res. 2003;9:998–1008.
Ribas A, Timmerman JM, Butterfield LH, et al. Determinant spreading and tumor responses after peptide-based cancer immunotherapy. Trends Immunol. 2003;24:58–61.
Ranieri E, Kierstead LS, Zarour H, et al. Dendritic cell/peptide cancer vaccines: clinical responsiveness and epitope spreading. Immunol Invest. 2000;29:121–5.
Butterfield LH, Comin-Anduix B, Vujanovic L, et al. Adenovirus MART-1-engineered autologous dendritic cell vaccine for metastatic melanoma. J Immunother. 2008;31:294–309.
Yee C, Greenberg P. Modulating T-cell immunity to tumours: new strategies for monitoring T-cell responses. Nat Rev Cancer. 2002;2:409–19.
Kammula US, Lee KH, Riker AI, et al. Functional analysis of antigen-specific T lymphocytes by serial measurement of gene expression in peripheral blood mononuclear cells and tumor specimens. J Immunol. 1999;163:6867–75.
Porter DL, Levine BL, Kalos M, et al. Chimeric antigen receptor-modified T cells in chronic lymphoid leukemia. N Engl J Med. 2011;365:725–33.
Kalos M, Levine BL, Porter DL, et al. T cells with chimeric antigen receptors have potent antitumor effects and can establish memory in patients with advanced leukemia. Sci Transl Med. 2011;3:95ra73.
Uno K, Setoguchi J, Tanigawa M, et al. Differential interleukin 12 responsiveness for interferon gamma production in advanced stages of cancer patients correlates with performance status. Clin Cancer Res. 1998;4:2425–32.
Miyata H, Uno K, Ono T, et al. Low density lipoprotein apheresis ameliorates interferon- gamma production in patients with nephrotic syndrome. Ther Apher Dial. 2012;16:189–94.
Gattinoni L, Klebanoff CA, Palmer DC, Wrzesinski C, Kerstann K, et al. Acquisition of full effector function in vitro paradoxically impairs the in vivo antitumor efficacy of adoptively transferred CD8+ T cells. J Clin Invest. 2005;115:1616–26.
Robbins PF, Dudley ME, Wunderlich J, El-Gamil M, Li YF, et al. Cutting edge: persistence of transferred lymphocyte clonotypes correlates with cancer regression in patients receiving cell transfer therapy. J Immunol. 2004;173:7125–30.
Zhou J, Shen X, Huang J, Hodes RJ, Rosenberg SA, et al. Telomere length of transferred lymphocytes correlates with in vivo persistence and tumor regression in melanoma patients receiving cell transfer therapy. J Immunol. 2005;175:7046–52.
Huang J, Khong HT, Dudley ME, El-Gamil M, Li YF, et al. Survival, persistence, and progressive differentiation of adoptively transferred tumor- reactive T cells associated with tumor regression. J Immunother. 2005;28:258–67.
Yu SS, Nukaya I, Enoki T, Chatani E, Kato A, et al. In vivo persistence of genetically modified T cells generated ex vivo using the fibronectin CH296 stimulation method. Cancer Gene Ther. 2008;15:508–16.
Ishikawa T, Kokura S, Sakamoto N, Matsumoto T, Funaki J, Adachi S, et al. Adoptive cellular therapy enhances the helper T cell response and reduces the number of regulatory T cells. Exp Ther Med. 2011;2:737–43.
Ishikawa T, Kokura S, Sakamoto N, Okayama T, Endo M, et al. Whole blood interferon-gamma levels predict the therapeutic effects of adoptive T-cell therapy in patients with advanced pancreatic cancer. Int J Cancer. 2013;133:1119–26.
Romagnani S. Human TH1 and TH2 subsets: doubt no more. Immunol Today. 1991;12:256–7.
Metcalf D, Begley CG, Johnson GR, Nicola NA, Vadas MA, et al. Biologic properties in vitro of a recombinant human granulocyte-macrophage colony-stimulating factor. Blood. 1986;67:37–45.
Hildebrandt B, Wust P, Ahlers O, Dieing A, Sreenivasa G, Kerner T, et al. The cellular and molecular basis of hyperthermia. Crit Rev Oncol Hematol. 2002;43:33–56.
Vidair CA, Dewey WC. Evaluation of a role for intracellular Na+, K+, Ca2+, and Mg2+ in hyperthermic cell killing. Radiat Res. 1986;105:187–200.
Stevenson MA, Calderwood SK, Hahn GM. Effect of hyperthermia (45 °C) on calcium flux in Chinese hamster ovary HA-1 fibroblasts and its potential role in cytotoxicity and heat resistance. Cancer Res. 1987;47:3712–7.
Malhotra A, Heynen ML, Lepock JR. Role of extracellular calcium in the hyperthermic killing of CHL V79 cells. Radiat Res. 1987;112:478–89.
Sapareto SA, Dewey WC. Thermal dose determination in cancer therapy. Int J Radiat Oncol Biol Phys. 1984;10:787–800.
Lepock JR. Cellular effects of hyperthermia: relevance to the minimum dose for thermal damage. Int J Hyperthermia. 2003;19:252–66.
van der Zee J. Heating the patient: a promising approach? Ann Oncol. 2002;13:1173–84.
Frey B, Weiss EM, Rubner Y, Wunderlich R, Ott OJ, Sauer R, et al. Old and new facts about hyperthermia-induced modulations of the immune system. Int J Hyperthermia. 2012;28:528–42.
Ostberg JR, Dayanc BE, Yuan M, Oflazoglu E, Repasky EA. Enhancement of natural killer (NK) cell cytotoxicity by fever-range thermal stress is dependent on NKG2D function and is associated with plasma membrane NKG2D clustering and increased expression of MICA on target cells. J Leukoc Biol. 2007;82:1322–31.
Ito A, Tanaka K, Kondo K, Shinkai M, Honda H, Matsumoto K, et al. Tumor regression by combined immunotherapy and hyperthermia using magnetic nanoparticles in an experimental subcutaneous murine melanoma. Cancer Sci. 2003;94:308–13.
Multhoff G, Botzler C, Jennen L, Schmidt J, Ellwart J, Issels R. Heat shock protein 72 on tumor cells: a recognition structure for natural killer cells. J Immunol. 1997;158:4341–50.
Botzler C, Li G, Issels RD, Multhoff G. Definition of extracellular localized epitopes of Hsp70 involved in an NK immune response. Cell Stress Chaperones. 1998;3:6–11.
Roigas J, Wallen ES, Loening SA, Moseley PL. Heat shock protein (Hsp72) surface expression enhances the lysis of a human renal cell carcinoma by IL-2 stimulated NK cells. Adv Exp Med Biol. 1998;451:225–9.
Vabulas RM, Ahmad-Nejad P, Ghose S, Kirschning CJ, Issels RD, Wagner H. Hsp70 as endogenous stimulus of the Toll/interleukin-1 receptor signal pathway. J Biol Chem. 2002;277:15107–12.
Asea A, Rehli M, Kabingu E, Boch JA, Bare O, Auron PE, et al. Novel signal transduction pathway utilized by extracellular Hsp70: role of toll-like receptor (TLR) 2 and TLR4. J Biol Chem. 2002;277:15028–34.
Todryk S, Melcher AA, Hardwick N, Linardakis E, Bateman A, Colombo MP, et al. Heat shock protein 70 induced during tumor cell killing induces Th1 cytokines and targets immature dendritic cell precursors to enhance antigen uptake. J Immunol. 1999;163:1398–408.
Noessner E, Gastpar R, Milani V, Brandl A, Hutzler PJ, Kuppner MC, et al. Tumor-derived heat shock protein 70 peptide complexes are cross-presented by human dendritic cells. J Immunol. 2002;169:5424–32.
Suzue K, Zhou X, Eisen HN, Young RA. Heat shock fusion proteins as vehicles for antigen delivery into the major histocompatibility complex class I presentation pathway. Proc Natl Acad Sci U S A. 1997;94:13146–51.
Suto R, Srivastava PK. A mechanism for the specific immunogenicity of heat shock protein-chaperoned peptides. Science. 1995;269:1585–8.
Binder RJ, Srivastava PK. Peptides chaperoned by heat-shock proteins are a necessary and sufficient source of antigen in the cross-priming of CD8+ T cells. Nat Immunol. 2005;6:593–9.
Mace TA, Zhong L, Kokolus KM, Repasky EA. Effector CD8+ T cell IFN-gamma production and cytotoxicity are enhanced by mild hyperthermia. Int J Hyperthermia. 2012;28:9–18.
Ostberg JR, Repasky EA. Emerging evidence indicates that physiologically relevant thermal stress regulates dendritic cell function. Cancer Immunol Immunother. 2006;55:292–8.
Bear AS, Kennedy LC, Young JK, Perna SK, Mattos Almeida JP, Lin AY, et al. Elimination of metastatic melanoma using gold nanoshell-enabled photothermal therapy and adoptive T cell transfer. PLoS One. 2013;8:e69073.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer Science+Business Media Singapore
About this chapter
Cite this chapter
Kokura, S. (2016). Combination of Hyperthermia and Immunotherapy: Hyperthermia and Naïve T-cell Therapy. In: Kokura, S., Yoshikawa, T., Ohnishi, T. (eds) Hyperthermic Oncology from Bench to Bedside. Springer, Singapore. https://doi.org/10.1007/978-981-10-0719-4_32
Download citation
DOI: https://doi.org/10.1007/978-981-10-0719-4_32
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-10-0717-0
Online ISBN: 978-981-10-0719-4
eBook Packages: MedicineMedicine (R0)