
Abstract
This paper aims to present the prevalence and trends of adolescents’ risky behaviours in Bulgaria over a 13-year period (2006–2018). Current tobacco smoking, drinking and alcohol abuse, current cannabis use, early sexual experience, and aggression towards schoolmates (bullying and fighting at school) are in the focus of research interest, using national representative data from the three waves (2006, 2014, 2018) of the Health Behaviour among School-Aged Children (HBSC) study. The descriptive and multivariate analysis reveals trends of decrease in smoking tobacco, excessive alcohol consumption (drunkenness), involvement in a physical fight, and the early start of sexual life as well as trends of an increase in regular alcohol consumption and cannabis use in a lifetime across the years. Additionally, the family context is a significant gradient in defining the prevalence of adolescents’ risk behaviours, in particular adolescents living in one-parent families and coming from high FAS families in Bulgaria are more likely to report risky behaviours compared to young people from low FAS families. The last part of the paper discusses the key areas for policy intervention in youth health and wellbeing in Bulgaria.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
- Adolescent risky behaviours
- HBSC-Bulgaria
- Trend analysis
- Family context
- Youth health and wellbeing programs
1 Introduction
The health and health status of children and young people is a foundational element of the quality of life and future generations’ wellbeing (UNICEF 2011). Today’s young people may expect to live longer than ever before, the prevalence of chronic illnesses in the 16–29 age group is lower than those in older groups with a higher self-rated health perception of youngsters: 91 % of the EU-28 young people at age 15–24 years reported that they were in good or very good health in 2016 (Eurostat 2017). However, the conceptualization of health not merely as a lack of illness but as physical, psychological, and social wellbeing assumes that youth’s health behaviours and health outcomes have to be seen in a broader social context of young people’s lifestyles. Prevention of diseases and promotion of healthy lifestyles and healthy environments are stated as key objectives in the EC strategic documents: EU public strategy ‘Health Programme’ (Multi-annual programme of EU action in the field of health for the period 2014–2020 (Regulation EU N 282/2014))Footnote 1 and the European Commission Youth—Discover EU’s Role—EU Youth Strategy—Health and Wellbeing websiteFootnote 2. Recognizing the unique psycho-social conditions of adolescence, the recent WHO documents ‘Investing in Children: the European Child and Adolescent Health Strategy’ (WHO 2014a), ‘Health for the World’s Adolescents: A Second Chance in the Second Decade’ (WHO 2014b) and ‘Global Strategy for Women’s, Children’s and Adolescents’ Health’ (WHO 2015) direct public attention and policy actions to this specific age group. Issues of health inequalities, mainly based on socioeconomic circumstances, have also been a focal point in public policies in order to facilitate better health and secure wellbeing for young people.
Among factors related to socioeconomic circumstances, tobacco and drug use, alcohol consumption, reduced physical activity, unhealthy eating habits, involvement in violence resulted in physical injuries, and early start of sexual activityFootnote 3 are of special importance for providing safe and healthy lifestyles for young people. From an individual perspective, the regularity of risky behaviours during adolescent age could impede physical, social, and emotional wellbeing later in young adults’ lives (Kann et al. 2018).
Adolescence has been recognized as a ‘second birth,’ a period when young people gain new experiences and social relations. Increased emotional intensity, social engagement, novelty-seeking, and creative explorations are key features of adolescents’ perceptions of the world, which implicates both mental excitement and mental confusion (Siegel 2014). Embedded in physiological changes in the brain around puberty (Steinberg 2008), sometimes adolescents’ risk-taking behaviours lead to long-standing habits resulting in nicotine, alcohol, and drug addictions. On the other hand, despite the adverse health effects, adolescents develop risky behaviours as a coping mechanism to reduce school stress and boredom, make contacts with the opposite gender and peers, boost their self-esteem, and get accepted as mature and self-reliant companions.
Recent studies on adolescent health apply a socio-ecological model through which an interaction of factors explains risky behaviours at five levels: individual, interpersonal, institutional/organizational, community and public policy (McLeroy et al. 1988; McLaren and Hawe 2005). Individual-level factors (for example, gender, age, life satisfaction, etc.) are related to adolescents’ developmental, psychological and behavioural characteristics. At the interpersonal level, adolescent health and health behaviours are influenced by relationships with family members, classmates, peers, and other regular social contacts. The institutional/organizational level involves factors within an institution/organization that impact on adolescent health. Findings from previous HBSC studies have shown that school policies regarding nutrition, physical activity, prevention of violence, use of harmful substances, etc. significantly impact students’ healthy and risky behaviours (Currie et al. 2008). The community-level involves the relationships between organizations, social networks, norms, and practices related to promoting healthy behaviours, e.g., the availability of sport and recreation venues such as sports clubs, parks, sports grounds, etc. to stimulate physical activity of the young people. The most general level of public policies concerns the policies, regulations, and laws aiming to create and support healthy environments (Subramanian et al. 2003), e.g., existing national policies to implement dietary food at school canteens and programs to increase sports activities.
The main objectives of this paper are:
-
To describe and evaluate the prevalence and trends of adolescents’ risky behavioursFootnote 4 in Bulgaria over a 13 year period (2006–2018);
-
To estimate the relationships between health risk behaviours, individual-level factors (gender, age) and some interpersonal level factors, mainly from the family domain (family structure and family affluence);
-
To present the country-level policies and some strategic programs that aim to improve young people’s health in Bulgaria.
The analysis is based mainly on the data from the Bulgarian samples of the Health Behaviour among School-aged Children (HBSC) study. HBSC is a large-scale international study conducted under the World Health Organization aegis every four years since the start of the 1980s in multiple European and North American countries. Students aged 11, 13, and 15 years fill out self-assessing questionnaires at school (with parents’ consent) and provide information on different aspects of health and health behaviours and their family, school, and peers. The HBSC study assets provide a broad set of representative data for the target population with an internationally standardized and validated questionnaire that makes possible cross-national comparative analyses. Despite the collection of large cross-national data over a 30 year period, the HBSC study faces methodological limitations concerning the self-reported data that may imply overreporting or underreporting on some sensitive topics at the adolescent age and cross-sectional type of the data that impedes a causality analysis.
In Bulgaria, the HBSC study was conducted three times in the following waves: 2005/2006, 2013/2014, and 2017/2018Footnote 5. Although the waves do not cover three successive surveys, the time period covers a ten-plus-year period that allows monitoring and evaluating trends of adolescent health and health behaviours. The same sampling procedure (based on a random sampling of schools and classes in the 28 country’s regions), as well as the use of identical questions and responses/categories across survey years, provide the data quality for sufficient trend analysis (Schnohr et al. 2015).
HBSC indicators on risk behaviours and statistical analysis
For this analysis, we use questions on current cigarette smoking, current alcohol consumption, lifetime drunkenness, participation in physical fights and bullying perpetration at school, cannabis use during the last 30 days, and early start of sexual life.
The HBSC study involves the question of current smoking “How often do you smoke tobacco at present?” with four categories ‘every day’, ‘less than once a week,’ ‘at least once a week but not every day,’ ‘don’t smoke.’ Weekly smoking combines the first two answers.
The question used for risky alcohol consumption concerns beverage-specific use: “At present, how often do you drink anything alcoholic, such as beer, wine, spirits (like rakia, vodka, whisky, tequila), alcopops, any other drink that contains alcohol?” with five options: ‘every day,’ ‘every week,’ ‘every month,’ ‘rarely,’ ‘never.’ The weekly alcohol use combines the two answers: ‘everyday’ and ‘every week.’ The second indicator used for alcohol misuse is drunkenness in a lifetime “Have you ever had so much alcohol that you were really drunk in your lifetime?” with the categories ‘no, never’, ‘yes, once,’ ‘yes, 2–3 times’, ‘yes, 4–10 times’, ‘yes, more than 10 times’.
We use current (last 30 days) prevalence for cannabis use as one of the most spread illicit substance in adolescent age “Have you ever taken cannabis?” with the scope of frequency: ‘never,’ ‘1–2 days’, ‘3–5 days’, ‘6–9 days’,’10–19 days’, ‘20–29 days’ and ‘30 days or more’. Only 15-year old students answer this question.
An indicator for the students’ sexual initiation is the question, “Have you ever had sexual intercourse?” with two options: ‘yes’ and ‘no.’ The question is asked only to 15-year old participants.
Two questions are used for youth violence and bullying. The first question indicates the prevalence of the students’ participation in a physical fight “During the past 12 months, how many times were you in a physical fight?” with answers ‘I have not been in a physical fight in the past 12 months’, ‘1 time’, ‘2 times’, ‘3 times’ and ‘4 times or more’. The presented proportions of the students who have participated in a physical fight at least 3 times include the last two responses. The frequency of bullying perpetration (bullying others) at school is measured by the question “How often have you taken part in bullying another student(s) at school in the past couple of months?” with the options: ‘I have not bullied another student(s) at school in the past couple of months,’ ‘It has only happened once or twice,’ ‘2 or 3 times a month’, ‘About once a week,’ ‘Several times a week.’ The presented proportions of the students who have bullied 2–3 times a month comprise the last three responses.
We apply logistic regression models to test the difference between the waves in the prevalence of risky behaviours. In these models, we test the effect of the time when the survey was conducted, and we also control for gender, age, family structure, and family affluence. Family structure is created as a composite measure and includes the following categories: students who live with two parents, students who live with one parent, and students who live with other relatives or in a child home/foster care. Family affluence is assessed through the Family Affluence Scale (FAS III)—a brief assets-based measure including 4 items: number of computers owned by the family, number of cars, number of travels/holidays abroad, having an own bedroom. The total scale score ranges from 0 to 9, with scores 0–3 representing the category of families with low affluence, the scores 4–6—the families with medium affluence, and the scores 7–9—the families with high affluence.
2 Findings
2.1 Prevalence of Risky Behaviours Across the Survey Waves, by Age and Gender
Current tobacco smoking
Findings in Fig. 1 demonstrate a steep growth of the proportion of weekly smokers by age with a crucial transition between the ages of 13 and 15 when their share increases three-four times. A positive statistically significant trend has been observed for a decline of the share of regular smokers among 15-years olds between the three waves, especially for girls, while for the boys, the percentage remains almost the same between 2014 and 2018. Gender differences present a higher prevalence in girls’ weekly smoking, and this trend remains across the three HBSC waves.

(Source: HBSC-BG 2006, 2014, 2018. Own calculations)
Adolescents who reported smoking at least once a week, by age and gender (%).
Current alcohol consumption and excessive drinking
Findings in Fig. 2 show that the prevalence of weekly alcohol consumption increases with age, particularly for boys between ages 13 and 15. Overall, weekly drinking is more typical for boys with gender differences greater than ten percentage points for all ages. Alcohol prevalence among Bulgarian boys and girls (significant for both genders at p < = 0.001) increases significantly in 2018 with clearly indicated growth for girls.

(Source: HBSC-BG 2006, 2014, 2018. Own calculations)
Adolescents who reported drinking alcohol at least once a week, by age and gender (%).
Data presented in Fig. 3 shows that the prevalence of getting drunk in a lifetime (on two or more occasions) increases with age, particularly between 13 and 15 years. Boys report having been drunk more often than girls. However, gender difference diminishes over the years as the proportions of boys who report excessive drinking decrease significantly, unlike the increasing proportion of girls who experiment with excessive alcohol consumption. There is a time trend of a decrease in alcohol abuse among 13- and 15-year olds and a slight increase among 11-year old students.

(Source: HBSC-BG, 2006, 2014, 2018. Own calculations)
Adolescents who reported to have been drunk on two or more occasions, by age and gender (%).
Current cannabis use
Findings presented in Fig. 4 show the proportions of Bulgarian adolescents at the age 15 who had used cannabis on at least one day during the last 30 days (current use). There is a steep increase in current cannabis use over the survey years, which is significant for both genders.

(Source: HBSC-BG, 2006, 2014, 2018. Own calculations)
15-year old adolescents who reported using cannabis in the last 30 days, by gender (%).
Age of initiation of risky behaviours—first cigarette, first alcohol drink and first drunkenness
The age of initiation of risky behaviours is of crucial importance for the design of intervention programs that should approach adolescents. Data presented in Figs. 5 and 6 show that the key age for the beginning of the most prevalent risky behaviours—smoking tobacco and alcohol consumption is 14 years for both boys and girls. For girls, there is a second peak at the age of 15.

(Source: HBSC-BG, 2006, 2014. No data available for 2018. Own calculations)
Initiation of risky behaviours for boys (%).

(Source: HBSC-BG, 2006, 2014. No data available for 2018. Own calculations)
Initiation of risky behaviours for girls (%).
Sexual initiation
Data in Fig. 7 shows that boys are more likely to report having had sexual intercourse. Gender disparities remain across the survey waves. A significant decrease in the reported sexual onset is observed between 2006 and 2018 for both genders and a slight increase for girls between 2014 and 2018.

(Source: HBSC-BG, 2006, 2014, 2018. Own calculations)
15-year old students who responded “yes” to having had sexual intercourse, by gender (%).
Youth Violence
Findings in Fig. 8 show the proportions of those who reported physical fighting involvement three times and more for the last 12 months. The proportions tend to decline significantly with age and over time, particularly for boys. However, for girls who have been less involved in physical aggression, there is a significant increase in the proportions in 2018.

(Source: HBSC-BG, 2006, 2014, 2018. Own calculations)
Adolescents who have been involved in a physical fight at least 3 times in the last 12 months, by age and gender.
Bullying perpetration
Data presented in Fig. 9 show that the proportions of students who have bullied other(s) at school at least 2–3 times a month increase over time. Changes across survey waves are observed with the highest prevalence at the age of 13 for boys and girls. Generally, bullying perpetration is significantly higher for boys, but girls’ participation in bullying has increased across survey waves.

(Source: HBSC-BG, 2006, 2014, 2018. Own calculations)
Adolescents who have bullied other(s) at school at least 2–3 times in the past couple of months, by age and gender.
2.2 Multivariate trend analysis of risky behaviours
On Table 1 we present the results from logistic regression analysis of the time trends in young people’s risky behaviours. Apart from the study’s wave, in the models, we control for age, gender, and family structure, and family affluence.
The models’ results reveal significant changes over time in the prevalence of certain risky behaviours among young people in Bulgaria. There is a statistically significant decrease in smoking tobacco, excessive alcohol consumption (getting drunk), involvement in a physical fight and the early start of sexual life compared to the first wave of HBSC in 2006 (reference year). Trends of a significant increase in regular alcohol consumption and cannabis use in a lifetime have also been observed.
Gender differences are statistically significant for five of the studied risky behaviours. The multivariate analysis results reveal that the odds of regular alcohol consumption, alcohol abuse (getting drunk), early start of sexual life, physical fight and bullying perpetration is significantly lower for girls than boys (reference category). The likelihood of smoking tobacco is significantly higher for girls. In the case of current cannabis use, gender differences are not statistically significant.
The effect of age reveals that the prevalence of cigarette smoking, regular alcohol consumption, getting drunk and bullying perpetration significantly increases with age. The effect is negative only in the case of physical fights.
There is a statistically significant relationship between the studied risky behaviours and family structure. The students who live in a one-parent family and a family of their relatives or in foster care are more likely to report that they smoke cigarettes, regularly drink alcohol, get drunk, have risky sexual behaviour and are aggressive towards others in school compared to those who live with both parents (reference category).
Family affluence is also significantly associated with some of the adolescents’ risky behaviours. The students from high FAS families are more likely to report that they regularly drink alcohol, have an early start of sexual life, use cannabis and show aggressiveness at school (bullying perpetration and participation in physical fights) compared to young people from low FAS families (reference category).
3 Discussion
The frequency of risky behaviours in Bulgarian adolescence over 13-years period of time indicates a chronic prevalence of unhealthy activities. Between one-third and one-fourth of schoolchildren aged 11–15 years report having been involved in tobacco smoking, alcohol use and abuse, cannabis use, early unsafe sexual experience, participating in physical fights and bullying others at school. From a cross-national perspective, the Bulgarian adolescents outnumber most of their peers in the other countries participating in HBSC and typically occupy the first ten risky behaviours (Inchley et al. 2016; Inchley et al. 2020b).
Over the years, trend analysis demonstrates a significant decrease in adolescents’ current cigarette smoking, excessive alcohol use, involvement in a physical fight, and sexual activity before age 15 and an upward trend of adolescents’ regular alcohol consumption and drug use.
From a cross-national perspective, despite the substantial decline of adolescent smoking for the last 30 years in the European countries, the prevalence of regular smokers among 15-years old Bulgarians is very high. Bulgaria leads the ranking out of 44 countries in cigarette smoking in the last 30 days—38 % of Bulgarian girls and 26 % of Bulgarian boys at the age of 15 report weekly smoking in 2018 (Inchley et al. 2020b, p. 92). According to the European Health Interview Survey (2014), 36 % of men and 21 % of women in Bulgaria are daily smokers, representing along with Cyprus (38 %) and Latvia (37 %) the largest proportion of regular smokers among the EU countries (National Statistical Institute 2019, p. 99). The Eurostat data reveal a high prevalence of daily smoking among Bulgarian men aged 15–24 (Eurostat 2017). These data confirm that adolescence is a crucial time for tobacco initiation and nicotine addiction that may be difficult to quit in adult life (WHO 1996).
Although HBSC survey waves reveal a trend of decline of regular drinking among boys and girls in the European region (Inchley et al. 2018b), drinking, including binge drinking, is still widespread among Bulgarian adolescents. Bulgarian 11- and 13-years olds report the highest share of current (last 30 days) alcohol consumption and 15-olds occupy the 6th position by this indicator in the international ranking (Inchley et al. 2020b, p. 82–83). Although Eurostat data show that in later age 15–24 years olds Bulgarians are not among the leaders in alcohol consumption (Eurostat 2017), Bulgarian adolescents rank on some of the first places by the prevalence of drunkenness at least twice in a lifetime. The frequent and excessive use of alcohol in adolescence may have adverse effects on young people’s physical and mental health and is associated with low academic achievements, more aggression, deviant behaviours at school, drug use (Kuntsche et al. 2012; Kuntsche and Gmel 2013) and unplanned and risky sex (Cooper 2002).
Cannabis, as the most frequently used drug by young people in Europe, is a risk factor for behaviour problems and mental disorders at this age (Inchley et al. 2018a). Trend analysis displays an expansion of the current use (last 30 days) of cannabis with a statistically significant increase between 2014 and 2018. Bulgarian students top rank the countries by this indicator (Inchley et al. 2020b, p. 95). Cannabis initiation and its regular use in adolescence is associated with dropouts and low school performance, unsafe sex, aggression and delinquency, anxiety and depression, cognitive disorders and brain deterioration (Kokkevi et al. 2006; Volkov et al. 2014). However, Eurostat data for cannabis use at the next age group (15–24 years) places Bulgaria among the countries with a low prevalence (Eurostat 2017).
Sexual health is part of adolescents’ social and personal wellbeing. The analysis across years presents a statistically significant downward trend of adolescent sexual activity. However, the Bulgarian 15-year old boys outnumber their coevals in most countries participating in the last wave of HBSC by this indicator (Inchley et al. 2020b, p. 76). We may consider that boys’ data on reported sexual onset is partially biased due to the adolescents’ aspirations to be perceived as mature men. On the other hand, Eurostat data reveal one of the highest proportions of abortions and births at the under the age of 20 years in Bulgaria (Eurostat online database. Section “Abortion indicators”Footnote 6). Early unprotected sex has its potential risks on adolescent physical and mental health: its effects are related not only to the risk of unintended pregnancy and induced abortion but as well as to sexually transmitted infections with a long term effect on reproductive health, emotional wellbeing, self-perception and social status of young people (Spriggs Madkour et al. 2010). Bacalso and Mihajlović (2018) draw the conclusion relevant to Bulgaria’s case that the high age barriers in accessing sexual and reproductive health services are contrary to the often lower age of consent to sexual relationships and even marriage at younger ages.
Physical fighting is the most vivid display of youth aggression and is considered an indicator of multiple risk behaviours (Sosin et al. 1995). Trend analysis for adolescents’ participation in physical fights reveals a statistically significant decrease in Bulgaria’s youth violence over the 13 years. In 2018 Bulgarian 15- and 13-year olds rank in the 9th position and 11-year olds—in the 14th position by involvement in a physical fight at least three times in the past 12 months (Inchley et al. 2020b, p. 106–107).
Trend analysis for bullying perpetration does not present substantial changes over the survey years. In a cross-national comparison, 11-year olds occupy the 3rd rank, 13-year olds—the 4th rank, and 15-year olds—the 5th rank by bullying others at least twice in the past couple of months (Inchley et al. 2020b, p.100–101). The high prevalence of bullying at school among Bulgarian adolescents is a major concern for public health as young people’s aggression is associated with other risky behaviours such as alcohol and drug use, alienation from school life, and lower overall life satisfaction, etc. (Walsh et al. 2013).
Gender differences are a substantial gradient for risky behaviours, with boys outnumbering girls in all risky behaviours, except cigarette smoking. There is a pattern of increasing the share of girls’ unhealthy behaviours over the years, especially in alcohol and drug consumption and aggression at school. The age of 14 is crucial for the onset of risky behaviours for both genders.
Cross-comparative data from Eurostat on the proportions of regular smoking, alcohol consumption, and drug use at the age of 15–24 show that Bulgarian young people continue unhealthy activities initiated during adolescent years. This effect is especially true for smoking tobacco that started in adolescent years and became a daily habit for 26 % of Bulgarian males aged 15–24. By this indicator, Bulgaria ranks among the countries with the highest proportion of male daily smokers.
The HBSC study applies a socio-ecological model where health behaviours and health outcomes are influenced by social, psychological, and ecological factors. Macro-level influences, including economic, political, cultural and environmental factors, are essential gradients of the socio-ecological model of understanding adolescents’ health and wellbeing. At the micro-level, the main determinants of adolescents’ health are delineated through social settings/contexts approach, including the effects of family, peers, and school.
Family structure and family affluence turn to be strongly associated with schoolchildren’s risky behaviours. Adolescents living in one-parent families or in families with relatives have higher odds of risky behaviours. Our previous studies (Dimitrova and Kotzeva 2009) prove that social support, close relations with the parents and high satisfaction with family life have a preventive effect on schoolchildren’s risky behaviours.
Family affluence is another significant gradient in defining the prevalence of risk behaviours. The multivariate statistical analysis shows that young people from high FAS families in Bulgaria are more likely to report that they regularly drink alcohol, have an early start of sexual life, use cannabis and show aggressiveness at school (bullying perpetration and physical fights) compared to young people from low FAS families. These results correspond to our previous findings (Dimitrova and Kotzeva 2019), which reveal that young people from high-status families are more likely to report certain types of risky behaviours. An association between the prevalence of risky behaviours and high affluence families is mostly found for the Baltic countries (Zaboriskis et al. 2006), unlike most West European countries where risky behaviours are more associated with lower socioeconomic status (Currie et al. 2012).
4 Youth Policy and Intervention Strategies in Bulgaria
Survey data, including HBSC data, have served as a valuable source for setting up policy agendas and developing evidence-based strategies and programs directed towards improving adolescents’ health and wellbeing in Bulgaria. The National Health Strategy (2014–2020)Footnote 7, esp. policy direction 7 “Effective functioning of maternal, child and school healthcare” and the auxiliary National Program for the Improvement of Maternal and Child Health (2014)Footnote 8 are the main policy-driven documents based on the European framework “Investing in Children: the European Child and Adolescent Health Strategy 2015–2022 (The WHO Regional Office for Europe)” and on the UN Convention on the Rights of the Child (General comment N 20 (2016) on the implementation of the rights of the child during adolescence).
Based on evidence-informed and rights-based principles the country-level health documents are directed to supporting growth during adolescence, reducing exposure to violence and risk, achieving a tobacco-free millennial generation, promoting healthy nutrition and physical activity, tackling depression and other mental problems in adolescence, addressing the unfinished agenda of preventable death and infectious diseases (Dimova et al. 2018).
The key areas for improving health literacy and health promotion for young people are risky behaviours, obesity, sexual and reproductive health, aggression and violence and mental health, with a special focus on at-risk groups, including the Roma community. In Bulgaria, state-run institutions and NGOs support policies and enhance programs responsive to adolescents’ needs and capacities and enable effective participation of young people in policy implementation. Among such programs is the national student contest ‘Missioners of health’ launched in 2018 by the Ministry of Health in partnership with other governmental and non-governmental organizations such as WHO’s office for Bulgaria and the Bulgarian Red Cross Youth. The contest aims at encouraging more schools to be involved in the initiative to raise schoolchildren’s health literacy concerning tobacco and alcohol abuse, unhealthy eating, and reduced physical activity.
The reduction of risk factors such as tobacco smoking and alcohol abuse is a priority of health promotion and health education programs in Bulgaria. Although smoking is banned in public spaces by the Health Act, tobacco advertising is prohibited, alcohol and cigarettes are not sold to people under the age of 18, the restrictions are often violated, and smoking is highly tolerated in public, including the increasing habits of smoking water pipes, which are equally toxic as smoking regular cigarettes. The effective intervention programs against drug abuse and addictions should be based not only on information campaigns but on improving coordination between school authorities and police to stop the illegal spread of drugs near schoolyards.
Sexual and reproductive health education exists as an option in a few schools in Bulgaria. Adolescents, especially from marginalized social groups, face barriers to access medical advice on contraception and abortion. At the EU baseline, the country has a high rate of abortions and births under the age of 18, making programs to reduce inequalities and transform gender violence between adolescent boys and girls crucial. The National Centre for Public Health and Analyses (NCPHA) promotes youth empowerment through sexual and reproductive health and rights, gender equality, and peacebuilding programs. In partnership with the International Institute for Youth Development PETRI, UNFPA, and Youth Peer Education Network (Y-PEER), PETRI-Sofia CenterFootnote 9 provides peer-to-peer education using alternative education methods (theatre-based techniques, role games, simulations), organizes meetings, and builds an international network of young volunteers and experts.
The NCPHA completed the project “Improved mental health services” with the sponsorship of EEA grantsFootnote 10. The project activities comprise training and online educational programs for general practitioners, psychologists, and social workers in primary care to detect anxiety and depression and suicidal symptoms. Other activities include organizing public campaigns to increase people’s sensitivity to mental health issues and media specialists’ training on how to cover the topic.
Another important area for policy interventions is combatting violence in adolescent age. ‘Childhood without violence’ CoalitionFootnote 11 comprises 20 NGOs and academic representatives aiming to build up public intolerance and change attitudes toward violence. In cooperation with parents and children and professionals working with children, the NGOs activists work on creating sustainable public services and measures to protect children against violence, developing of instruments for detection and reporting about children at risk, providing advocacy for changes in legislation and policies, organizing information and awareness campaigns and mapping the situation through research studies.
5 Conclusion
The surveys’ findings show that some of the risk-taking behaviours started during adolescence as part of youth culture of experimentation, mood improvement and peers’ appreciation, relevant for ‘fruit-bearing age,’ but they may lead to substance addiction and chronic physical, social and psychological problems in adult life. Additionally, risky and unhealthy behaviours are observed simultaneously, producing multiple risk-taking. The policy agenda of national programs should address the health risk multiplicity and involve teachers, parents, NGOs, and young people to coordinate and unify different stakeholders’ efforts to encourage healthy lifestyles for young people.
The school environment is of paramount importance to health promotion and building up healthy habits among schoolchildren, but health education is not a substantial gradient of school curricula in Bulgaria. There is a considerable need for an increase of social workers, psychologists, and special needs assistants at schools as a strategy to tackle aggression and bullying and as a way to monitor students’ mental health and personal development. Providing more opportunities for extracurricular activities for sports, art, social volunteering, and school community building are tools to achieve resilience to unhealthy behaviours and stimulate young people’s capacities to establish rewarding relationships with others and develop pro-social lifestyles.
Notes
- 1.
https://ec.europa.eu/health/funding/programme_en (Accessed 24.09.2021).
- 2.
https://ec.europa.eu/youth/policy/youth-strategy/health-wellbeing_en (Accessed 24.09.2021).
- 3.
The Centre for Disease Control (CDC) has suggested six primary domains of risk among youth and young adults: tobacco use, alcohol and illicit substance use, sexual behaviour related to unintended pregnancy and sexually transmitted infections, injury-prone and violent behaviour, unhealthy dietary patterns, and physical inactivity (Kann et al. 2018).
- 4.
We refer to a scope of risky behaviours as they are defined according to the HBSC methodology (Inchley et al. 2018a).
- 5.
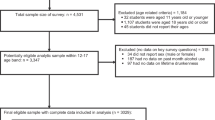
The sample size of the HBSC respondents is 4854 in 2005/2006, 4796 in 2013/2014 and 4548 in 2017/2018. In the last wave of the survey the response rate for the three age groups is 60.3 % for 11-year olds, 68.1 % for 13-year olds, and 65.1 % for 15-year olds.
- 6.
https://ec.europa.eu/eurostat/databrowser/view/demo_fabortind/default/table?lang=en (Accessed—24.09.2021).
- 7.
- 8.
- 9.
http://petri-sofia.org/en/homepage/ (Accessed 24.09.2021).
- 10.
http://bgmental.ncpha.government.bg/bg (Accessed 24.09.2021).
- 11.
http://endviolence.bg/ (Accessed 24.09.2021).
References
Bacalso, C. & Mihajlović, D. (2018). Age Matters! Understanding age-related barriers to service access and the realization of rights of children, adolescents and youth. Final Synthesis Report. UNICEF: Youth Policy Labs.
Cooper, ML. (2002). Alcohol use and risky sexual behavior among college students and youth: Evaluating the evidence. Journal of Studies on Alcohol, Suppl. 14: 101–117.
Currie, C., Nic Gabhainn, S., Godeau, E., Roberts, C., Smith, R., Currie, D., Pickett, W., Richter, M., Morgan, A. & Barnekow, V (Eds.) (2008). Inequalities in young people’s health: HBSC international report from the 2005/06 Survey. Health Policy for Children and Adolescents, No. 5. Copenhagen: WHO Regional Office for Europe.
Currie, C. et al. (Eds.) (2012). Social determinants of health and wellbeing among young people. Health Behaviour in School-aged Children (HBSC) study: international report from the 2009/2010 survey. Copenhagen: WHO Regional Office for Europe; 2012 (Health Policy for Children and Adolescents, No. 6).
Dimitrova, E. & Kotzeva, T. (2009). Risk behaviors of the Bulgarian school-aged children: family predictors and determinants. In: Bulgarian Journal of Psychology. The South-East Regional Conference of Psychology “South Eastern Europe Looking Ahead: Paradigms, Schools, Needs and Achievements of Psychology in the Region. Sofia, Bulgaria, 30–1 Nov 2009, Is.3–4, pp. 43–55.
Dimitrova, E. & Kotzeva, T. (2019) Socio-economic Inequalities and Risk Behaviors among School-aged Children in Bulgaria: Results of the HBSC. Sociological Problems. Special Issue “How We Live Together: Communities, Institutions, Networks, 51, 2019, ISSN:0324-1572, 102–124.
Dimova, A., Rohova, M., Koeva, S., Atanasova, E., Koeva-Dimitrova, L., Kostadinova. T. & Spranger, A. (2018). Bulgaria: Health system review 2018. Health Systems in Transition, 20(4): 1–256.
European Commission. EU Health Programme (Multi-annual programme of EU action in the field of health for the period 2014–2020 (Regulation EU N 282/2014)). https://ec.europa.eu/health/funding/programme_en (Accessed 24.09.2020).
European Commission. Youth—Discover EU’s Role—EU Youth Strategy—Health and Well-being website. https://ec.europa.eu/youth/policy/youth-strategy/health-wellbeing_en, (Accessed 24.09.2020).
Eurostat (2017). Being Young in Europe Today—Health. Data extracted in December 2017. https://ec.europa.eu/eurostat/statistics explained/index.php?title=Being_young_in_Europe_today_-_health#Health_status, (Accessed 24.09.2020).
Inchley, J., Currie, D., Budisavljevic, S., Torsheim, T., Jåstad, A., Cosma, A. et al. (Eds.) (2020a). Spotlight on adolescent health and wellbeing. Findings from the 2017/2018 Health Behaviour in School-aged Children (HBSC) survey in Europe and Canada. International report. Volume 1. Key findings. Copenhagen: WHO Regional Office for Europe. Licence: CC BY-NC-SA 3.0 IGO.
Inchley, J., Currie, D., Budisavljevic, S., Torsheim, T., Jåstad, A., Cosma, A. et al. (Eds.) (2020b). Spotlight on adolescent health and wellbeing. Findings from the 2017/2018 Health Behaviour in School-aged Children (HBSC) survey in Europe and Canada. International report. Volume 2. Key data. Copenhagen: WHO Regional Office for Europe. Licence: CC BY-NC-SA 3.0 IGO.
Inchley, J., Currie, D., Cosma, A. & Samdal, O. (Eds.). (2018a) Health Behaviour in School-aged Children (HBSC). Study Protocol: background, methodology and mandatory items for the 2017/18 survey. St Andrews: CAHRU.
Inchley, J., Currie, D., Vieno, A., Torsheim, T., Ferreira-Borges, C., Weber, M., Barnekow, V. & Breda, J. (Eds.). (2018b). Adolescent alcohol-related behaviours: trends and inequalities in the WHO European Region, 2002–2014. Observations from the Health Behaviour in School-aged Children (HBSC) WHO collaborative cross-national study.
Inchley, J., Currie, D., Young, T. et al. (Eds.). (2016). Growing up unequal: gender and socioeconomic differences in young people’s health and wellbeing. Health Behaviour in School-aged Children (HBSC) study: international report from the 2013/2014 survey. Health Policy for Children and Adolescents, No. 7. Copenhagen: WHO Regional Office for Europe.
Kann, L., McManus, T., Harris, W.A., Shanklin, S.L., Flint, K.H., Queen, B., Lowry, R., Chyeu, D., Whittle, L., Thornton, J., Lim, C., Bradford, D., Yamakawa, Y., Leon, M., Brener, N. & Ethier, K.(2018). Youth risk behavior surveillance—United States, 2017. Morbidity and Mortality weekly Report—Surveillance Summaries. 67(8): 1–114. Published online 2018 Jun 15. doi: https://doi.org/10.15585/mmwr.ss6708a1, (Accessed 24.09.2020).
Kokkevi, A., Nic Gabhainn, S., Spyropoulou, M. & the Risk Behaviour Focus Group of the HBSC. (2006). Early initiation of cannabis use: A cross-national European perspective. Journal of Adolescent Health, 39(5): 712–719.
Kuntsche, E., Rossow, I., Simons-Morton, B., ter Bogt, T., Kokkevi, A. & Godeau, E. (2012). Not early drinking but early drunkenness is a risk factor for problem behaviors among adolescents from 38 European and North American countries. Alcoholism: Clinical and Experimental Research, Volume first published online 2012.
Kuntsche, E. & Gmel, G. (2013). Alcohol consumption in late adolescence and early adulthood—Where is the problem? Swiss Medical Weekly, 143, p. w13826 https://doi.org/10.4414/smw.2013.13826, (Accessed 24.09.2020).
McLaren, L. & Hawe, P. (2005). Ecological perspectives in health research. Journal of Epidemiology & Community Health, 59 (1): 6–14. doi: https://doi.org/10.1136/jech.2003.018044.
McLeroy, KR., Bibeau, D., Steckler, A. & Glanz, K. (1988). An ecological perspective on health promotion programs. Health Education Quarterly 15: 351–377. doi: https://doi.org/10.1177/109019818801500401.
Marmot, M. (2009). Social determinants and adolescent health. International Journal of Public Health, 54(2): 125–127.
National Statistical Institute. (2019). Sustainable Development in Bulgaria 2005–2016. Sofia: NSI.
Schnohr, W., Molcho, M., Rasmussen, M., Samdal, O. et al. (2015).Trend analyses in the health behaviour in school-aged children study: methodological considerations and recommendations. European Journal of Public Health, vol.25, Supplement 2: 7–12.
Siegel, D. (2014). Brainstorm. The Power and Purpose of the Teenage Brain. Tarcher Perigee.
Sosin, DM., Koepsell, TD., Rivara, FP. & Mercy, JA. (1995). Fighting as a marker for multiple problem behaviors in adolescents. Journal of Adolescent Health, Mar:16(3):209–15.
Spriggs Madkour, A., Farhat, T., Halpern, CT., Godeau, E. & Nic Gabhainn, S. (2010). Early adolescent sexual initiation and physical/psychological symptoms: a comparative analysis of five nations. Journal of Youth and Adolescence, 39(10): 1211–1225.
Subramanian, SV., Jones, K. & Duncan, C. (2003) Multilevel methods for public health research. Kawachi I, Berkman LF, (Eds.). Neighborhoods and Health [Internet]. Oxford: Oxford University Press: 65–111.
Steinberg, L. (2008). A social neuroscience perspective on adolescent risk-taking. Developmental Review 28: 78–106.
UNICEF. (2011). The State of the World’s Children. Adolescence: an age of opportunity. New York, United Nations Children’s Fund. https://www.unicef.org/publications/index_57468.html, (Accessed 24.09.2020).
Volkow, ND., Baler, RD., Compton, WM. & Weiss, SR. (2014). Adverse health effects of marijuana use. New England Journal of Medicine, 370(23): 2219–2227.
Walsh, SD., Molcho, M., Craig, W., Harel-Fisch, Y., Huynh, Q., Kukaswadia, A. et al. (2013). Physical and emotional health problems experienced by youth engaged in physical fighting and weapon carrying. PLoS One. Feb 21; 8(2):e56403.
World Health Organization (1996). Tobacco, alcohol and illicit drugs. WHO Fact Sheet No. 127.
World Health Organization (2014a). Investing in children: the European child and adolescent health strategy 2015–2020. Copenhagen: WHO Regional Office for Europe. http://www.euro.who.int/en/health-topics/Life-stages/child-and-adolescent-health/policy/investing-in-children-the-european-child-and-adolescent-health-strategy-20152020, (Accessed 24.09.2020).
World Health Organization (2014b). Health for the World’s Adolescents: A second chance in the second decade. Geneva, World Health Organization. https://www.who.int/maternal_child_adolescent/documents/second-decade/en/, (Accessed 24.09.2020).
World Health Organization (2015). The Global Strategy for Women’s, Children’s and Adolescents’ Health (2016–2030). Geneva: World Health Organization. https://www.who.int/life-course/publications/global-strategy-2016-2030/en/, (Accessed 24.09.2020).
Zaboriskis, A., Sumskas, L., Maser, M. & Pudule, I. (2006). Trends in drinking habits among adolescents in the Baltic countries over the period of transition: HBSC survey results 1993–002. BMC Public Health 6:67 doi:https://doi.org/10.1186/1471-2458-6-67.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Open Access Dieses Kapitel wird unter der Creative Commons Namensnennung 4.0 International Lizenz (http://creativecommons.org/licenses/by/4.0/deed.de) veröffentlicht, welche die Nutzung, Vervielfältigung, Bearbeitung, Verbreitung und Wiedergabe in jeglichem Medium und Format erlaubt, sofern Sie den/die ursprünglichen Autor(en) und die Quelle ordnungsgemäß nennen, einen Link zur Creative Commons Lizenz beifügen und angeben, ob Änderungen vorgenommen wurden.
Die in diesem Kapitel enthaltenen Bilder und sonstiges Drittmaterial unterliegen ebenfalls der genannten Creative Commons Lizenz, sofern sich aus der Abbildungslegende nichts anderes ergibt. Sofern das betreffende Material nicht unter der genannten Creative Commons Lizenz steht und die betreffende Handlung nicht nach gesetzlichen Vorschriften erlaubt ist, ist für die oben aufgeführten Weiterverwendungen des Materials die Einwilligung des jeweiligen Rechteinhabers einzuholen.
Copyright information
© 2022 Der/die Autor(en)
About this chapter

Cite this chapter
Kotzeva, T., Dimitrova, E. (2022). Risk Behaviours: Tracking Youth Health and Well-Being in Bulgaria 2006–2018. In: Heinen, A., Samuel, R., Vögele, C., Willems, H. (eds) Wohlbefinden und Gesundheit im Jugendalter. Springer VS, Wiesbaden. https://doi.org/10.1007/978-3-658-35744-3_30
Download citation
DOI: https://doi.org/10.1007/978-3-658-35744-3_30
Published:
Publisher Name: Springer VS, Wiesbaden
Print ISBN: 978-3-658-35743-6
Online ISBN: 978-3-658-35744-3
eBook Packages: Social Science and Law (German Language)