
Abstract
The accessibility to safe drinking water is a major challenge India faces as a developing nation. The condition is grimmer in rural areas where only 45% of the population has access to clean drinking water, a number significantly low when compared to urban areas (79%). The issue has become relevant and will continue to do so in the coming years as more and more water sources get contaminated with both biological and chemical pollutants. Annually, 1.5 million children die from diarrhoea after consuming contaminated water. Despite various technological breakthroughs and innovations, especially involving nanomaterials, the research benefits have not been percolated to the vulnerable communities at the Bottom of the Economic Pyramid (BoP). Experience suggests that this can be achieved through innovative approaches on behaviour change, service delivery models and sustainable supply chains. Technology and Action for Rural Advancement (TARA) and Development Alternatives (DA) are involved in ensuring access to safe water to the BoP through testing innovative delivery models. The action research tested the potential for scalability of these sustainable and affordable solutions for a wider dissemination in the BoP market. Based on the end-user preference, the Tata Group introduced a product, Tata Swach filter, at an affordable rate of Rs. 999. Through design and implementation of a sustainable supply chain mechanism, the demand for the Swach filter has increased exponentially with consumers placing immediate orders for its procurement. The chapter will further elaborate on the features of the supply chains, delivery models, drivers and barriers within the larger scheme of sustainability.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others



1 Background
About 884 million people worldwide do not have access to safe drinking water and are, therefore, forced to consume water that has high concentrations of bacteria, viruses, protozoa or even chemical contaminants. As a result, more than 4000 children die every day from diarrhoea (WHO 2011). 80% of the water-borne diseases in developing countries originate from microbiological contamination.
Over the past few years, private market actors such as Hindustan Unilever Ltd., Tata Chemicals, PATH, Aquatabs, Antenna Technologies, Procter & Gamble, TARA water services, Water Health International, Naandi have come up with promising technological solutions such as silver-impregnated nano-technology-based water filters, membrane filters, chlorine solution and tablets, water kiosks based on UV and membrane filters, slow sand filters, etc., for low-income customers. It is widely recognised that new and emerging technologies such as nano-based water filtration, have the potential to service this population due to their high efficacy, low-material intensity and cost (Development Alternatives, May 2011).
Despite the availability of various technologies in the market to deal with the water quality, the benefits have not percolated down to the 835 million strong BoP population in India (Vijaya Lakshmi et al. 2011; 2013), who live on an annual income of less than INR 200,000 (<US$3000). It becomes imperative to offer them affordable yet effective solutions for water purification. These solutions often do not reach the BoP segment due to high cost of the filters, lack of awareness and demand for safe water and irregular supply of products and after-sales services. Thus, any innovation needs to address these issues in order to ensure adoption and sustained demand. To ensure the long-term viability and sustainability of these models, it is essential to develop them in consideration with the socio-economic status of the community and market conditions in the area including the study of the flow of finance in those markets.
There is sporadic evidence that technology research benefits can reach the BoP, through innovative and appropriate delivery models (TARA 2012). In view of the same, Development Alternatives (DA) Group has piloted an action research for ensuring access to safe water to the BoP through testing innovative delivery models using nano-technology-based filters. The action research looked into testing its scalability potential and associated barriers of these models for a wider dissemination of these products in BoP market.
2 Piloting the Delivery Models
2.1 Technology Selection Process
Based on the readiness to be taken to the market in terms of economics and availability of product, an initial scan resulted in the short listing of technologies for the pilot. Five technologies made the cut based on performance, ease of use and wow factors. It was decided to include the end-user in the final selection since it was a market-based model. During the consultations with target end users, the filters and their associated features were demonstrated to the residents. The feedback from the group helped analyse and rank the selection criteria for the users. These are categorised as critical and important factors in decision-making for the residents are listed in Table 12.1.
The decision in Table 12.2 shows the mapping of various technology options against the above factors. The possible lists of three filters tested from the matrix are
-
(a)
Swach Smart filter
-
(b)
Tulip Siphon filter
-
(c)
ARCI candles with container model filter.
On the overall product deliverables across all factors, service capabilities and probability of product continuity, Tata Swach Smart filter was selected for pilot testing in Delhi and Bundelkhand.
2.2 Demand Creation for Safe Water in the Study Area
As anticipated, there was a lack of awareness of the need for safe water in many households. Even where there was recognition for the need of safe water, it rarely converted into a priority due to a slew of reasons ranging from competing priorities, to the lack of awareness about options or the lack of acceptance that their water was not safe. The perception of safe water is closely tied to appearance, taste and smell. The families who opted for safe water, they bought water from the local RO vendor. In order to encourage behaviour change, several promotional activities were conducted using street plays, door-to-door visits, leaflets, posters and banners containing information on the possible impacts of drinking contaminated water and benefits of using Swach filters.
2.3 Innovations in Delivery Model
2.3.1 Lead Experience User (LEU) Model in Delhi
Bacterial contamination is one of the largest problems in urban slums in India. The quality of water supplied or sourced in these areas is secondary contamination due to unsanitary and unhygienic living conditions. Delhi is no stranger to this problem (Kumar 2013).
DA has developed an innovative approach to reach the BoP in two urban slums of Delhi, i.e. Mandanpur Khadar and Ambedkar Camp. The technology selected for the pilot was nano-silver-based Swach filters. A peer influence-based model was adopted. The pilot was implemented in two slums, Madanpur Khadar in South East Delhi (15,000 HHs) and Ambedkar Camp in South West Delhi (3000 HHs). The average monthly income of a household in both the slums vary from Rs. 5000 to Rs. 10,000. In Madanpur Khadar, the primary source of water is hand pumps, used mostly for cooking and washing. Some families also use it for drinking. Majority of the residents rely on the so-called filtered water or packaged mineral water from the local RO plants in the area. These residents are provided with door-to-door services at prices as low as Rs. 2 per litre of RO water. Ambedkar Camp residents mainly rely on water tankers supplied by the Delhi Jal Board (the city water supply system). The main concern for water quality in these areas was bacterial contamination.
-
Service Delivery Model
A LEU is a local housewife willing to be a Swach Champion. Swach is presently being sold based on two distinct distribution models, i.e. direct selling to local Swach champions and the distributor model shown in Fig. 12.1. Based on the local market conditions and taking into account the existing distribution channels for Swach, a LEU model was adopted. The model builds on the existing distribution channels but enables last mile delivery to a previously sub-serviced population. The LEU cuts through the long-winded distribution chain and obtains filters at a discount to ensure access of the slum population to a filter. This modified delivery model was chosen for the pilot due to a number of different reasons. First, there was no requirement of working capital to implement the model. Second, there was already a linkage with the existing distributor of Tata and local delivery by these distributors. In addition, this model allowed for direct activation and training by Tata Chemicals as well as access to free servicing by Swach service executives.
Fig. 12.1 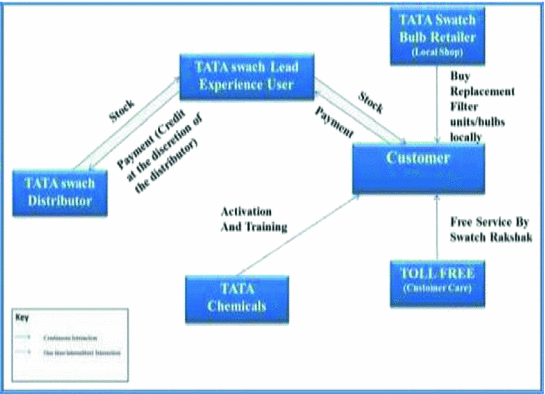
LEU model schematic for Tata Swach

The two elements of the model which make it distinct from the existing distributor model, is access to a local LEU and the use of local retailers to stock and sell replacement units and bulbs were also important reasons for this model being chosen. The model considers local retailers to distribute the replacement filter units/bulbs as these agents have their own pre-existing relationships with clients, which they are able to leverage in order to make sales. Second, it requires little to no working capital and the margins will be suitably high as compared to the other products that they stock, making them a good investment.
Financing was a critical element to consider, given the low-income levels of the BoP population. Following the research of the pilot area however, the cost of the filter at Rs. 900, was not considered to be prohibitively expensive and would not deter residents from purchasing the product. Although it was understood that providing financing options would increase the rate at which the filters were adopted, as there were no financing organisations working in that area, the decision to provide financing as part of the model was not built into the model.
-
On the Ground Activities
In order to reach the maximum number of households in the study areas and to test the workability and potential scalability of the model, following processes were taken up.
-
(a)
Selection and Activation of Lead Experience Users (LEUs): LEUs are local women/housewives who are interested in becoming entrepreneurs. Given the socio-cultural environment in villages, LEUs are a vital component as they have good knowledge of the local people and existing networks in place, credibility as a user, and thus ability to demonstrate the long-term benefits of using the filter.
-
(b)
Training sessions were conducted for LEUs to orient them to the product and its features. This is also essential for effective communication of the services being offered to the community. Initial on-field support was given to LEUs by experienced marketing professionals. The idea was to assist the SHG members so that they are confident to continue the activity in long term.
-
(c)
Financial incentives were offered to the LEUs, so they could create a sustainable business from the activity. LEUs were able to purchase the filters from Tata Swach for the reduced cost of Rs. 799. The filter was then sold at the market price of Rs. 899 to the customers, leaving the LEUs with a profit of Rs. 100.
-
(d)
On-field Promotion and Demonstration: A separate team of demonstrators was recruited for running live group demonstrations on the streets outside the homes.
-
(e)
Delivery and Post Delivery: A daily tracking system was developed to track record of houses visited, hot leads identified and sales of the filter. The date of booking was recorded to help the LEUs determine the date of bulb replacement. Customers were given a toll free number of Swach filter in case of any issues.
-
Lessons Learnt
-
Need for Financial Incentives: As per our initial research, there was no apparent requirement of financial incentives as the product fell in an affordable range for the consumers in urban slums. However, it was realised that affordability never ensured acceptance and adoption of the product. In some cases, they were used as small ticket payments (INR 5 for 10 L of water delivered at home) for their daily quota of water from a local RO supplier. Consumers preferred making daily payments to purchase water daily instead of paying a bulk amount for a filter which proved to be expensive in the long run with compromised water quality. Thus, in order to encourage adoption of water filters, the need for financial incentives was felt. But the absence of microfinance institutions in the study area, however, prevented this intervention.
-
Technologies need to be customised: While the purification technology is not an aspect that has a major bearing on the consumers decision-making, the term RO (reverse osmosis) has become a household name. It has acquired a brand value people associate with purity, even though it may not be a reputed company or product. There are local vendors riding this wave and supplying sub-standard water to communities, as seen in Madanpur Khadar. In addition, the raw water TDS levels in Madanpur Khadar are high and have an impact on taste, even though they are well within permissible limits as per the BIS standards. Due to access to demineralized water (even though it may not be bacteria free) from the local RO plants people have acquired a different taste. The perception of safe water is so directly linked to taste that some families rejected the Swach filter on this account. This issue was not faced in Ambedkar Camp, where the raw water TDS levels were lower and did not distort taste.
-
Need for Behaviour Change Communication for Demanding Safe Water: As expected, there was a lack of awareness on the need for safe water in many households. Even where there was recognition for the need of safe water, it rarely converted into practice due to a variety of reasons ranging from differential priorities, to the lack of awareness about options or the lack of acceptance that their water was not safe. Also, the perception of safe water is closely tied to appearance, taste and smell. The families who opted for safe water, bought water from the local RO vendor. In order to encourage behaviour change, several promotional activities were conducted using street plays, door-to-door visits, leaflets, posters and banners containing information regarding the possible impacts on health by drinking contaminated water and highlighting key features of Swach filters.
-
Designing robust business models and entrepreneurship development for Supply Chains: Discovering and nurturing entrepreneurship is not an easy task, more so in areas where women are not considered at par with men. Initial efforts of recruiting women as LEU, who have experience in promoting safe drinking water or similar schemes showed grim results due to their unavailability and time constraints to undertake additional work. Another major barrier was that most women were accustomed to the idea of a fixed monthly salary. Commission-based and target-driven work was outside their comfort zone. This can in part be attributed to the lack of confidence and risks involved in reaching out to communities and creating enough demand for water filters for the business to be profitable. They were unconvinced by arguments that this micro-entrepreneurship would provide long-term benefits. Thus, only two women eventually managed to take up the role of LEUs.
-
Responding to the above challenge, the team widened the pool of people suited as LEUs including teachers, doctors and NGOs in the area. In Madanpur Khadar, a local NGO ‘Sunshine’ and ‘Social Welfare Society’ and Pradhan from the local village-level committee were identified for encouraging activities in the area. However, owing to technological and area specific challenges, involvement of these stakeholders also could not bring appreciable results in the activity. In Ambedkar Colony, the rollout of the model has shown appreciable results in a short span of on-field activity. This was due to the involvement of Pradhan of the village, who provided on-field assistance. This support essentially helped in strengthening engagement with the community and building up their confidence for the on-going activity in the area. Moreover, lessons from experiences at Madanpur Khadar helped in formulating strategy and initiating work at Ambedkar Colony as the work here started in succession of Madanpur Khadar.
-
2.3.2 Piloting Microfinance-Inclusive LEU Model in Bundelkhand
Learning from the lessons in Delhi, a modified version of the LEU model with Self-Help Groups (SHGs) and local NGOs was piloted in few remote villages of Chattarpur, and Hamirpur districts of Bundelkhand region in Central India. The financial barrier was overcome by engagement with the local women SHGs, who supported the community through microfinance loans for purchasing the filter. The technological barriers were addressed through selection of the location with low-TDS levels.
During the study period, appreciable results in filter adoption rates were obtained in rural Bundelkhand with a 13% penetration in 3 months (among 3216 no. of households), as compared to Delhi with only 1.6% success. As most of these filters need filter media replacement periodically, the role of supply chains is quite critical in supplying replenishments and not just one-time sales. Hence, the model can become unsustainable if the supply chains function erratically. Therefore, the filter manufacturers are expected to build closer tie-ups with supply chains and provide oversight on distribution channels for sustaining and expanding their market outreach among vulnerable populations.
-
The Model
To overcome the challenges of recruiting individuals as LEUs, the presence of a strong local NGO was considered as a critical factor for the selection of a location during the pilot rollout in Bundelkhand. Sumitra Samajik Kalyan Sansthan (SSKS) was selected to enhance the outreach of services to the community. Also, the confidence of the community in the local NGO would serve as a driver for behaviour change (Mishra 2014). Based on our experience during the Delhi roll out, behaviour change in the community is an essential component for wider dissemination of safe water services especially as these services are often not prioritised by the BoP. SSKS was also involved in selecting and providing technical and institutional support to the SHG.
The model is centered on the involvement of Jai Shankar Swayam Sahayata Samooh, a local woman Self-Help Group (SHG) in the role of the LEU. It was strategized that one entity (the identified SHG) would undertake a long-term business initiative and be the driving force in the identified geographical domain. It will leverage the efforts of local entrepreneurs, who can promote the filters in their available time to generate some extra income whenever and wherever possible (Fig. 12.2).

Microfinanced LEU model schematic for Tata Swach
Tata Chemicals enabled the SHGs to procure the filters at a lower rate of Rs. 839, as the cost of the distributor was eliminated in this model. In one of the models, the filter was sold at the market price of Rs. 999 to the end customers, leaving the SHG with a profit of Rs. 160. An alternative model was implemented; wherein local shops were engaged with SHGs. Filters were also sold to these shopkeepers at a rate of Rs. 899. This resulted in an Rs. 60 profit to the SHG and an Rs. 100 profit to the local shopkeeper for each filter sold.
For widespread dissemination of safe water services among the community, in addition to upfront payment options, the model considers microfinancing options essential to overcome the financial barriers. Under microfinancing, the interested individuals from the target areas were provided with a loan to cover the initial instalment of Rs. 500 from the SHG for booking of the filter. This amount was either leveraged through SHG funds or Rashtriya Mahila Kosh fund, which was reaching the SHGs through the active intermediation of SSKS. The remaining amount of Rs. 499 was given by the customer at the time of procurement of filter. The amount of Rs. 500 leveraged by SHG to the customer was repaid to SHG within 1–3 months. The SHG charged interest at the rate of 18% for the loan. The model follows similar lines as the delivery model for Delhi roll out for replacement of filter bulb made by the local retailers and for activation and training services by Tata Chemicals. The project team facilitated the links between the various stakeholders.
-
On-the-Ground Activities
Demand creation is an essential component for wide-scale dissemination of services and long-term sustainability of the model. Prior to the rollout of Swach filter in the target locations, extensive efforts were put into creating demand for the product. Most of the times, the need for safe drinking water is not prioritised amongst the BoP population and, therefore, these needs remain unmet. There were regular awareness generation sessions conducted in Bundelkhand highlighting the importance of safe drinking water and how nano-based water filtration technology provides an affordable and effective solution to achieve the same. In addition, street plays were also organised at these locations. The team also used IEC material to facilitate information exchange with the community on importance and handling of safe drinking water. The community was also made aware of their drinking water quality by conducting on-field testing of water quality parameters including TDS using TDS meter and bacterial contamination using Aquacheck vials. The on-site testing of water quality had a massive impact on the communities. The approach for the field rollout was similar to the one adopted in Delhi.
-
The Challenge
Sustaining the supply chains remains a challenge. Tata Swach filters are not readily available in the nearby markets of Chhatarpur and Hamirpur. The nearest procurement of Swach for the on-going activity is made from the Ghaziabad region of Uttar Pradesh, which often consumes a lot of time in delivery of the filters. Time-consuming process of filter delivery to the target location is eventually leading to loss of interest in the community especially creating issues with the individuals who have paid for the services in advance. In order to speed up this process, and maintain the momentum created, DA has intervened and facilitated the process so that the local NGO is in close contact with manufacturer tracking the delivery of the orders. Efforts have also gone into making the manufacturer realise the potential of the market, which will also drive timely delivery of services to the growing client base in the study area.
3 Imperatives for Scaling up
The pilots lent themselves to a lot of learning on issues of access to water as well the support systems. The section below highlights some of the key lessons learnt from the experiences in Delhi and Bundelkhand.
-
Influencing behaviour change in the community for safe drinking water services: Based on our understanding of the attitude of BoP towards safe drinking water services, this section of society is aware of the health impacts associated with contaminated water, however, the need for such services often gets neglected over other priorities. Therefore, it becomes imperative to influence the behaviour to seek safe drinking water. For this on the spot water quality testing, street play/awareness generation campaign can play a very vital role in bringing out changes at grass-root level, in creating much-needed awareness and behaviour changes amongst the public at large. It was observed that the best method to change people’s mind set is on the spot water testing, wall paintings and street plays. In addition, sessions involving close interaction between the community and influential individuals from the medical field, water industry, etc., were helpful.
-
Engaging with local NGO/SHGs can better facilitate service delivery mechanisms: Based on our experience from the on-field activities, it can be clearly concluded that the peer-influenced models are not very successful for providing safe drinking water services, however, similar models for other products such as of Amway has shown appreciable results in urban space. The reason for the same is because safe drinking habits are not often prioritised and hence the demand is very limited, which is usually perceived as a risk by the entrepreneurs as it questions the profitability of the business. Therefore, these entrepreneurs are only interested to work in models from where they can derive fixed salaries on the monthly basis. Engaging with local NGOs and SHGs who have been present in the community from a long time in similar kind of activities would be beneficial in terms of their understanding on the needs of the community and the confidence community has on them.
-
On the financial front, the introduction of microfinancing with easy instalments-based schemes is a driver that accelerates uptake. Since the sale of filter is a consumer product, user preference and expectations from the product are keys to successful adoption. Building financial incentives along the supply chains is a key factor for sustaining and scaling up of the service delivery models.
-
Aesthetic aspects—to enhance product acceptability: In addition to the filter parameters such as affordability, effectiveness in treating water, the rate of filtration and ease of filtration, change of taste and aesthetics catering to aspirations also are found to be critical parameters in accepting a treatment solution or a filter product.
4 Way Forward
The study highlighted the hypothesis that access to water is impeded by the lack of appropriate delivery systems to the Bottom of the Pyramid. The pilots clearly demonstrated that there is a demand for safe water. However, to convert this demand into changed behaviour and practice, there is a need for customers to see clear value in the product. This value creation can be perceived both in terms of the service offered and a perceptible difference from the raw water baseline as well as the financial value of the product, in terms of ease of payment, avoided health costs, etc.
In order to be able to service the BoP, it is important to develop and strengthen the delivery mechanism. The pilot showed that penetration and conversion were much higher in spaces where there was trust at the point of delivery. Building capacities of all points of the chain are important to ensure smooth delivery of the product and service.
References
Report
Vijaya Lakshmi, K., Nagrath, K., & Jha, A. (2011). Access to safe water: Approaches for nanotechnology benefits to reach the bottom of the pyramid. New Delhi: Development Alternatives Group.
Vijaya Lakshmi, K., Nagrath, K., & Mishra, S. (2013). Access to safe water for the bottom of the pyramid.
Online Document
DA. (2011). Market potential analysis for water purifier using nanotechnology for the bottom of pyramid market.
TARA. (2012). Access to safe water for the bottom of pyramid: Strategies for disseminating technology research technology packaging study.
WHO. (2011). Estimated with data from Diarhhoea: Why children are still dying and what can be done. The UNICEF fund.
Newsletter Article
Kumar, S. (2013, October). Innovative service delivery model for providing low cost safe drinking water solutions to rural India.
Mishra. S. (2014, March). Providing low cost safe drinking water solutions to rural Bundelkhand.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2018 The Author(s)
About this paper

Cite this paper
Mishra, S., Vijaya Lakshmi, K. (2018). Reaching the Last Mile—Technology Solutions and Models for Service Delivery. In: Hostettler, S., Najih Besson, S., Bolay, JC. (eds) Technologies for Development. UNESCO 2016. Springer, Cham. https://doi.org/10.1007/978-3-319-91068-0_12
Download citation
DOI: https://doi.org/10.1007/978-3-319-91068-0_12
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-91067-3
Online ISBN: 978-3-319-91068-0
eBook Packages: Earth and Environmental ScienceEarth and Environmental Science (R0)