
Abstract
Even if heart transplantation is an undisputed source of medical progress, several complications still hamper the outcome of transplanted patients. Among them, infections are associated with significant morbidity, mortality, and economic burden.
Depending on clinical and radiological signs and based on the time interval after transplantation, a broad spectrum of microbial pathogens can be responsible for these infections. This microbiological diversity, associated with altered clinical signs due to immunosuppressive drugs, is a cause of delayed diagnosis and treatment.
The objective of this overview is to provide a structured procedure to explore fever and specific symptoms that can be suggestive of infection in heart-transplanted patients. Furthermore, main preventive and curative strategies will be described.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others



Keywords
1 Background
Heart transplantation has revolutionized the outcome of patients with terminal chronic heart failure. Worldwide, about 5,000 heart transplantations are performed annually (Stehlik et al. 2011). Survival after heart transplant is continuously increasing due to advances in drug-induced immunosuppression, improvement of surgical procedures, optimal pretransplant risk assessment, and close patient monitoring (Stehlik et al. 2011; Gavalda et al. 2014a).
Soon after the first heart transplantations were performed in the late 1960s, infection appeared to be a major complication and a significant cause of mortality. Indeed, infectious events are responsible for 30 % of deaths, with a significant weight between 30 days and 1 year posttransplant (Stehlik et al. 2011). Beyond morbidity and mortality, infectious complications are also associated with a high economic burden due to higher length of hospital stay, increased graft losses, and costs related to indirect effects such as virus-induced malignancies (Gavalda et al. 2014a; Menzin et al. 2011). Beyond this direct burden, microorganisms are also involved in indirect transplant-related complications. For instance, it has been repeatedly shown that the “microbially determined immune modulation (MDIM)” could increase the risk of allograft injury or rejection, atherogenesis, malignancies (such as PTLD), and other opportunistic pathogens (Gavalda et al. 2014a). Therefore, preventive measures are cornerstone for the management of heart-transplanted patients (Fishman 2014).
There are many challenges in the management of infectious diseases after heart transplantation. First, infectious processes may originate from a wide range of sources (hospital environment, recipient community, reactivation of a latent process, transmission by the donor organ) (Fishman 2014; Wright and Fishman 2014). Therefore, a high number of bacterial, viral, fungal, and parasitic agents may be causative in heart transplant recipients. Second, the use of immunosuppressive agents may modify the clinical presentations associated with infectious events (Fishman 2014). Finally, drug toxicities and interactions are frequent and hamper antimicrobial treatment once the infectious diagnosis is made in such patients (Fishman 2014).
For all these reasons, diagnosis, prevention, and treatment of infectious complications appear as a cornerstone aspect of the management of heart-transplanted patients.
2 Clinics and Management
After solid organ transplantation, infectious risk may be stratified according to two axes: time posttransplantation and source of the infection.
Follow-up after heart transplantation can be divided into three time periods: less than 4 weeks after SOT (phase 1), between 1 and 6 months (phase 2), and more than 6 months after SOT (phase 3) (Fig. 19.1) (Fishman 2014; Wright and Fishman 2014). Besides that transplantation timeline, four distinct infection sources should be distinguished: the hospital environment, community exposure, donor (or graft) derived, and reactivation of an infection from the recipient (Fishman 2014; Wright and Fishman 2014). Taken together, these elements lead to distinct microbiological hypothesis.

Infectious timeline after heart transplantation and most frequent sources of infections. To note, even if donor-derived or recipient-derived infections are always possible, different pathogens can be involved, depending on the delay after transplantation (Adapted from Fishman 2014). *Of note, after 6 months, donor-derived infections are rare, with the notable exception of CMV disease
-
In the early phase after heart transplantation, most of infections are related to surgery and/or postoperative supportive care. Among these infections should be included surgical site and wound infections and catheter-related or urinary tract infections. The frequent use of antibiotics before or after surgery increases the risk of C. difficile-associated diarrhea (Fishman 2014). Lastly, donor-derived infections can be revealed early after heart transplantation if donor had an active viral, bacterial, or fungal infection or in case of graft contamination (Fishman 2014; Wright and Fishman 2014).
-
Between 1 and 6 months, co-trimoxazole prophylaxis significantly reduces the risk of major opportunistic infections such as P. jirovecii pneumonia, T. gondii encephalitis, or listeriosis and may also reduce the risk of urinary tract infections. Most of febrile episodes are caused by viruses and graft rejection at that time (Fishman 2014). Depending on the level of immunosuppression, a broad spectrum of pathogens can occur such as Aspergillus spp., Cryptococcus spp., or Nocardia spp.
-
More than 6 months after transplantation, drug-induced immunosuppression is tapered for most of patients. Thus, opportunistic pathogens are less common (Fishman 2014). However, opportunistic infections might occur late after transplantation, especially if immunosuppression has been beforehand intensified due to allograft rejection (Fishman 2014). The risk of CMV late-onset infection should be considered if an antiviral prophylaxis has been used and stopped. Besides, transplanted patients can experience more severe complications from community-acquired infections.
Even if infection is usually suspected because of fever, the first diagnostic step is to perform a complete clinical examination in order to identify a focus of infection.
2.1 Lung Infections
In case of respiratory symptoms (e.g., cough, dyspnea, chest pain), lung infection should be suspected, and a radiological work-up is mandatory. Even if chest radiography is still an important first-line exam, computed tomodensitometry (CT) scan is now considered cornerstone in order to obtain a clearer view of the type and extension of the lung lesions (Gavalda et al. 2014b). Indeed, depending on the type of radiological aspect, oriented diagnostics should be suspected (Fig. 19.2). In case of radiological abnormalities, a microbiological work-up is mandatory in order to increase the likelihood of pathogen identification.

Microbial etiologies as a function of radiological findings during pneumonia, in heart transplant recipients
In case of pneumonia occurring early after transplantation (phase 1), a ventilator-associated pneumonia should be suspected. In that case, a distal sample is mandatory, due to the broad spectrum of possible pathogens and the high frequency of resistant bacteria. In that case, bronchoscopy is mandatory and allows performing bronchoalveolar lavage (BAL), distal protected specimen with a plugged telescoping catheter or a brush. If the patient is ventilated, bronchoscopy is not mandatory and a blinded protected telescoping catheter sampling is feasible.
If pneumonia occurs in phase 2 or 3, community-acquired or opportunistic pathogens are responsible for most cases of infections. In that case, chest CT scan is important as microbiological diagnosis can be suspected based on the radiological picture (Fig. 19.2).
In any case, noninvasive diagnostic procedures are cornerstone such as sputum analysis (for Gram staining, bacterial cultures, fungal and mycobacterial examinations), urine antigen assays (for S. pneumonia and L. pneumophila), and blood cultures.
However, due to the broad spectrum of responsible pathogens, an invasive procedure is frequently required and relies on the BAL. Usually, BAL is required in case of nodular or interstitial pneumonia or in case of lung consolidation without clinical improvement after a 3-day course of antibiotics. Lastly, bronchoscopy and BAL should be proposed in case of relapsing infection, despite a complete course of antibiotics. This procedure will allow obtaining specimen for bacterial, mycobacterial, and viral examinations (Tables 19.1 and 19.2). Fungal examination is also important and should include the identification of P. jirovecii with Grocott–Gomori methenamine silver (GMS) staining, immunofluorescence ± quantitative PCR-based assay. Furthermore, indirect tests can be proposed in the blood and in the BAL, depending on the radiological aspects such as galactomannan antigen (for the identification of Aspergillus spp.), Cryptococcus spp. antigen, or β-D-glucan.
In case of nodular pneumonia and if BAL is negative, a lung biopsy should be proposed for microbial identification but also to rule out a noninfectious diagnosis (PTLD, cancer). In that case, a complete microbiological work-up is also mandatory (Table 19.1).
2.2 Neurological Symptoms
Between 10 and 85 % of SOT recipients experience central nervous system (CNS) symptoms (Wright and Fishman 2014). Among them, infections are one of the most severe etiologies. However, due to the use of drug-induced immunosuppression, clinical signs and symptoms may be reduced. Of note, noninfectious causes such as metabolic disorders, drug-induced side effects, and primary brain lymphoma should be considered. Early CNS infections (during phase 1) are rare, unless the patient experiences a massive microbial exposure or exhibits an anatomic underlying factor (Wright and Fishman 2014). Furthermore, donor-derived infections may occur in this time period, such as lymphocytic choriomeningitis, West Nile virus or herpes simplex virus (HSV) encephalitis, or, in case of graft contamination, cryptococcosis, even if the latter case is rare. CNS opportunistic infections mainly occur during phases 2 and 3. Fungal infections (Aspergillus, C. neoformans, Histoplasma, Coccidioides), nocardiosis, toxoplasmosis (if the chosen prophylaxis is not active against T. gondii), and tuberculosis should be considered (Wright and Fishman 2014; Lebeaux et al. 2014a). Viral infections are also possible at that phase (such as HSV or VZV encephalitis). After 6 months, even if the patient may experience infection caused by community-acquired pathogens (S. pneumoniae), the risk of opportunistic pathogens can be increased as prophylaxis is usually interrupted at that stage: herpesviruses, nocardiosis, invasive molds, tuberculosis, and cryptococcosis can be encountered.
If CNS infection is suspected, two cornerstone elements are mandatory: lumbar puncture and brain imaging (CT scan or, ideally, magnetic resonance imaging, MRI). Indeed, MRI has been shown to be superior, especially in the case of invasive fungal infections (Gavalda et al. 2014b). Lumbar puncture should be performed first in case of meningeal syndrome. However, brain imaging should be performed before LP in case of localizing neurological signs, seizure, or reduced vigilance. Indeed, these clinical signs might be suggestive of intracranial hypertension. In that case, LP increases the risk of brain herniation (Duffy 1969). If lumbar puncture is performed, several microbiological tests should be performed (Table 19.1). If Cryptococcus infection is suspected or diagnosed, CSF opening pressure should be measured (see below). Based on the results of brain MRI and LP, different pathogens are possible (Fig. 19.3).

Microbial etiologies in case of neurological signs, based on the results of brain imaging and lumbar puncture. *At the initial stage of viral meningitis, PMN cells can prevail. CSF cerebrospinal fluid, CT computed tomography, EBV Epstein–Barr virus, HSV herpes simplex virus, LP lumbar puncture, MRI magnetic resonance imaging, PMN polymorphonuclear, PTLD posttransplant lymphoproliferative disorder, VZV varicella-zoster virus, WBC white blood cells
Furthermore, the presence of extra-neurological symptoms can be cornerstone for the microbial diagnosis. For instance, concomitant skin lesions can suggest disseminated nocardiosis and mycobacterial or fungal infections (Wright and Fishman 2014; Lebeaux et al. 2014a). In that case, a skin biopsy should be performed. In this regard, lung infection, heart murmur, and sinusitis should also be investigated.
Lifestyle is also important to assess neurological symptoms, and an extensive travel history should be made for these patients. For instance, a recent travel in tropical zone should prompt malaria testing. Even if the travel occurred years ago, the diagnosis of endemic fungus should be investigated (e.g., Coccidioides immitis, Histoplasma)
If LP and the abovementioned extensive extra-neurological work-up did not lead to a microbial diagnosis, neurosurgery should be considered for biopsy or debridement, in case of brain abscess (Wright and Fishman 2014).
2.3 Skin and Soft Tissue Infections
Most of skin and soft tissue infections occurring during phase 1 are related to the surgical procedure. In that case, the most worrisome diagnosis should be mediastinitis. Indeed, heart transplant recipients have an increased risk of surgical wound infections, as compared with patients undergoing conventional heart surgeries (Zuckermann and Barten 2011). After heart transplantation, surgical wound infections are observed in 8–15 % of patients with some groups reporting incidence of mediastinitis up to 40 % (Zuckermann and Barten 2011). The diagnosis of surgical wound infection may be difficult as fever, erythema, and purulent discharge are sometimes absent (Zuckermann and Barten 2011). Therefore, chest CT scan and needle aspiration are cornerstone for the diagnosis of posttransplant mediastinitis.
Due to prophylaxis with aciclovir or valaciclovir, viral recurrences caused by HSV or VZV are rare but can be severe with more extensive zona or herpes lesions. Without prophylaxis, reactivation of HSV or VZV can occur in more than 35 % of cases (Ulrich et al. 2008).
During phases 2 and 3, other cutaneous findings may be related to community-acquired infections caused by group A Streptococcus or S. aureus. Strikingly, Gram-negative rods can be responsible for skin and soft tissue infections in immunocompromised patients. Opportunistic pathogens can also be causative, especially in case of nodular skin lesions or relapse after an antibiotic course. In that case, main diagnosis includes bacteria (Nocardia spp.), mycobacteria, and fungus (Cryptococcus, invasive dermatophytosis, Aspergillus spp.) (Lebeaux et al. 2014a; Ulrich et al. 2008). Skin lesions may be secondary to direct skin inoculation (after telluric or soil trauma, for instance) or because of a disseminated disease (in which a hematogenous spread is observed). Therefore, skin lesions should always be considered after heart transplantation, and skin biopsy performed when possible.
During phase 3, human herpesvirus 8 (HHV8) can be responsible for Kaposi sarcoma, human papilloma viruses (HPV) can cause warts, and mucocutaneous candidiasis are frequent (Ulrich et al. 2008).
Lastly, heart-transplanted patients have an increased risk of skin cancer. Thus, a yearly dermatological examination is mandatory.
2.4 Digestive Tract Infections
During phase 1, most of the digestive tract infections are caused by C. difficile. This infection is related to nosocomial exposure and frequent antibiotic prescription. During the second and the third phases, community-acquired as well as opportunistic pathogens can be found. In case of diarrhea after heart transplantation, an exhaustive microbiological work-up is mandatory (Table 19.1). In this setting, viruses can be responsible for long-term aqueous diarrhea. Of note, if the patient has been exposed to Strongyloides, even decades ago, initiation of corticosteroids and/or immunosuppressive drugs can be responsible for hyperinfection syndrome (see below).
2.5 Isolated Fever
Lastly, infection can be suspected in heart-transplanted patients only because of an isolated fever. If none of the abovementioned symptoms are present, a minimal work-up is mandatory and should include at least blood and urine cultures and chest radiography. If uninformative, chest and abdominal CT scan, cryptococcal antigen, serum PCR for CMV, and toxoplasmosis should be performed. Cardiac echocardiography can also be performed to investigate infective endocarditis. Lastly, noninfectious etiologies must be considered such as PTLD.
3 Viral Diseases
3.1 Cytomegalovirus
Cytomegalovirus (CMV) is the major viral agent after heart transplantation, increasing both morbidity and mortality. CMV may cause direct effects (ranging from benign viral syndrome to life-threatening tissue-invasive disease) as well as indirect effects such as allograft rejection, coronary vasculopathy, accelerated atherosclerosis, new-onset diabetes mellitus after transplantation, and opportunistic infections. International consensus guidelines on the management of CMV after solid organ transplantation have recently been published (Kotton et al. 2013).
“CMV infection” usually applies to the evidence of CMV replication without any signs of disease. When attributable symptoms are associated with this viral replication, the process is called “CMV disease.” CMV disease is divided into “viral syndrome” (fever, malaise, hematological cytopenia) and “tissue-invasive disease,” a process that may, for example, affect the digestive tract, the eyes, the central nervous system, the pancreas, or the liver and the lungs. Therefore, complete physical examination and adapted work-up should be conducted when a CMV infection is suspected.
Risk stratification is of great importance to prevent CMV after transplantation. A CMV IgG screening test should be performed for both donor (D) and recipient (R) before transplantation to allow for risk stratification of CMV disease. Beyond serostatus, some specific cell-mediated immunity tests such as QuantiFERON-CMV and ELISpot have been developed to better predict the risk of CMV disease (Manuel et al. 2013a). Due to the strong impact of CMV infection on clinical outcomes, a preventive strategy should be used for both CMV-positive recipients (R+) and CMV-negative recipients with a positive donor (D+/R-). Two preventive strategies are currently available: universal prophylaxis (i.e., administration of antiviral therapy in the first months after transplantation) and preemptive therapy (i.e., repeated realizations of laboratory assays such as (ideally) quantitative nucleic acid amplification testing or pp65 antigenemia ± administration of antiviral therapy once an early viral replication has been diagnosed). Their roles are summarized in Table 19.3. If universal prophylaxis is selected, routine viral load monitoring should not be encouraged in asymptomatic patients as this strategy is not cost-benefit. For CMV prophylaxis, oral valganciclovir (900 mg once daily) and intravenous ganciclovir (5 mg/kg once daily) have proven their efficacy. Both valganciclovir and ganciclovir dosages should be adjusted to renal function. Limited data suggest that the preventive use of CMV hyperimmune globulin may decrease the cardiac consequences of CMV infection after heart transplantation (Valantine et al. 2001).
While serological tools have no role after transplantation, both CMV pp65 antigenemia and PCR assays are highly useful tools for the diagnosis of CMV infection. Of note, sensitivity of pp65 antigenemia decreases significantly in neutropenic recipients, defined as less than 1000 polymorphonuclear cells/mm3. Mainly because of poor interhospital correlation of PCR assays until the recent creation of an international World Health Organization (WHO) standard, no consensual cutoff value has been determined to initiate antiviral therapy in patients with isolated replication without identified disease. While a low threshold should most likely be used in D+/R- couples to initiate antiviral therapy and prevent direct and indirect effects of CMV infection, it is unclear when to initiate therapy in CMV seropositive heart transplant recipients. Kinetics of DNAemia may offer additional information. The role of CMV detection by PCR in bronchoalveolar lavage is still a matter of debate. Last, physicians should be aware of the possibility of a compartimentalized CMV disease. A common illustration is that of digestive CMV disease which may be seen with undetectable or low viral load values in blood samples.
Curative treatment of CMV infection in heart transplant recipients does not differ from other solid organ transplant recipients. Briefly, oral valganciclovir as well as intravenous ganciclovir could be used for nonlife-threatening CMV disease, with the notable exception of gastrointestinal tract infections. In that case, oral valganciclovir should be avoided. Treatment dose should be adapted with great attention according to the estimated glomerular filtration rate. Duration of treatment is based on the monitoring of CMV DNAemia. A minimum length of treatment of 2 weeks should be used, at the condition of obtaining one or more negative CMV tests (i.e., pp65 antigenemia or PCR). Antiviral drug resistance is a cause of persisting infection despite antiviral treatment at an adapted dose. Testing for mutations of viral UL97 kinase and/or UL54 DNA polymerase should be conducted in such cases.
3.2 Herpes Simplex and Varicella-Zoster Viruses
Like CMV, other Herpesviridae viruses are able to cause infection in transplant recipients. Among them, herpes simplex virus (HSV) and varicella-zoster virus (VZV) are of importance. Due to the impaired cell-mediated immunity observed after transplantation, both these agents may progress from latency in sensory nerve ganglia to reactivation. HSV and VZV may also be transmitted via the graft from an infected donor.
HSV type 1 (HSV-1) and type 2 (HSV-2) are generally transmitted by direct contact with a subject actively infected. While primary HSV-1 infection usually occurs during childhood via oral secretions, HSV-2 is sexually transmitted. In the absence of antiviral prophylaxis, HSV replicates in the first weeks after transplantation and symptoms ranging from mucocutaneous viral reactivation to lethal multiple visceral organ involvement may be observed. Atypical presentations require adapted specimen collection and laboratory confirmation. In case of benign mucocutaneous lesions due to HSV, aciclovir (400 mg PO three times daily) and valaciclovir (1 g PO twice daily) are effective agents when started early after the onset of symptoms. In case of severe disease such as meningoencephalitis or disseminated disease, aciclovir should be used intravenously at a dose of 10 mg/kg every 8 h.
More than 90 % of adults are infected by VZV. Serological testing should be conducted before transplantation to identify VZV-naïve patients as the occurrence of primary infection after transplantation may lead to severe dermatologic lesions and visceral involvement (e.g., pneumonitis) in such subjects. In seropositive transplant patients, herpes zoster (also known as shingles or zona) may present as dermatomal herpes zoster or as varicella-like skin lesions. In most cases, a clinical diagnosis can be made. Contact with infected subjects may be a clue to diagnosis. Unlike CMV, asymptomatic replication is not observed after solid organ transplantation. As a consequence, identification of VZV (e.g., by PCR) from lesions or plasma is a highly valuable tool. Aggressive therapy is needed once the diagnosis of VZV disease has been made in an immunocompromised patient. Intravenous aciclovir should be used at a dose of 10 mg/kg every 8 h. Dosing adjustments with renal impairment is required. Localized shingles may be treated orally with valaciclovir (1 g three times daily). Of note, aciclovir-resistant VZV isolates have been described.
Preventive strategies play a significant role for both HSV and VZV. Prophylaxis against HSV should be used for 1–3 months after solid organ transplantation. Aciclovir (400–800 mg per os twice daily) and valaciclovir (500 mg per os twice daily) are effective to prevent HSV infections in transplant recipients. Of note, ganciclovir and valganciclovir (the most widely used anti-CMV drugs) also offer protection against HSV and VZV. Patients who are seronegative pretransplant for VZV should receive vaccination before transplantation. Indeed, the use of this live virus vaccine is not recommended after transplantation.
3.3 Epstein–Barr Virus
More than 90 % of the world population is infected with Epstein–Barr virus (EBV). Such as other Herpesviridae viruses described supra, it persists lifelong. After transplantation, the use of immunosuppressive agents imbalance the relation established between EBV-infected B-cells and the host’s cytotoxic T lymphocyte response. As a consequence, it may lead to a wide range of presentations ranging from asymptomatic viremia to posttransplantation lymphoproliferative disorder (PTLD). EBV serological testing should be realized for risk stratification before transplant for both donor and recipient. EBV-negative recipients of EBV-positive heart transplants (D+/R-) have the highest risk of PTLD. In this high-risk population, EBV-positive PTLD typically occurs within 1 year after transplantation. Because increased EBV viral load is linked to aberrant EBV-induced B-cell proliferation, the question of viral load monitoring is of interest. However, such strategies of monitoring are imperfectly correlated with the risk of developing EBV-positive PTLD, especially due to a low-positive predictive value. Moreover, this tool has no utility for predicting EBV-negative PTLD. In patients who are at high risk for PTLD (such as EBV D+/R− patients and/or recipients with chronic EBV viremia), preemptive reduction in immune suppression appears to be an effective first-line strategy. The role of adjunctive therapies such as rituximab is an ongoing debate in solid organ transplant recipients. Apart from PTLD, uncommon events such as infections of the central nervous system and aplastic anemia have been associated with EBV in transplant recipients.
3.4 Influenza and Other Community-Acquired Respiratory Viruses
In immunocompromised subjects such as heart transplant recipients, community-acquired respiratory viruses (CARVs) have been shown to be responsible for severe respiratory diseases (Table 19.2) (Manuel et al. 2013b). Progression from upper to lower respiratory infection is common. Clinical symptoms are poor tools to distinguish one CARV from one other. Infections with CARVs should be suspected in all solid organ transplant recipients with symptoms of upper or lower respiratory tract infection. Specimens should be taken as soon as possible from the site of clinical involvement. In case of upper respiratory tract symptoms, pooled nasopharyngeal and throat swabs are recommended. In case of lower respiratory tract infection, BAL should be made when possible, in order to exclude other infectious diseases. Laboratory diagnostic methods mainly include antigen detection assays, virus isolation by cell culture, and nucleic acid amplification testing. When available, the latter is a rapid and highly sensitive tool for clinicians. Prevention is a major tool to prevent infection by CARVs in solid organ transplant recipients. Inactivated vaccination is highly recommended to prevent influenza in solid organ transplant recipients, even if conflicting results have been published concerning its immunogenicity in heart transplant recipients. Meanwhile, vaccination of household contacts and health-care workers attending transplanted patients should be done annually. To prevent infections with CARVs in transplant recipients, general preventive measures are also mandatory (including contact avoidance with individuals suffering from respiratory tract infection and young children, hand hygiene, and adapted isolation of infected patients). Promising results have been published concerning the use of prophylaxis by neuraminidase inhibitors in solid organ transplant recipients during influenza season (Ison et al. 2012). Curative treatment options are presented in Table 19.2. Antiviral therapy using neuraminidase inhibitors should be administered in all heart transplant recipients with suspected influenza infection, even if symptoms started several days earlier. In severe cases, reduction of immune suppression should be considered.
3.5 West Nile Virus
West Nile virus (WNV) is an arthropod-born agent. WNV is mainly acquired via Culex that are infected by wild birds. While this disease has been first described in the West Nile district of Uganda in 1937, many countries are currently concerned all over the world. Notably, a worrisome outbreak is observed in North America since 1999. Transmission has also occurred through blood transfusion and transplantation with an infected organ. While 80 % of WNV infections are asymptomatic in immunocompetent subjects, symptomatic forms range from West Nile fever (a self-limiting febrile illness) to neuroinvasive diseases (meningitis, encephalitis, or acute flaccid paralysis) and myocarditis. Solid organ transplant recipients are at higher risk for severe disease (Singh et al. 2013). Incubation varies from 3 to 14 days. The diagnosis of WNV depends on a high index of suspicion. Serum and cerebrospinal fluid analysis should include WNV serological assays and nucleic acid testing. WNV treatment is mainly supportive and may include reduction of immunosuppression, use of interferon or passive immunization using anti-WNV antibodies. In the absence of an available vaccine, protection against mosquito bites should be recommended in the concerned areas.
4 Nonviral Diseases
4.1 Management of Fungal and Parasitic Infections
Candidiasis
Candida is the most frequent agent of invasive fungal infection (IFI) after SOT, accounting for more than half of the cases (Gavalda et al. 2014b). Most cases occur during phase 1 and originate from the gut and an indwelling device (such as intravenous catheter) or can be caused by a graft contamination (even if this latter event is more frequently associated with kidney transplantation). Invasive candidiasis is associated with a high mortality (≈30–40 %) (Gavalda et al. 2014b). Even if blood cultures are cornerstone, it has been repeatedly shown that their sensitivity for invasive candidiasis was 50–75 %, therefore leading scientific societies to propose other diagnostic options such as the detection of β-D-glucan in the serum that can be useful for its negative predictive value (Gavalda et al. 2014b). Initial treatment of candidemia should rely on intravenous echinocandins. All central venous catheters should be removed, except in specific and complex situations, and venous ultrasonography, cardiac echocardiography, and funduscopy should be performed. Antifungal treatment should be prescribed for 14 days after the first negative blood culture (Gavalda et al. 2014b). Asymptomatic candiduria, a common phenomenon, should not be treated unless the patient is neutropenic or is about to have a urological procedure. However, symptomatic candiduric patients must be treated, and urinary catheters should be removed or replaced.
Aspergillosis
Aspergillus is the second most frequent fungal pathogen after SOT, and heart- and lung-transplanted patients are at higher risk. Most of cases are invasive aspergillosis (IA) with an acute pulmonary (Fig. 19.4) or neurological infection that is associated with a high mortality (up to 80 %) (Gavalda et al. 2014b). IA can be considered proven if specific diagnostic criteria are met (Table 19.4) (De Pauw et al. 2008). In other cases, IA is considered probable or possible (Table 19.5). To note, even if the detection of galactomannan antigen in the serum is not recommended in SOT recipients due to its low sensitivity, it can be performed in BAL or CSF (Gavalda et al. 2014b). β-D-Glucan can be used for the diagnosis of IA even if false-positive or false-negative results have been reported.

Invasive aspergillosis after transplantation. Axial non-enhanced computed tomography (NECT) of a transplanted patient with invasive aspergillosis shows a right hilar mass (a, black arrow) with central low attenuation and intrinsic air (b), consistent with tissue necrosis and early cavitation
No universal antifungal prophylaxis is proposed, but some groups propose an itraconazole-based prevention only to patients at high risk of IFI (acute rejection, hemodialysis, reexploration after transplantation, CMV disease, or excessive Aspergillus spp. in the air of the center) (Gavalda et al. 2014b).
Antifungal therapy should be initiated early in case of suspicion of IA, and immunosuppression should be reduced. First-line treatment should rely on voriconazole, and therapeutic drug monitoring is mandatory with a trough concentration target between 2 and 4 mg/l. Drug-to-drug interactions and liver and skin toxicities (including squamous cell carcinoma, in case of long-term therapy) should be closely monitored. Treatment duration is difficult to standardize but usually lasts for 6–12 weeks. Surgery should be proposed in case of hemoptysis, endocarditis, sinus disease, pericardium, or large vessels involvement (Gavalda et al. 2014b).
Cryptococcosis
The third most frequent fungal pathogen is Cryptococcus, especially in patients receiving high doses of corticosteroids, monoclonal antibodies, alemtuzumab, or infliximab. Most of cases occur lately after transplantation (16–21 months), and mortality may reach 25 % (Gavalda et al. 2014b). Cryptococcosis can be revealed by CNS or lung infection (Fig. 19.5), associated or not with fungemia and skin lesions. Besides blood, urine, and skin culture (in case of skin lesions), diagnostic relies on the detection of cryptococcal antigen in CSF and blood (Gavalda et al. 2014b). For meningoencephalitis, disseminated disease, and severe pneumonia, first-line treatment is liposomal amphotericin B (3–4 mg/kg/day) or amphotericin B lipid complex + flucytosine (25 mg/kg x4/j) for 2 weeks (induction therapy) (Gavalda et al. 2014b). Then if CSF culture is sterile, consolidation with fluconazole 400–800 mg/j for 8 weeks. Lastly, maintenance therapy with fluconazole 200 mg/j is prescribed for 6–12 months. In case of elevated intracranial pressure, large volume taps are required to reduce the intracranial pressure < 20 cmHg. Even if a reduction of immunosuppressant drugs should be proposed, immune reconstitution inflammatory syndrome (IRIS) can occur in 5–11 % of cases (Gavalda et al. 2014b). For focal pulmonary infections, fluconazole can be used first at 400 mg/day (6 mg/kg/day) for 6–12 months.

Coronal non-enhanced computed tomography of a transplanted patient with pulmonary cryptococcosis demonstrates a subpleural left upper lobe solid nodule (black arrow)
Pneumocystosis
Pneumocystis pneumonia (PcP) is a fungal infection responsible for an asymptomatic or mild disease in the normal host but severe interstitial lung infection (PcP) in immunocompromised patients. Despite intense controversies, it is now considered that infection originates from recent acquisition of Pneumocystis jirovecii rather than reactivation of a latent infection. After transplantation, the risk of PcP is high, especially in the first year posttransplant. As the use of prophylaxis with trimethoprim–sulfamethoxazole significantly decreases this risk, most of cases occur after cessation of this preventive agent (Wang et al. 2012). Thus, several groups propose a lifelong prophylaxis. Atovaquone or pentamidine can also be proposed as prophylaxis. The diagnosis of PcP can be difficult as PCR-based assays are highly sensitive and can reveal only colonization. β-D-Glucan has been demonstrated to have a high negative predictive value in this setting.
Toxoplasmosis
This life-threatening opportunistic infection is caused by T. gondii, a parasite able to encyst in several organs, such as the heart. In transplant recipients, toxoplasmosis can result from the transmission of the parasite with the graft (D+) to a seronegative recipient (R-) or from a reactivation of a pretransplant latent infection in a seropositive recipient (R+) (Derouin et al. 2008). In the first case, clinical signs usually occur in the first 3 months after heart transplantation (sometimes earlier, within 2 weeks) with febrile myocarditis, encephalitis, or pneumonia. Without prophylaxis, incidence of disseminated toxoplasmosis in case of mismatch (D+/R-) may reach 75 %, but trimethoprim–sulfamethoxazole prophylaxis efficiently prevents this complication. The second option (reactivation of a latent infection R+ patient) is less frequent. Even if serological reactivation (defined by a rise in IgG antibody titers, with a high avidity index) occurs in ≈5 % of R+ patients, a clinical toxoplasmosis is exceptional (Derouin et al. 2008). The diagnosis of disseminated toxoplasmosis relies on the identification of the parasite or its DNA (through PCR testing) in any involved organ or in the blood. Serologic diagnostic might be useful but does not have enough sensitivity or specificity. Even if trimethoprim–sulfamethoxazole is highly effective in preventing toxoplasmosis, the risk might appear after cessation of the drug or if it is replaced by aerosolized pentamidine prophylaxis against PcP. Beside trimethoprim–sulfamethoxazole, pyrimethamine alone or atovaquone can also be used as prophylaxis.
Strongyloidiasis
Strongyloides stercoralis is a parasite that is present in tropical and subtropical regions. Strongyloides can complete an entire life cycle through an autoinfection pattern, allowing a prolonged survival within the host, up to several decades (Roxby et al. 2009). The immunodepression induced after transplantation may lead to hyperinfection, through a massive increase in the reproductive cycle of the larvae (Roxby et al. 2009). After a proliferation step in the duodenum, larvae may reach the bloodstream, the lungs, and then the gut. Thus, hyperinfection syndrome usually associates respiratory symptoms leading to acute respiratory distress syndrome, gastrointestinal symptoms (from abdominal pain to gastrointestinal bleedings or occlusion), and neurological involvement. A frequent complication is the occurrence of a bloodstream coinfection or meningitis cause by Gram-negative enteric bacteria. Due to its severity, hyperinfection syndrome should be prevented in patients awaiting heart transplantation who lived or stayed in area of endemicity (South America, Africa, Southeast Asia), even decades ago. The prevention relies on the treatment of chronic intestinal strongyloidosis with ivermectin before starting chemical immunosuppression (Roxby et al. 2009).
Chagas disease
This vector-borne (reduviid bug) parasitic infection caused by Trypanosoma cruzi is widespread in Latin America where seven to eight million people are chronically infected (Andrade et al. 2014). Human disease can be separated in two different phases: acute and chronic infection (Lattes and Lasala 2014). In most of adult cases, acute infection is spontaneously cleared and frequently asymptomatic. However, without any specific treatment, infection can evolve to the chronic phase. This chronic infection can be asymptomatic but can lead in 30 % of patients to irreversible damages of the following organs: the heart, esophagus, colon, and peripheral nervous system. During acute infection, diagnosis can be made through direct parasitologic examination of the whole blood (with and without concentration) or serologic tests. The later methods only can be used for the diagnosis of the chronic phase. More recently, PCR-based methods performed on the blood, body fluid, or tissues emerged as sensitive tools for the diagnosis of chronic Chagas disease with low parasite burden or in case of reactivation.
Two connections between Chagas disease and transplantation are described: reactivation and graft-transmitted disease.
In the first case, chronic Chagas was not known before transplantation. For instance, the patient can suffer from end-stage heart dysfunction requiring transplantation because of chronic Chagas disease. After heart transplantation, immunosuppressant drugs are responsible for parasitic reactivation with parasitemia, meningoencephalitis, panniculitis, or erythema nodosum-like lesions and myocarditis. In case of heart transplantation, mortality may reach 100 %.
In the other scenario, the organ donor was suffering from an unknown chronic Chagas disease. Kidney and liver transplantation are associated with a risk of graft-transmitted disease of 19 and 29 %, respectively, but heart transplantation is contraindicated if the donor had a chronic Chagas disease (Andrade et al. 2014).
Because of these two scenarios, serologic screening for chronic Chagas disease is mandatory for donors and recipients originating from or who lived in endemic areas. In this regard, increased traveling and migrations are leading to difficulties regarding organ transplantation and blood donation systems.
4.2 Management of Mycobacterial Infections
-
Active tuberculosis (TB) is a severe disease after SOT with mortality ranging between 9.5 and 17 % (Meije et al. 2014). Most cases occur within the first year after transplantation. Strikingly, extrapulmonary or disseminated TB is more frequent than in the general population. As a consequence, all transplant candidates and living donors should ideally be screened for latent tuberculosis with a tuberculin skin test (lecture at 48–72 h, positive if induration ≥5 mm). However, due to a reduced sensitivity and false positiveness of tuberculin skin test after vaccination, interferon gamma release assay (IGRA) should be done when possible, independently of the tuberculin skin test result (Meije et al. 2014). In case of positive tuberculin skin test or IGRA test, active TB should be investigated.
Active TB can be confirmed only by culturing M. tuberculosis or detecting nucleic acid sequence from a clinical specimen. In case of lung infection, if sputum is negative, BAL, transbronchial biopsy, or mediastinoscopy should be considered. For extrapulmonary TB, any involved site might be sampled (Table 19.1).
If active TB is not present, treatment of latent TB is recommended for patients awaiting heart transplantation in any of the following cases: (i) positive TST or IGRA test, (ii) history of untreated TB, or (iii) history of contact with a subject with active TB. In that case, treatment relies on isoniazid (300 mg/day) + vitamin B6 for 9 months, associated with a close monitoring of liver tests and signs of neuropathy (Meije et al. 2014).
For the treatment of active TB, rifamycins (rifampicin or rifabutin) can be avoided in case of localized and non-severe infections. In that case, maintenance therapy should last for 12–18 months. However, for severe or disseminated TB, a regimen containing rifampicin or rifabutin is mandatory, with a close monitoring of calcineurin or mTOR inhibitors and corticosteroid levels (Meije et al. 2014). In that case, maintenance therapy should last for 9 months. IRIS during the treatment of active TB is possible.
-
Nontuberculous mycobacteria are ubiquitous and found in a wide range of environments. Even if their incidence is low, it is much higher after SOT than in the general population and may reach 0.24–2.8 % after heart transplantation (Meije et al. 2014). Most cases develop cutaneous lesions of the extremities, tenosynovitis, or arthritis (Meije et al. 2014). The diagnosis is confirmed by the isolation of NTM from a normally sterile body site. Even if lung infection is rare (beside lung recipients), its diagnosis is more complex and requires compatible clinical and radiological presentation (Fig. 19.6), exclusion of other diagnosis, and identification of NTM in BAL or two consecutive sputa or pulmonary tissue. Treatment of NTM requires antimicrobial therapy, surgical excision, or drainage and reduction of immunosuppressant drugs. Association of two or three drugs will be chosen, based on the initial severity and the identification of the bacterial species (Meije et al. 2014).
Fig. 19.6 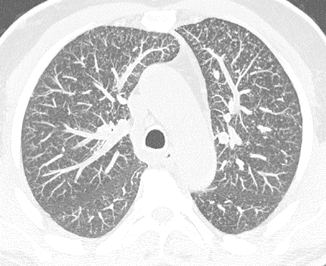
Transplanted patient with pulmonary Mycobacterium bovis infection. Axial non-enhanced computed tomography (Maximal intensity projection images) shows multiple scattered centrilobular nodules

4.3 Management of Opportunistic Bacterial Infections
Nocardia. Nocardiosis is a rare opportunistic infection caused by Nocardia spp., an ubiquitous aerobic actinomycete that is commonly found in a wide range of environments such as decaying vegetation, soil, and water. In recent reports, incidence after heart transplantation ranges between 0.65 and 2.5 % (Lebeaux et al. 2014a). Nocardiosis during the first month after SOT is uncommon and about 2/3 of cases occur during the first year after transplantation. Main risk factors are high-dose corticosteroids, cytomegalovirus (CMV) disease in the preceding 6 months, and a high median calcineurin inhibitor serum level in the preceding 30 days. Invasive nocardiosis accounts for 80–90 % of cases and is caused by bacterial inhalation, therefore leading to pneumonia in most cases. CT scan discloses lung infiltrates with consolidation (Fig. 19.7), nodules, excavations, or pleural effusion. Bacteria may then reach the bloodstream and disseminate to all organs: the CNS (with brain abscess), skin, soft tissue, eyes, liver, bone, heart valve, joint, muscle, and testis (Fig. 19.7). Overall mortality is ≈30 % but may reach 50 % in case of brain abscess. Strikingly, coinfections are possible with viral, bacterial, or fungal pathogens and are associated with a worst outcome. Primary cutaneous or subcutaneous nocardiosis is also possible in case of direct bacterial inoculation after a penetrating skin trauma. First-line treatment relies on trimethoprim–sulfamethoxazole, amikacin, third-generation cephalosporin, imipenem, or linezolid, depending on initial severity and dissemination (Lebeaux et al. 2014a). To reduce the risk of relapse, treatment is usually administered for 6 months in case of lung infection or 12 months in case of brain abscess.

Disseminated nocardiosis in a transplanted patient. (a) Nodular skin lesion of the right leg, (b) lung consolidation (coronal non-enhanced computed tomography, black arrow), (c) postcontrast sagittal T1-weighted magnetic resonance image showing multiple rim-enhancing brain lesions with a central hypointensity and peripheral edema, (d) Gram staining of the skin biopsy reveals filamentous and branching Gram-positive rods. Figure previously published in (Lebeaux et al. 2014b)
Listeriosis
Listeria monocytogenes is a Gram-positive bacillus that is transmitted to humans through contaminated foods such as milk and cheese or undercooked meat. It is responsible for bloodstream infection and meningoencephalitis in immunocompromised patients, including SOT recipients.
Conclusion
Even if heart transplantation dramatically changed the care of patients with terminal chronic heart disease, several challenges remain. Among them infections put the emphasis on the importance of mixing several medical skills including surgeon, infectious diseases specialist, radiologist, and microbiologist, among many.
Furthermore, there is still a lot to do regarding the challenges of donor-derived infection, in the context of a severe lack of grafts.
Key Points
-
Infection, a major complication which increases mortality after heart transplantation, should be suspected early in this population.
-
Due to the important number of causative pathogens, advances in molecular diagnostic tools, new therapeutic options, and interactions between antimicrobial agents and immunosuppressive drugs, a close collaboration between infectious diseases specialists and heart transplantation teams is mandatory.
-
Pretransplant evaluation of the heart transplant candidate should assess the risk of posttransplant infections with agents such as Herpesviridae, tuberculosis, and Strongyloides. Needed vaccinations should also be initiated during pretransplant care.
-
Preventive strategies (prophylaxis and preemptive therapy) increase the survival of heart transplant recipients. Main agents to consider are Herpesviridae (such as CMV, HSV, and VZV), influenzae, hepatitis viruses, Pneumocystis jirovecii, Toxoplasma gondii, and Mycobacterium tuberculosis.
-
Depending on factors such as donor specificities, pretransplant colonizations, drug-induced immunosuppression used, time post heart transplantation, local specificities, prophylactic regimen used, and clinical presentation, likely pathogens should be considered and guide first-line diagnostic investigations once an infection is suspected.
-
A wide range of viral, bacterial, fungal, and parasitic agents may cause infection after heart transplantation. An extensive clinical and radiological work-up is mandatory due to diagnostic pitfalls in these patients.
-
Early infections (within 4 weeks) after heart transplantation suggest surgical site and wound infections or graft-transmitted disease.
-
Clinical and radiological aspects have low predictive values to predict the causative microbial pathogen involved. Bronchoalveolar lavage and biopsy of any involved organ play an important role due to the broad spectrum of causative pathogens.
-
Antimicrobial resistance is a matter of concern in heart transplant recipients. Useless antimicrobial therapies should be avoided, and catheters and other devices should be removed when no longer essential. Antimicrobial therapies should be targeted against identified pathogen(s).
References
Andrade DV, Gollob KJ, Dutra WO. Acute chagas disease: new global challenges for an old neglected disease. PLoS Neglect Tropical Dis. 2014;8, e3010.
De Pauw B, Walsh TJ, Donnelly JP, Stevens DA, Edwards JE, Calandra T, Pappas PG, Maertens J, Lortholary O, Kauffman CA, Denning DW, Patterson TF, Maschmeyer G, Bille J, Dismukes WE, Herbrecht R, Hope WW, Kibbler CC, Kullberg BJ, Marr KA, Munoz P, Odds FC, Perfect JR, Restrepo A, Ruhnke M, Segal BH, Sobel JD, Sorrell TC, Viscoli C, Wingard JR, Zaoutis T, Bennett JE,; European Organization for R; Treatment of Cancer/Invasive Fungal Infections Cooperative G; National Institute of A; Infectious Diseases Mycoses Study Group Consensus G. Revised definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clin Infect Dis. 2008;46:1813–21.
Derouin F, Pelloux H, Parasitology ESGoC. Prevention of toxoplasmosis in transplant patients. Clin Microbiol Infect. 2008;14:1089–101.
Duffy GP. Lumbar puncture in the presence of raised intracranial pressure. Br Med J. 1969;1:407–9.
Fishman JA. From the classic concepts to modern practice. Clin Microbiol Infect 2014;20(Suppl 7):4–9.
Gavalda J, Aguado JM, Manuel O, Grossi P, Hirsch HH, Hosts ESGoIiC. A special issue on infections in solid organ transplant recipients. Clin Microbiol Infect. 2014;20(Suppl 7):1-3.
Gavalda J, Meije Y, Fortun J, Roilides E, Saliba F, Lortholary O, Munoz P, Grossi P, Cuenca-Estrella M, Hosts ESGfIiC. Invasive fungal infections in solid organ transplant recipients. Clin Microbiol Infect. 2014;20(Suppl 7):27–48.
Ison MG, Szakaly P, Shapira MY, Krivan G, Nist A, Dutkowski R. Efficacy and safety of oral oseltamivir for influenza prophylaxis in transplant recipients. Antivir Ther. 2012;17:955–64.
Kotton CN, Kumar D, Caliendo AM, Asberg A, Chou S, Danziger-Isakov L, Humar A, Transplantation Society International CMVCG. Updated international consensus guidelines on the management of cytomegalovirus in solid-organ transplantation. Transplantation. 2013; 96:333–60.
Lattes R, Lasala MB. Chagas disease in the immunosuppressed patient. Clin Microbiol Infect. 2014;20:300–9.
Lebeaux D, Morelon E, Suarez F, Lanternier F, Scemla A, Frange P, Mainardi JL, Lecuit M, Lortholary O. Nocardiosis in transplant recipients. Eur J Clin Microbiol Infect Dis. 2014a;33:689–702.
Lebeaux D, Rodriguez-Nava V, Laurent F, Mainardi JL, Meynard JL, Toro A, Boiron P, Lecuit M, Lortholary O. Diagnosis and treatment of nocardiosis. Lettre de l’Infectiologue. 2014. XXIX:20–5.
Manuel O, Husain S, Kumar D, Zayas C, Mawhorter S, Levi ME, Kalpoe J, Lisboa L, Ely L, Kaul DR, Schwartz BS, Morris MI, Ison MG, Yen-Lieberman B, Sebastian A, Assi M, Humar A. Assessment of cytomegalovirus-specific cell-mediated immunity for the prediction of cytomegalovirus disease in high-risk solid-organ transplant recipients: a multicenter cohort study. Clin Infect Dis. 2013;56:817–24.
Manuel O, Estabrook M, Practice ASTIDCo. RNA respiratory viruses in solid organ transplantation. Am J Transplant. 2013;13(Suppl 4):212–9.
Meije Y, Piersimoni C, Torre-Cisneros J, Dilektasli AG, Aguado JM, Hosts ESGoIiC. Mycobacterial infections in solid organ transplant recipients. Clin Microbiol Infect. 2014;20(Suppl 7):89–101.
Menzin J, Meyers JL, Friedman M, Korn JR, Perfect JR, Langston AA, Danna RP, Papadopoulos G. The economic costs to United States hospitals of invasive fungal infections in transplant patients. Am J Infect Control. 2011;39:e15–20.
Roxby AC, Gottlieb GS, Limaye AP. Strongyloidiasis in transplant patients. Clin Infect Dis. 2009;49:1411–23.
Singh N, Levi ME, Practice ASTIDCo. Arenavirus and West Nile virus in solid organ transplantation. Am J Transplant. 2013;13(Suppl 4):361–71.
Stehlik J, Edwards LB, Kucheryavaya AY, Benden C, Christie JD, Dobbels F, Kirk R, Rahmel AO, Hertz MI. The Registry of the International Society for Heart and Lung Transplantation: Twenty-eighth Adult Heart Transplant Report--2011. J Heart Lung Transplant. 2011;30:1078–94.
Ulrich C, Hackethal M, Meyer T, Geusau A, Nindl I, Ulrich M, Forschner T, Sterry W, Stockfleth E. Skin infections in organ transplant recipients. J German Soc Dermatol. 2008;6:98–105.
Valantine HA, Luikart H, Doyle R, Theodore J, Hunt S, Oyer P, Robbins R, Berry G, Reitz B. Impact of cytomegalovirus hyperimmune globulin on outcome after cardiothoracic transplantation: a comparative study of combined prophylaxis with CMV hyperimmune globulin plus ganciclovir versus ganciclovir alone. Transplantation. 2001;72:1647–52.
Wang EH, Partovi N, Levy RD, Shapiro RJ, Yoshida EM, Greanya ED. Pneumocystis pneumonia in solid organ transplant recipients: not yet an infection of the past. Transplant Infect Dis. 2012;14:519–25.
Wright AJ, Fishman JA. Central nervous system syndromes in solid organ transplant recipients. Clin Infect Dis. 2014;59:1001–11.
Zuckermann A, Barten MJ. Surgical wound complications after heart transplantation. Transplant Int. 2011;24:627–36.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Lebeaux, D., Coussement, J., Poiree, S., Lortholary, O. (2016). Infections. In: Leone, O., Angelini, A., Bruneval, P., Potena, L. (eds) The Pathology of Cardiac Transplantation. Springer, Cham. https://doi.org/10.1007/978-3-319-46386-5_19
Download citation
DOI: https://doi.org/10.1007/978-3-319-46386-5_19
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-46384-1
Online ISBN: 978-3-319-46386-5
eBook Packages: MedicineMedicine (R0)