
Abstract
When we started using the ILM real time, air quality measurement system in 2013, the ‘what next?” question arose amongst the AiREAS group. Our cooperative venture for creating a healthy city was not just meant to make visible the invisible but also to do something with what we see. The ILM gave us a first detailed glance into the quality of our own living environment.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
2.1 Introduction
When we started using the ILM real time, air quality measurement system in 2013, the ‘what next?’ question arose amongst the AiREAS group. Our cooperative venture for creating a healthy city was not just meant to make visible the invisible but also to do something with what we see. The ILM gave us a first detailed glance into the quality of our own living environment. A multidisciplinary meeting at the end of 2013 came up with several new ideas that garnered the approval of the team. This meant that we would go ahead with multidisciplinary co-creation tables that could help us develop the proposed ideas into a project. A ‘project’ in AiREAS is always a complex initiative with an agreed-upon time span, an expected result and a commitment from the diversity of partners who lend it their resources, such as talent, energy, money, etc. Until that agreement is reached, it is only a positive intention, and not yet a project.

The effort to get from the idea stage to the project stage is coordinated by a so-called Sustainocrat , a totally independent professional who connects the many fragmented interests around the multidisciplinary, sustainocratic table. In the world of payments, the person who pays tends to lead the transaction. In the world of co-creation, money is not the leading factor, the higher purpose is. Money is a means, just like knowledge, input, technology , infrastructures, ideas, etc. Out of the co-creation, a variety of new values are obtained that can be made available again for the economy of growth. The results of our own AiREAS phase 1 had produced two show cases: the way of working at a peer 4 level and the ILM measurement infrastructure for feeding innovation through qualified real time open data gathering and interpretation . These show cases were already attracting attention from all over the world.
The POP was suggested by two different people, each with their own half of the idea. Dr. Eric de Groot is a specialist who researches heart and vascular deterioration due to air pollution. Eric suggested comparing the local exposure of people to air pollution with the effects on their health. He argued that a population of 4000 individuals would be needed to achieve results that were both scientific and practical. The individuals would represent a cross-section of the entire population and be followed over a particular period of time, for instance, 8 years. If, in the meantime, measures were to be taken in town, this should show up in the heart and vascular health evolution of this population.
Ben Nas is a social entrepreneur in one of the city quarters of Eindhoven. He is active in FRE2SH ,Footnote 1 a sister organization of AiREAS within the STIR Foundation, dedicated to developing city farming and reconnecting the city’s consumption patterns with its own retriggered productivity. Ben suggested linking air quality to the reuse of space in town for primary need purposes. The rest of the AiREAS group reacted positively, suggesting that Eric and Ben’s ideas might be combined. Both started to lobby for enough further support to turn the idea into a project. Eric presented the idea on numerous occasions in town, in an attempt to get sufficient civilian support. Ben started to list all of the sustainability initiatives in his city quarter to see if they could become involved or connected one way or another, rather than AiREAS reinventing the wheel and ‘competing’ with other pioneers. Ben came to the astonishing number of over 400 civilian initiatives in a population of 60,000, all fragmented and disconnected from each other. Each was somehow connected to the core values we were looking for. He decided to create a cycle route that connected many of the initiatives, since most did not know of each other’s existence.

With all of this human energy invested in core values , each in their own creative way, we still were not anywhere close to finding the support of the 4000 people needed to participate in the medical research. The expected financial investment for the research, spread over 8 years, was estimated to be between 12 and 15 million euros, based on similar research done elsewhere in the world. The city government was in the process of downsizing their organizational and operational costs to compensate for the effects of the credit crisis of 2008 and the growing cost of society. So, project finance needed be sourced from elsewhere (Europe or The Hague, or the other partners). Or we needed to review the project creatively to see how we might obtain the same or better results with reduced financial means. In AiREAS, we had a persistent drive to find ways to move forward, since we believe in our common purpose. We were fixated on the healthy city objective and flexible as to how we might get there. One way to reduce costs was through peer 4 multidisciplinary co-creation. People and organizations invest resources in a multidisciplinary context with their own reciprocal wishes. These are not by any means always expressed in money.
In AiREAS, we use the STIR principle of ‘what exists can be bought at a cost, what does not exist can be co-created and is an investment’. Also, once a value is created, it exists and can be bought by others. New values that are created together can be inserted by the different partners into a new cycle of money-driven expansion. The interaction between value-driven motivation, the co-creation of values and the subsequent expansion of such values worldwide is referred to as the ‘transformation economy ’, as shown in the figure previously displayed. The transformation economy is fed by data and common sense, challenging at all times the establishment with core human value-driven change. This challenge is converted into positive invitations to co-create new values when the stress at the left hand side of the drawing (the transaction economy) builds up. When the transformation economy is not taken seriously, or left to the fragmented speculation of business innovators, we see the cycle interrupted by severe crises. There are always powerful structures on the side of the transaction economy that do not want change and do everything in their power to avoid change out of self-interest . Tension builds up and can lead to an explosive situation. This can be overcome when we include Sustainocracy and the Transformation Economy structurally in the DNA of our human society.
When we were looking at the possibility of involving 4000 people in a healthy city co-creation, we invited house doctor organizations, schools, community managers, etc., to participate. No one accepted the invitation, arguing that they had no time, needed to justify themselves to their financial stakeholders, had no resources, were in crisis themselves, etc. This meant that even if we had the research budget, it would still be extremely difficult to get the right amount of participants. Also, potential partners referred to the many studies that had already been done in the world and asked what use such additional research would have?
It became clear that we needed to apply multidisciplinary persuasion to get the change going that would motivate others to join or help enlarge our mission. It could not simply be a scientific study to fill the bookshelves; it had to suit our purpose of innovative change.
2.2 E-health and Lifestyle
While looking at European funding possibilities, we found that those that might be accessible to us all had a technological and economic drive. Europe’s financial backing was primarily focused on the creation of new jobs, not resolving key local issues with our core values . This had its macro-economic logic, since the hierarchy of governance is financed through taxation of consumption (VAT), contracted labor (income tax) and profitable business development (venture tax). The subsidy program in Europe hence was strongly oriented towards sustaining its own tax structure. Large multinationals were dealing with this lobby, but in the long run, neither were the issues solved, nor were jobs created, despite the enormous amounts of public money invested. Also, at the level of European governance, a new social economic resonance was needed, but this was not yet the reality of the situation. We had to deal with our value-driven reality, with all its potential, and the unjustifiable economic growth focus gripping Brussels.
E-health often came back in the calls, just like the development of handheld devices. But basic network requirements, health analyses and persuasion for change did not. We decided to take on the e-Health challenge within our own context of value-driven citizen interaction and arrived at the decision to include lifestyle analysis in our project using e-health investigation. This decision had huge consequences for the team, the approach and the way we needed to address our program. The mix of medical and social researches, applied technological tools and the many databases to be combined and interpreted first led us to want to see if we could establish a working format and team. The desired persuasive output would be fed by scientific and practical information-gathering and the complexity of value-driven interpretation and communication. The Proof of Principle (POP) was born and enthusiasm grew fast in the AiREAS community. A new scientific member was included from the e-Health perspective, Dr. Ir. Pierre Cluitmans from the University of Technology of Eindhoven. Subsequently, ICT became a hot issue bridging all the disciplines at the database level. The Sustainocrat level was also leveraged from a purely medical and social combination to a holistic approach within the contextual paradigm shift at the level of civilian participation through e-Health and awareness challenges. Now that the project had increased tremendously in terms of complexity and expert involvement, we needed to downsize the objectives to see if we could get it to work. Instead of 4000 citizens, we reduced the minimum initial need to 40.
2.3 The POP Flowchart

The entire process, from idea to project, with financial commitment from the local government and the multidisciplinary involvement of all required talents, had taken 8 months. It has since demanded creativity, in regard to both sticking to our higher purpose and connecting to the drivers for financial support. The team that established itself was:
- Team supervisor:
-
Jean-Paul Close
- Scientifically:
-
Eric de Groot (Vascular) and Pierre Cluitmans (HRV)
- ICT:
-
John Schmeitz , later supported by Andre van der Wiel
- Civilian participation:
-
Jean-Paul Close, Nicolette Meeder , John Schmeitz, Ben Nas
- Government:
-
Sandra van der Sterren
The first-mentioned in each category together formed the core team for discussion of progress and strategy. We engaged in dynamic clustering to deal with the specific issues whenever they arose. A book on the scientific medical and ICT insights and deliverables is written as a Phase 2 publication. This Phase 3 publication sticks to the part that deals with civilian involvement, participation and social innovation.
The POP financing was estimated to be 200,000 euros, 75 % of which was committed to by the city and 25 % by the province.
2.4 Finding 40 Participants
The enthusiasm for starting this project was high, and now that the expertise and resources had been established, one key part was still missing: the civilian participants. We had chosen to do the POP in a region of the city where the most pollution could be expected. Also, we determined that the local population seemed to be active when we measured the number of complaints addressed to the government referring to smells, dust on the cars and windows, etc. The local residents were united through resident’s associations that defended the interests of the people in the region. When we asked the leaders of such associations of neighbors to try to gather 40 local volunteers for the research program, we were both surprised that we received so little response. We extended the call to other associations and always received the same negative attitude. Finding 40 persons was becoming an unexpected obstacle and learning curve . We had been naive in expecting people to jump at an opportunity to address an issue that had triggered their worries and corresponding complaints for such a long time.

This taught us that people resonate with a particular socio-economic paradigm through the investment of their time and attention. This investment is related to expectations and results. Most people work all day in the current money-driven paradigm. When they come home, they want to engage in their hobbies, relax or have family time. Disturbing things like air pollution, dust accumulation, etc., are sufficient to irritate them up to the level of formulating a complaint but not necessarily to crossing the line for personal action. It is much easier to place the responsibility for the burden on the government and ask the pensioners who lead the associations of neighbors to make their complaints known, but when asked to become active in a program, other personal priorities prevail. This observation strengthened our understanding that air quality and health are leadership issues, not democratic ones for consensus, unless the socio-economic culture becomes modified. This would be the same for all sustainocratic core values .
With this in mind, one of our own participants suggested addressing the membership list of the national foundation for Environmental Defense.Footnote 2 These members already resonate with the issue of air quality and most likely would have a positive reaction to participation. The experiment was carried out and indeed a positive response was received.
We had learned that it is important to find combinations within the complex interaction of citizenship, social commitment and expectations in order to get support and participation for our program. This would be key for getting to 4000 participants. The context of people’s own drive is the motivator, not just our invitation to participate. This was an important lesson, but also a worrying indicator. If we could only involve people that had the time and a context-driven motivation, we would never get to a paradigm shift that resonates primarily with such core values as health. We would only be addressing a marginal segment of the population, while the mainstream would remain uninvolved due to the reigning paradigm that produces the problems in the first place and even has a reward system backing it.
Our financial reward system stimulates people to commute between home and work and live a consumerist lifestyle . This reigning paradigm therefore rewards polluting behavior within a continuous push for economic growth. In order to transform the productive resonance of people, we would also need to address the reward system. The people who got involved in the POP did so out of their own very special motivation, which had already been confirmed by their association with and commitment to other groups. Rather than approaching it as a new paradigm, we could use the POP participation to learn about motivation, awareness, communication techniques and mentality change, even if the group had already made steps towards committing to change and the reciprocity Footnote 3 they expected. This required us to see the participants as partners in the process, rather than study objects for scientific interpretation or political influencing.
2.5 The First Encounter
We invited the first group of confirmed participants to an evening during which we would explain what we were going to do. The evening was organized in the temporary research center that we had set up. It gave the participants the chance to see where the interaction would happen and what equipment would be used. The evening was socially oriented, with presentations by the research scientists, and drinks afterwards.
Since the participants had been defined as partners, we had decided to use the evening presentation as a living lab. After the session, the participants were contacted by telephone for feedback. This was key to improving our interaction in our attempt to get the required attitude of proactive innovation rather than them dealing with a passive research object. They were all asked to help us further through active feedback, participation and open reflection. This was to become a highly appreciated red line throughout the project. Scientific research and persuasive communication had become instruments for provoking change and our personalized interaction with the participants would provide us with measurable progress and insights into how to improve or enhance the interaction.
2.6 Feedback Collection
The feedback from our first evening presentation was an eye opener. This research was done by Nicolette Meeder . Nicolette had become a participating member of STIR right from the kickoff date in 2009. She had been active through the FRE2SH experiments in food transition and the STIR Academy of participative learning. Now, she was rapidly integrated into the AiREAS POP complexity, assuming the role of mediating analyst between the participants and the project. This proved to be a fundamentally important role and one to be taken into account for repetition of the program elsewhere or its application in much larger groups.
2.7 Nicolette Meeder Reports on Feedback from the First Evening Session
The general sense of the evening was that people:
-
attended with a positive and motivated feeling
-
felt the need to work on air quality together
-
were prepared to attend further meetings
-
also wanted to participate in other AiREAS activities
-
felt this to be a nice approach, connected with other, more social cohesions
-
felt confusion about the evening and needed clearer communication about what was expected from them.
Suggestions for the next meeting:
-
better indication as to how to reach the location
-
welcoming by the organizers
-
provision of a name badge for both organizers and presenters
-
agenda of the evening
-
greater structure and adherence to the schedule.
The presentations:
-
clear for some, but too scientific and complex for most
-
one participant requested more Dutch language material rather than the abundant technical jargon in English
-
information needed to be more practical, more focused on what was actually going to happen
-
a short introduction to the entire objective would be preferable
-
a clear explanation of what was expected from the participants
-
use of fewer sheets per explanation, 1 or 2 being sufficient.
People also liked the following ideas:
-
having room for questions and discussion
-
having people give their names when speaking, in order to move beyond the sphere of anonymity
-
allowing demo materials to be circulated so they might be felt, seen, touched, etc.
-
seeing more cohesion between the speakers instead of fragmented bursts of knowledge and expertise
-
getting the sense of a good and well-harmonized organization, giving a feeling of comfort and safety.
In general, the participants want to be taken by the hand in a positive manner and guided through the entire process, both in terms of the structure throughout the evening but also of a more concrete plan to achieve a healthy city. The personal interviews were taken as a human and necessary experience. As a result of these, one feels seen and heard, and taken seriously in a positive progression.
2.8 End of the Report
With this, Nicolette consolidated the team through an unexpected and unplanned contribution. It confirmed for the first time the complexity of the POP and the flexibility needed to shape our progress without losing sight of our higher purpose. This would become the attitude throughout the project and key to its success.
As a consequence, Nicolette was, of course, asked to organize the second evening session with the next group of participants, using the feedback from the first. She also had to convince the diversity of research partners to adjust their interaction as a result of the feedback. This became a challenge of self-reflection for all involved. The professionals initially felt criticized and attacked in their professional self-esteem. But this was a temporary initial reaction to the new approach of extended partnership and the fixation of the focus on persuasion rather than just research. Step by step, the group of researchers also started to understand their particular role and developed a new kind of empathy with our AiREAS mission. They understood that they are not only valued for their scientific expertise, which needed no confirmation anyway. They are also recognized as scientific influencers of value-driven processes geared towards a desired end result of innovative change , measurable health and air quality development. This combination made AiREAS stand out from any other research done elsewhere in the world and lent an extra dimension to the involvement of our professionals. Apart from their islands of expertise, they are being extra-valued for their empathy with the team as a whole and their contribution to the overall objective.
2.9 Setting the Tone
After just one evening’s session and feedback loop, the productive, result-driven tone was set for the entire POP from a Sustainocratic perspective. We were all now acting as a value-driven group, not as a bunch of fragmented, specialized participants. We entered a learning curve that affected every member of the team with just one objective, the health ideal of AiREAS through lifestyle , air quality and our resonance with a perceived reality.
The second evening session was done in a way that was 100 % empathic with the group. The second round of feedback was also very much more in line with the group’s expectations and interaction as a team. A positive vibe had been achieved.
Nicolette became responsible for creating the agenda, having personal interaction with the participants and coordinating the interviews for the purpose of obtaining background information about the lifestyles of the people involved. Every human being may be equal, but from a biological and behavioral point of view, we all differ. The interviews were meant to provide context around each individual being examined, using various forms of medical expertise. We first researched their health by measuring the aging of their heart and arteries. We also subsequently researched the variability of their heart rate during the diverse activities that each went through during their normal day. GPS tracking determined the positioning of the person in town and their possible exposure to air pollution when outdoors in the city. Questions were also asked about the way people moved about town. There is a huge difference between riding a bike, walking and commuting by car or bus. Also, the ratio between outdoor and indoor presence is relevant for the interpretation of data.
We needed to cultivate a strong sense of responsibility in the fields of ethics and privacy. We were obtaining a lot of data from each individual that could not be shared with anyone other than the person in question. For the sake of interpretation, we needed to depersonalize the data and look at it from an objective, not subjective, point of view. The group of living objects was of interest for the study of behavior as if they were molecules in a lively environment. When providing individual feedback, the objective and subjective contexts could be brought together so that the individual might develop awareness and do something with the insight.
2.10 Data Validation
This introduced a unique new element into the investigation and usage of data. Data validation is done by experts who look at possible strange deviations that do not comply with the logic of accumulated experience. These deviations can be caused by malfunctioning equipment, errors in the programming or faults in the technological communication and database management systems. This intelligence is key to making sure that we use the right data for interpretation . But this goes for all data, including interviewing and human interaction. When combining datasets, the logic of its outcome can be judged against accumulated experience. But when these experiences don’t exist, there is nothing to benchmark against. The validation of our findings then needs to be verified through dialogue between all participants, observation of the real situation and registering of the unknown for further investigation or detection of recurring circumstances. A whole new field of knowledge-gathering appeared with a complexity of interpretation against rational logic, leaving room for error and further verification.
2.11 Influencing People
During the POP’s medical and lifestyle examination, the participants were not only influenced by the research itself and the data they could obtain. They confirmed that they were especially influenced by the questions providing continuous feedback in their partnership within the team and their participation in the different elements of the program. It was the questions that made the people process their thoughts. The medical and area researchers showed great empathy and took their time in explaining the working method and expected results to each of the participants individually. The need to reflect personally afterwards, in order to give relevant answers to the feedback questions, got all the partners to open up to reality in a new way. Some of the awareness triggers were:
-
The opportunity to observe your own heartbeat and vascular behavior in real life and in color, without pain or invasive methods. This was an eye opener for most participants. It was also necessary to further understand the aging of the artery walls and measures people could take by themselves to improve their vascular and overall health.
-
The GPS tracker that showed the whereabouts of someone during the day when plotted on a map of the city. We all live our daily routines and hardly reflect on our traces until we see it in a picture.
-
Wearing instruments for heart rate variability . This made people much more aware of their daily activities, their environment, their respiration and the reaction of the body. ‘Will this show on the graphs?’ fostered a strange sense of curiosity and self-sensitivity. People would adjust their respiration or try to control their heartbeats simply because of the awareness that everything was being registered. This was not only done to positively influence the readings but also to experiment with the different situations they encountered in daily life. In a way, they became researchers themselves.
-
The questions about registering the whereabouts of the participants during the day. These revealed that most people spend the greater part of their time indoors (90–95 % of the time).
-
That lifestyle is key in determining the level of exposure to pollution and all sorts of triggers that may produce physical damage or stress.
2.12 Producing Individual Reports
The POP research with this particular group continued through June 2015. The conclusion of the physical analysis program was cause for a collective celebration, during which the scientists could present their early findings. For the medical and civilian participation teams, it all really started then. The data needed to be interpreted per set and then combined to get as complete a holistic picture of every individual as possible. This is, of course, just a moment in a lifetime, but it still gives interesting feedback and insight into our current lifestyle patterns. The POP team was not only surprised at the enormous amount of data that had been generated with a relatively small population; we also found a surprising richness in information and insight due to the cross-referencing possibilities of the different data sets. We could have spent years analyzing the data in many different compositions, but that is not the purpose of AiREAS. AiREAS wants to take steps towards developing health and a healthy city . The focus was therefore on finding ways to use the data adequately and persuasively by becoming selective. Individually, each research specialist can, of course, still do in-depth research themselves with the data obtained, but from an AiREAS perspective, it’s the result-driven persuasion and communication that prevails, with measurable results to be registered in terms of positive innovation and change.
2.13 The Results
The details of this research from a medical perspective can be read in the specific publication of this AiREAS Phase 2. It took the period from June 2015 to November 2015 to interpret the different data and get to a combined analysis with feedback for each of the participants. As mentioned before, the personalized report is obviously subject to privacy. Here, we reproduce the depersonalized report as we gave it to the participants, together with their very specific private results. The very specific personal results we cannot share here.
The process was finalized through yet another feedback call from Nicolette, who tried to get a feel for the degree of change that the exercise had provoked in the mentality or behavior of the participants.

When looking at the picture above, we need to be aware that:
-
the interview took place 6 months after the physical measurements
-
also, immediately after participants had obtained the personalized reports
-
the group already had a high awareness level at the start (>3) due to personal choices of cohesion and participation.
Having said that, we ask ourselves what achievements we might be able to make when dealing with totally unaware and uninvolved groups?
To finalize this chapter, we share below a depersonalized copy of the final report, translated into English. The report is published under the Local AiREAS Eindhoven heading. Every AiREAS region has its own Local AiREAS platform, which allows us to allocate the innovations generated in a region to that community and share the inspiration, innovation and implementation invitation through the STIR HUB network among all Local AiREAS. Potential royalties included in the expansion process are allocated to the region where the innovation was created.
We will conclude the chapter with specific findings after the report.


Dear participant,
You have participated in a trial project in which we tried to find a relationship between air quality and health on the one hand, and motivation, behavior, awareness and behavioral change on the other. The project, therefore, does not deal primarily with the research, but rather how it affects you as a participant and partner.
Information and communication can produce a variety of behavioral reactions, which we summarize here for you:
-
(1)
No reaction: It may have been fun to participate, but it did little to nothing for me. I continue to live my life as usual.
-
(2)
The best defense: I have good reasons to live as I live and will not let myself be influenced that easily.
-
(3)
Passive behavioral change : I am now (more) aware of air pollution and its possible effects on my health. I will try my best to avoid the most polluted areas to reduce my exposure.
-
(4)
Active behavioral change : I am (more) aware of my own possible contribution to air pollution and will try to reduce my own polluting patterns.
-
(5)
Innovative change:
-
(a)
My consumption behavior has changed. I look very closely at what I purchase now and when something needs to be changed because it pollutes, I will look for less polluting alternatives.
-
(b)
I have begun to undertake action. It stimulated me so much that I became creative. I started to think of all kinds of innovations that could reduce the pollution caused by myself and others.
-
(a)
The AiREAS POP focuses especially on points 3, 4 and 5 with the information we supply. We are curious to see if we have managed to produce a significant contribution and will ask you for feedback at regular intervals. Of course, we will share our findings with you as well.
2.14 Introduction to AiREAS
2.14.1 What Is Aireas About?
AiREAS is a cooperative association that arose from the STIR Foundation, better known as City of Tomorrow. The STIR Foundation was founded in 2009 in response to the credit crisis and growing tension around the world as a result of the huge number of economic bubbles that have made our lives and lifestyles extremely vulnerable. STIR has been experimenting with new ways of connecting society to our core responsibilities in order to achieve sustainable (human) progress and harmonically progressive communities. From this was developed Sustainocracy , a type of democracy based on core natural and human values. AiREAS (air quality, health and regional dynamics) became one of the first sustainocratic ventures in the world. The Province of North Brabant became our Proof of Concept and the city of Eindhoven our living lab and Proof of Principle .
Along with AiREAS, other initiatives were also created. These cooperatives have the commonality that they develop core human and natural values in which citizens, local government, scientists and innovative entrepreneurs work together. Other initiatives are:
-
FRE2SH and FRE2SH Farms (Food, Education, Energy, Recreation , Regional Self-Sufficiency and Health)
-
STIR participative learning cooperation (Awareness, empathy and co-creation)
-
STIR HUB Inspiration, innovation and implementation, sharing innovation between regions.
-
SAFE , a research community examining how we can reduce our dependence on dangerous resources.
By placing your personal perception of reality at the center of our attention, combined with knowledge about air quality, mobility and health parameters, we have together made Eindhoven unique and core value-driven around health. AiREAS Eindhoven invited you to contribute to your own health as well as that of the environment in which you live and are active. Starting a local AiREAS is possible in any region, city or village.
For more information about AiREAS and a review about air quality, please consult the website: www.AiREAS.com and/or the AiREAS blog https://globalAiREAS.wordpress.com/.
2.15 Core Values
2.15.1 Why Take Core Values as the Starting Point?
There are 5 core values , or basic principles of sustainable life, that the STIR Foundation uses to define sustainable human progress . Those core values are a part of the dynamics of all life forms, not just the human being. If a core value is not respected, it will always lead to the disappearance of life or the lifeform. We sense this as a crisis, but in reality, it is part of our evolution, and we need to adjust continuously to fit into the complexity of life in general.
We human beings can only make self-aware evolutionary decisions about our own behavior and our symbiotic relationship with our surroundings. We will deal here specifically with the human being in context with the environment of which we are an integral part based on equality . Bacteria, fungi, insects, plants, animals, fish, etc., deal with the same core values for their own evolution.
-
1.
Food (primary resource, including drinking water and the air we breathe)
-
2.
Health (including maintaining a healthy environment)
-
3.
Safety (including respect for and integrity among each other)
-
4.
Regional Self-Sufficiency (including taking responsibility together for regional mutual resilience)
-
5.
Self-awareness (including new educational processes).
If one or more of these core values is underestimated or neglected, it will put life under pressure and our wellness will decline in all aspects. The context (how you perceive yourself, your role and life’s core values) of your own situation is always the starting point. This personal context description comes primarily from the interviews that you had with Nicolette Meeder .
Our objective is that you will not just get more insight into the 5 core values, but will also become more aware of them and how they can positively influence your own situation. We hope therefore to contribute more than simple summarizing observations, by also providing you with guidance for your own future choices. For better understanding, we explore each core value here a bit more.
2.15.2 Core Value: Food
Food, water and air are the building bricks and connections of life. Food is also storage of the solar energy contained in the processes of life of the plants and animals that we eat. We eat our own evolution contained in the DNA of our system. An average human being consumes, per day:
-
1 kilo of food
-
3 kilos of water
-
30 kilos of air
What we consume is part of living and sustaining our lives, including the stored solar energy that provides us with our own energy through digestive processes. If we pollute or manipulate water, food or air, we do the same to ourselves and the billions-of-years-old mechanisms of life stored in our systems. The consequences form a genetic anthropocene Footnote 4 in which anything can happen. In exceptional cases, a new species can develop out of our own destructive processes. But mostly, the manipulating sort disappears, due to a lack of harmony with the larger context. Every human being itself is already a living harmonic mechanism that is sustained through symbiotic interaction with billions of microscopic life forms. When that is disturbed, the human being will go into decline, just as we bring our surroundings into decline. Natural food, water and air hence are core values , because we owe our physical and energetic existence to it.
2.15.3 Core Value: Health
Life is, in essence, always healthy. If unhealthy, it will die or be consumed by healthier species to provide room for a new healthy life cycle. If we accept our polluting, unhealthy socio-economic system and lifestyles , we will contribute to our own self-destruction. It is that simple.
Health is hence a core value. This core value is not just about our own health, but also that of our environment.
2.15.4 Core Value: Safety
Safety is an essential value for creating society (family, community, protection). Without safety, this would be impossible, as everyone would be stuck in the individual mode for survival rather than cohesion . Safety is key to being able to deal with the fear that goes with awareness. Safety translates into mutual respect, integrity, listening to each other, and empathy with yourself and the people around you. It relates to a place to live, clothing, warmth, equality of opportunity and societal positioning. Safety is the “right to BE”. Safety protects life.
2.15.5 Core Value: Self-sufficiency—Local Mutual Resilience
Regional self-sufficiency and mutual resilience are the basis of the creation of a society. We cannot produce all our needs ourselves and need to work as a team. But if we make ourselves dependent on a (care) system, we lose our connection to our own natural reality. We enter easily into a state of greed and apathy which becomes the basis for the appearance of hierarchies of power and control. Only regional self-sufficiency keeps us alert to the changing circumstances that require our innovative drive. Hierarchies are deadly structures when they don’t deal with the core values and just focus on power and control.
This core value hence also deals with the need to take responsibility for our own local resilience and the freedom to take responsibility when needed. Freedom hence is not without obligation, but rather is obtained when, as an individual and/or community, we commit to our sustainocratic core values and bring in our talent and energy to produce common sustainable progress.
2.15.6 Core Value: Self-awareness
Self-awareness is the rational, spiritual, physical and emotional connection between the above and the wellness development of our community. It applies not only to the individual, but also to our community and the entire society format. Our world history, together with the developed scientific knowledge, provides us with all we need to progress in a wise and sustainable way, with wellness in abundance without the destruction of our habitat.
This core value also deals with the educational processes of lifelong participative learning, as developed and deployed in the STIR Academy.
2.16 Observations
In this report, we provide you with the most important observations from the research.
2.16.1 Personal Situation
In this section, we share the information we received from you during the interviews.Footnote 5
General awareness:
-
Participant sees more aspects that influence health (some examples):
-
1. Bad sleep, wakes up a few times per night due to the noise of the highway.
-
2. Exhaust gases, sore throats, sometimes shortage of breath.
-
3. Disturbance from barbecues and wood stoves.
-
Experiences stress when having to leave home for work.
-
Participant feels healthy and tries to keep it that way (examples):
-
1. Jogging 2× per week
-
2. Cycles a lot
-
Eliminates stress through walking and cycling.
-
Participant uses no medications.
We have GPS-tracker and HRV measurement data from March 4–11, 2015 and April 15–22, 2015. We made echoes on March 11 and April 22.
On your location form, you have indicated (various examples of responses):
-
Outdoor activity between 1 and 3 h per day
-
Most important transport device: bike
A word cloud was produced for each interview. In one glance, the participant could see the emphasis placed by him or her on the different aspects of living life.

2.16.2 Position Determination During the Measurement Period(s)
During the pre-study, you were given a GPS-tracker with which we could map your position in town and relate it to the closest airbox. Below, you will find a map overview of all the airboxes in Eindhoven.

2.16.3 Exposure to Air Pollution
As we register data from the AiREAS Innovative Measurement System (ILM) in near real time, we can combine this with your position and determine your exposure to air pollution . This is just an indication, because you are not always in the direct neighborhood of the airbox, and also spend most of your time indoors . The Airbox is connected to a light post at a fixed location in town. Interpretation of your exposure is therefore always subject to modulation and indication.
The concentration of fine dust inside a building can, indeed, sometimes be up to 2.5 times higher than what we measure outdoors , depending on the situation inside and outside. There are also examples of buildings with good climate management in which the situation inside is better than that outside. Higher concentrations indoors can be caused by activities like:
-
Smoking
-
Open fireplace /stove
-
Vacuum cleaning /changing the bed
-
Cooking
-
Indoor construction work
-
Hobbies
For personal exposure, we have chosen the fine dust with an aerodynamic diameter smaller than 2.5 micrometers, referred to as PM2.5.
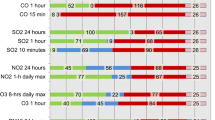
In the table below, established by the Ministry of Health, you can see that the concentration point that determines the PM2.5 transition from “Good” to “Moderate” is placed at 20 µg/m3. We keep these reference values during our research period. If the measurement of one or more airboxes shows values above those thresholds, then we can assume a situation of the worst air quality and hence a larger possible impact on your health. The qualification of “Good” is relative too. Air pollution is always bad. Very sensitive people can also feel discomfort at lower levels of fine dust. Everything therefore depends on the particular situation of a person and environment.
The table with value indicators was established by the RIVM (Ministry of Health) in cooperation with IRAS (Risk Assessment of the University Utrecht). Information can also be found on the AiREAS site: http://www.AiREAS.com.

In the graphical representation of exposure, the black line represents the threshold between ‘Good’ (below the line) and ‘Moderate’ (above the line). Underneath, in the same graphic, you find colored boxes with the numbers of the airboxes. The same color of the airbox is then traceable in the measurements. You can also find the same numbers on the back of the city map that we have shown before.

There was a problem with airbox 24 on March 5, 2015, which is also shown in the graphics. Apart from that, the values remained below the norm, except for March 10. Then, the value peaked up to 30 µg/m3.

Above, we see that all the values remained well under the reference line for the days of our study. Only on April 16 did the values peak a little towards the threshold.
2.16.4 Heart Rate Variability (HRV) and Motion Measurement
Twice, you were asked to wear measurement equipment on your body for one week, with which we could determine and register the variations in your heart rhythms. This indicates degrees of stress. We also register movements, allowing us to determine whether you were active or resting.


In the figure above, you see that the time between heart beats never remains the same. The heart is no clock. The variation is natural and is caused by our brain, which keeps regulating the rhythm. Two separate nerve tracks inside our body interact and neither can be influenced by our will. One nerve track is part of our stress system and has the tendency to make our heart beat faster. The other is part of our recovery and relax system, and has exactly the opposite effect. Both systems interact continuously in some kind of competition, sometimes with one track dominating in one heartbeat , and the other dominating in the very next. This also determines the variety we observe in the measured data.
We have accumulated a trustworthy set of data around your particular measurements. In the graphic below, we show the heartbeat intervals from beat to beat on Saturday, April 18 (participant number 3). It may look kind of messy, but our experts can still distill a reliable image of your heart rate variability during that day.

We can look at these fluctuations in beat to beat rhythm (HRV) in different ways. What we did with these HRV data is to relate them to the average motion velocity that we get from the GPS tracker averages and the average reference of your own for that week. No general standard values are known yet for HRV values, so this is the best we can do at this stage, and yet it already provides interesting insights.

The first line in the graphic above shows the speed we determined from the GPS trackers. We can sometimes see a strange, straight line, as opposed to the mountainous curves. This means that, during that period of time, we received no data at all. Also important is the realization that if this graphic representation does not show a huge speed variation, this does not mean that an individual has not been subject to great tension, causing peaks in heartbeats . The 2nd line or part shows the average heartbeat. The other three show measurements of different HRV variables. The graphs are in Dutch. The translation of the interpretation for this Saturday is provided here:
-
km/h: Participant number and measurement week: GPS speed, weekly average of this case: 2.5 km/h
-
BPM: Average heartbeat. Weekly average (this case): 71.2 beats/min
-
ms: RMSSD, higher values = more relaxed—weekly average (this case): 60.5 ms
-
ms: SD1 (short term HRV: higher values = tension peak)—weekly average (just this case): 108.1 ms
-
ms: SD2 (global HRV: higher values = long period of tension)—weekly average (just this case): 128.6 ms
In the reference case above, personalized feedback is provided in the sense of:
The average heartbeat of just above 70 beats/min is perfectly normal. It is interesting to see that no large deviations are detected over a significant period of 10 h. In the middle graph (RMSSD), we see the most used HRV numbers. This is just one of the ways to look at the balance between the interaction of stress and relaxation. In your particular graphic, we see more fluctuations there than in the one of the heartbeat. Around noon, there is a clear moment of rest. Also, between 15:15 and 16:45, we see this period of relaxation. The same returns in the other graphs below the middle one, but is less prominently visible.
On Monday, April 20, we see another pattern:

Early in the morning (between 4 and 5) and between 15:00 and 15:15, we see from the GPS speed that biking activity was most probably undertaken. The HRV graphs (RMSSD, SD1 and SD2) show a period of relaxation between 8:30 and 9:00. It is interesting is to see that, during the biking activity, relaxation seems to increase.
2.16.5 Echo Vascular Tension
To get an impression of the health of your heart and blood vessels, the left and right neck arteries (medical term: arteria carotids ) were measured using modern echo techniques. In addition, the same was done with the artery in your right arm (the arteria brachialis). An echo-image is made with (inaudible) sound waves, which is non-invasive and totally friendly for the human being.
Measuring the thickness of the walls of the neck artery
The neck arteries (carotids) are important distribution channels of oxygen-rich blood to the brain. For the body, they are very large in size, with a diameter ranging between about 0.7–1.1 cm. The arteries run just underneath the surface of the skin, on the left and right sides of the neck. They relate very closely to the heart; if you put your fingers on your neck, you can feel the pulse.

It’s a fact that everyone gets older and that artery walls get thicker with age. This increase in thickness is a normal process, but is influenced by risk-factors that accelerate the thickening. Because the thickness of the arteries in the neck can easily be determined with non-invasive , painless echography, it has become one of the most popular methods for determining the long-term risk factor of heart problems. The method is relatively simple, very accurate and very well reproducible in imaging techniques. It is also a very good indicator of the condition of the rest of the blood vessels in the body.
How does this work? The thicker the artery wall gets, the greater the risk that extra local thickness will appear (atherosclerotic plaque) . Sometimes, this leads to the total closure of the artery (occlusion) with all the consequences that follow. There is also an increased chance for the formation of blood clots (thrombosis) caused by this atherosclerosis. Well-known (or better yet, infamous) are the decreased bloodstream functions of the coronary arteries around the heart (coronary atherosclerosis), in the neck or elsewhere in the body, sometimes with closures and the whole host of heart and artery problems as a consequence.
From previous (echo) artery investigations over periods of more than 25 years with many thousands of participants, we know that the thickness of the carotid wall, under normal circumstances, increases with age from about 0.4 mm at birth to about 0.8 mm when you are 80 years old (blue line in the graphic below).

Since getting older is something you cannot avoid, we call this a non-modifiable risk factor for health. The thickness of your artery wall increases (much) faster when you are exposed to particular risk factors for heart and artery illnesses (the red line in the graph). This artery thickness is an important indicator of health. In vascular medicine, a saying is used—that you are as ‘old as your arteries’.
Smoking, high cholesterol, high blood pressure and exposure to air pollution are important, subject to influence modifiable risk factors. Nowadays, we know that if you address the modifiable risk factors, for instance, through a healthy lifestyle , the arteries get thinner and the natural thickening process once again slows down. The good news is therefore that artery thickness can be influenced in a positive sense.

Addressing the modifiable risk factor with healthy food, adequate physical exercise and fresh air, one can improve health before problems occur (primary prevention) or reduce the chances of renewed problems after illness (secondary prevention ). The sooner one reacts, the better the possible outcome.


Functionality of the arm artery using echo-equipment
This research was also performed by Dr. Eric de Groot and is described in detail in the book on Phase 2. The investigation concentrated on the functional vitality of the arteries. This so-called flow-mediated-dilatation (FMD) is a valid short term risk-indicator of the inner lining of the arteries, the endothelial . The wall of the artery is influenced by the (autonomous) nervous system, as well as by all kinds of molecules through receptors on the endothelial cells and in the blood stream. The endothelial, in fact, organizes the interaction between the blood stream and arterial functionality. Especially ultrafine dust (UFP) can disturb the nervous system and the endothelial function, and also therefore all vascular functionality. Long-term vascular disturbance causes an increase in the risk of heart and vascular diseases, as well as lung illnesses.
With FMD, we look at the way the blood vessel widens when the stream accelerates after applying a temporary (5 min) blood pressure cuff around the lower arm that closes the artery for a short moment.

After reducing the tension of the cuff, the bloodstream, which had built up tension due to pressure on the artery, will temporarily speed up. This increase triggers receptors on the inner lining of the artery that rapidly release a small molecule (nitrogen oxide, NO) to the muscle layer in the artery wall. This NO-release relaxes the muscular layer of the artery wall: the diameter of the artery can thus increase. This NO release and the echographically-measured blood vessel diameter increase are measures of the health of the endothelial . Since the inner lining of all the blood vessels in the body consist of endothelial, the measurements are a representative value for the artery functionality of the whole body.

A healthy endothelial shall release more NO and induce a larger widening than a less healthy endothelial. Someone with a healthy endothelial will therefore have a higher FMD.
A typical arm artery has a diameter of 3–5 mm and can widen about 5–10 % (i.e., between 0.15 and 0.5 mm!). Echographic measurement is therefore not very easy. The FMD also varies a fair amount under the influence of coffee, smoking, physical activity and food. In order to obtain a reproducible FMD, a participant needs to be sober and in a state of rest. There are no clear reference values for FMD, but the “normal” value will be somewhere between 4 and 10 %. Just as with the wall thickness, we also took average values of the available FMD measurements.
Following this information, the participant receives their personal FMD measurement and an assessment by the medical research specialist. If something really significant is detected that may prove dangerous for the participant, then the team contacts the individual so as to advise them to contact the house doctor and consult with them regarding the personalized report.
2.17 Conclusions
From all of the AiREAS POP researches, we can determine that exposure to air pollution is very much related to individual lifestyle and daily activities. The composition of air pollution also varies constantly, causing a diversity of effects on our bodies. Normally, our bodies know pretty well, through a natural drive for self-regulation based on health, how to deal with outside influences. There are, however, plenty of factors influencing the human being that directly or indirectly damage our health. Some of them we have a hand in ourselves, and with the right knowledge, we can positively influence our wellness and the quality of life for ourselves and our environment. This does not just produce better physical health, but also a much greater degree of pleasure in life, higher general productivity and an improved sense of well-being. The POP research has tried to make this visible for you.
In general, we can state that human health is determined by what we eat, breathe, drink and how we move physically with the right motivation. Awareness of these factors also alerts us to the elements that can be act as disturbances. We tend to be more aware of the origins and quality of our food. We tend to stop smoking and ventilate our houses better. We more often travel by bike or public transportation, leaving the car at home or even selling it altogether. Things that used to determine the coziness of our homes, like an open fire, candles or aromatic sticks, are replaced by other healthier, more positive alternatives. We also notice that we are talking with each other more and more often about subjects like air quality and health.
There are also things we cannot influence because they belong to our DNA-related system, or they are engrained in the reigning culture or structure of society, or they are endemic to the climate in which we live. That is why AiREAS also involves the government, science and innovative entrepreneurship in our common mission. The POP investigation is therefore valuable for influencing every aspect of society and stimulating innovation in which we can all be involved.
With our research, we try to give reassurance to everyone that this can all have a positive effect on our health and well-being, as well as a positive outcome for the global issues we face, just by giving the example and showing the results. Hopefully, you have received sufficient tips and insights to enable you to make up your own mind and take action accordingly. If you need help, you can always rely on the support of the entire AiREAS team of partners, including all specialized professionals.
In the name of the entire POP team, we thank you for your involvement and value-driven input.
2.17.1 Information Sources
The sources we used for information:
-
Exposure: Concentrations of fine dust and Ozone during the research period via the ILM ;
-
Position: General displacement pattern during the day using a GPS tracker;
-
Speed: Mobility based on speed via the GPS tracker;
-
HRV: Heart rhythm variations as indicators for stress;
-
Movement sensor HRV: Circumstances (movement or rest) in moments of stress indications;
-
Echo blood arteries: Long-term effect of lifestyle and circumstances;
Interviews: Subject’s age and perception of their health and environment.
-
////End of individual POP feedback////
2.18 Specific Conclusion of the POP Project
The POP was developed around two core themes: medical research and the participation of civilians. The medical research has been detailed in a specific publication (Phase 2). This current publication uses the medical outcome for measurable social innovation. We found both challenging and innovative results in developing such complexity.
2.19 Challenges Encountered
-
The team member’s specialties tend to work on specific islands of expertise in which each excels. The team itself and the required end results, however, need the sum of all experts, linked together through the interpretation of the different individual results in a combined complexity. In a well-integrated team, 1 + 1 rapidly becomes much more than 2. A badly integrated team produces a negative outcome: 1 + 1 = 1.5 or even less. We spent a lot of time becoming a well-integrated team with a positive outcome that was even greater than we expected.
-
The team had to get into the habit of remembering that the participants were also part of the team and key for feedback and measurable co-creation through social innovation, executive value-driven interaction and entrepreneurship . This feedback loop proved essential for the flow, analysis and optimization of the POP .
-
Our city of Eindhoven consists of many more cultures beyond just the Dutch. How do we involve all of them? We needed to experiment with this, and ended up having unexpected positive experiences with the Turkish subculture . This is described in Chap. 6.
-
The HRV data contains so much detail on a microsecond level that it requires automated support to analyze such a massive amount of information. The equipment used, however, produced skin irritation for our participants. We could use the data but decided that, for a research population of 4000, we would need to find other, less irritable solutions. Only when some HRV standard exists or we determine a preferred system will we be able to develop an automated pre-analysis of the data. The true validation and analysis is always done by human specialists and scientists through interpretation of various datasets, yet the computer can eliminate many hours of nitty gritty micro-analysis.
-
We gathered 11 different databases, each with scientifically-valuable information, especially when further used in combination. This produced an immense amount of cross-referencing options for multi-data interpretation purposes. We spent a lot of time making choices based on the persuasive purpose of the POP rather than the many other interests that we could have developed around analyzing data combinations.
-
If combined with other open public data sources, such as historical health information, traffic intensity, weather and climate data, the challenge risks becoming huge and chaotic without any clear added value. This may be of interest for students, but not for triggering health innovation. Choices in this field also needed to be made.
-
We needed to stick very closely to the higher purpose of influencing and developing a healthy city through healthy innovation, as well as continuously managing the relationship of every research aspect to this common purpose.
-
Very special and critical attention went to the ILM calibration and validation routines, since we needed to use the reliable and qualified data for our own health and lifestyle research and civilian feedback. This gave rise to the creation of a new AiREAS team, the CalVal team.
-
A lot of discussion arose as to the way to report back to the participants and trigger their response. To what depth should the response go, and what might trigger awareness and even reaction? We decided always to take the positive ‘can do’ approach, with an invitation to take personal action for change.
-
Finally, it became a challenge to get each researcher to produce publishable material. An exercise in human interaction is experienced with great professional love and passion, but the project is only finished when the documentation has been delivered. This is not just important for sharing our findings with the world; it also helps when we want to expand the activities to the 4000 people in Eindhoven or somewhere else in the world.
2.20 Innovative Results
-
The POP brought us to the insight that life is always health-driven. This positive driver in a healthy city challenge produces very positive vibes among the participants.
-
People tend to resonate with a reality that produces rewards. This reciprocity is not always measured in money. A learning curve , a sense of purpose , belonging to a group, secondary value development (an increase in the value of my house), worries about family members with health problems, etc., are deliverables that motivate people just as much as money may. We also introduced the AiREAS coin as a token of appreciation for value creation. With the token, people could attend STIR evening inspiration and college sessions to learn still more about peer 4 regional development and individual participation.
-
The POP got us to use technological innovations to develop research insights, but also successfully to stimulate the entrepreneurship within our own group of partners, as well as new small and medium entrepreneurial initiatives.
-
The POP, combined with the ILM experiences described in our first publication, got us to redefine our interaction at the different levels of regional development and automated activities. The whole link with peer 4 (see Chap. 7) of our own City of Tomorrow views could be related to the Presencing InstituteFootnote 6 and VentureSpring reports of Smart City development in Eindhoven. It came alive in the specific need for value-driven interaction between the layers. The ‘large buttons’ team was created to link the various levels of quality that are needed for proper interaction.

-
The interaction we developed with other cultures in town, of which the Turkish community is the most representative, with a local population of about 10,000, gained us very special insights that are worth further exploration. A special chapter (Chap. 6) is dedicated to this. The key insight became that core human values are creating social cohesion while political/economic drivers tend to produce fragmentation and segregation.
-
We truly established a well-structured team capable of addressing this complexity in a magnificent way. We have overcome obstacles and found solutions together. The dynamics are typical of this team, due to the human bonds and cohesion that developed. It will become a challenge to train other teams elsewhere to do the same.
Despite the enormous amount of information gathered, we remained unsatisfied, because we had only covered a minute part of the city’s population and the possible motivations around core values that connect or disconnect people. The medical complexity of expensive equipment and highly-trained people required us to spend a significant amount of the budget. But from a civilian participation point of view, a sufficient number of arguments had been discovered to justify trying to find new contexts and experimentation to broaden our views. POP1 had become an important part of the toolkit that a city can use to measure its health-driven progress, but we needed it to be connected to the city as a whole. We opened ourselves up to experiments, not knowing where this would take us. Being now known in the world in a new socio-economic context, with the ILM and POP1 as key instruments, we became visible to others. Our flexibility as a team did the rest as can be read in the subsequent chapters.
Notes
- 1.
FRE2SH stands for regional resilience in Food, Recreation, Energy, Education, Safety and Health through co-creation.
- 2.
Milieudefensie.
- 3.
Reciprocity became a key factor in our approach, as it refers, for us, to a much broader diversity of return on effort than the financial reward system. https://en.wiktionary.org/wiki/reciprocity.
- 4.
Anthropocene - the era in which our planet’s climate, atmosphere and soil are experiencing the specific results of human activities. https://en.wikipedia.org/wiki/Anthropocene.
- 5.
The statements reflected here are examples. In the real report, the actual statements of the individual are reported with feedback.
- 6.
https://www.presencing.com/ know from the U-Theory (Otto Scharmer and Peter Senge).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, duplication, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the work’s Creative Commons license, unless indicated otherwise in the credit line; if such material is not included in the work’s Creative Commons license and the respective action is not permitted by statutory regulation, users will need to obtain permission from the license holder to duplicate, adapt or reproduce the material.
Copyright information
© 2016 The Author(s)
About this chapter
Cite this chapter
Close, JP., Meeder, N., Schmeitz, J. (2016). The AiREAS Proof of Principle—POP Relating Air Quality to Health and Lifestyle. In: Close, JP. (eds) AiREAS: Sustainocracy for a Healthy City. SpringerBriefs on Case Studies of Sustainable Development. Springer, Cham. https://doi.org/10.1007/978-3-319-45620-1_2
Download citation
DOI: https://doi.org/10.1007/978-3-319-45620-1_2
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-45619-5
Online ISBN: 978-3-319-45620-1
eBook Packages: Earth and Environmental ScienceEarth and Environmental Science (R0)