
Abstract
After hematopoietic stem cell transplant (HSCT), up to 60 % of patients develop pulmonary complications. In spite of antibacterial, antiviral, and antifungal prophylaxis, reduced host defenses render the HSCT patient vulnerable to pulmonary and other infections in the early weeks and even months post-transplantation. This chapter suggests an integrative approach followed by a description of the most common pulmonary syndromes seen in HSCT patients, including diffuse alveolar hemorrhage (DAH), idiopathic pneumonia syndrome (IPS), bronchiolitis obliterans syndrome (BOS), and cryptogenic organizing pneumonia (COP).
The high risk of developing pulmonary complications after HSCT necessitates a pre-transplant pulmonary workup. Pulmonary function tests (PFTs) are done prior to HSCT and include spirometry and diffusion capacity of carbon monoxide (DLCO). Low DLCO and alveolar–arterial oxygen gradient on PFTs carry increased mortality post-HSCT. Decreased DLCO and forced expiratory volume in one second (FEV1) < 80 % are indicators of developing respiratory failure post-HSCT.
Investigating new pulmonary complaints is challenging. All patients should undergo an extensive workup of new pulmonary findings, including dyspnea, cough, fever, and hypoxia. In the first 4–6 weeks post-HSCT, immunocompromised patients can develop bacterial pneumonia. Pathogens include gram-negative rods (Pseudomonas or Klebsiella), Staphylococcus aureus, and Nocardia. While chest X-rays could show typical lobar or multilobar opacities, computed tomography (CT) scan of the chest (noncontrast CT scans are adequate for workup of infectious processes) may yield additional characteristic findings (nodules, ground glass opacities, etc.). Fungal pneumonias, primarily aspergillus, can also develop in this early period. There is a very strong association between invasive Aspergillus pneumonia and neutropenia lasting more than 10 days. Viral pneumonia may develop as well in this patient population; however, it tends to occur later. Cytomegalovirus (CMV) is the most common viral pathogen, but with monitoring and preemptive therapy, the incidence has declined. Other viruses have emerged as pathogens, including respiratory syncytial virus (RSV), influenza, parainfluenza, and human metapneumovirus (see Chap. 17).
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others



Keywords
1 Pulmonary Function Tests
-
1.
Spirometry is used to aid in the diagnosis of obstructive versus restrictive lung disease. Two-year mortality after hematopoietic stem cell transplant (HSCT) has been estimated using a pre-transplantation assessment of mortality (PAM) score which incorporates spirometry and diffusing capacity variables in combination with the presence of renal and hepatic dysfunction, conditioning regimen, and disease risk .
-
a.
Obstructive lung disease is diagnosed with a forced expiratory volume in one second (FEV1)/forced vital capacity (FVC) ratio < 70 % and FEV1 < 80 %. If plethysmography (measurement of changes in lung volumes) is performed, increased residual volume (RV) indicates air trapping as seen in bronchiolitis obliterans syndrome (BOS).
-
b.
Low FVC with normal FEV1/FVC ratio indicates restriction. Lung volumes will help confirm restriction as seen in idiopathic pneumonia syndrome (IPS) or usual interstitial pneumonia. All lung volumes, including RV, will be reduced with restriction.
-
a.
-
2.
DLCO
-
a.
Diffusion capacity of carbon monoxide (DLCO) corrected for hemoglobin should be used (DLCOadj)
-
b.
> 80 % normal, 60–80 % mild, 40–60 % moderate, < 40 % severe impairment
-
a.
2 Bronchoscopy
-
1.
Bronchoalveolar lavage (BAL) via bronchoscopy should be pursued once pneumonia is considered.
-
2.
Pre-procedure stabilization with supplemental oxygen is key.
-
a.
Depressed mental status may increase the risk of the procedure.
-
b.
The presence of severe hypoxia and depressed mental status may require endotracheal intubation to safely perform the procedure.
-
c.
Conscious sedation with fentanyl and/or midazolam is often used for comfort and amnesia.
-
a.
-
3.
Unless there is active bleeding, correction of coagulopathy is not required, and there is no absolute platelet level required for safety with BAL alone.
-
a.
If transbronchial biopsy will be attempted, a pre-procedure platelet count of ≥ 30,000/mm3 and international normalized ratio (INR) of < 1.5 is recommended.
-
a.
-
4.
Complications of bronchoscopy include worsening hypoxemia, airway hemorrhage, and respiratory failure.
-
5.
The risks with transbronchial biopsy are much higher, including pneumothorax, respiratory failure, and difficult to control airway bleeding.
-
6.
Electromagnetic navigational bronchoscopy with BAL and biopsy may improve rates of diagnosis.
-
7.
Appropriately stained BAL smears may suggest a pathogen in a matter of hours while cytology, culture, and genetic results are pending. BAL fluid should routinely be sent for:
-
a.
Cytology, including stains for organisms (fungi, Pneumocystis jiroveci pneumonia (PCP)) and hemosiderin-laden macrophages
-
b.
Bacterial cultures (including Nocardia) and sensitivity
-
c.
Fungal smear and culture
-
d.
Mycobacterium smear and culture
-
e.
Cell count and differential
-
f.
Galactomannan antigen (Aspergillus)
-
g.
Polymerase chain reaction (PCR) for respiratory viral panels
-
h.
PCR for legionella
-
i.
Direct fluorescent antibody (DFA) staining for PCP
-
a.
3 Diffuse Alveolar Hemorrhage
Diffuse alveolar hemorrhage (DAH) is a subset of pulmonary hemorrhage that can develop in up to 5 % of all post-HSCT recipients with mortality rates ranging between 50 and 80 % based on the two largest case series. About 87 % of the cases develop in the first 3 weeks post-HSCT.
-
1.
Risk factors
-
a.
Advanced age
-
b.
Grade 3–4 acute graft-versus-host disease (aGVHD)
-
c.
Allogeneic transplant
-
d.
Pre-HSCT myeloablative conditioning regimen
-
e.
Thrombocytopenia
-
f.
Renal insufficiency
-
g.
Coagulopathy
-
a.
-
2.
Clinical findings
-
a.
Subjective Findings
-
i.
Shortness of breath
-
ii.
Cough
-
iii.
Rarely hemoptysis
-
i.
-
b.
Objective Findings
-
i.
Fever
-
ii.
Tachypnea
-
iii.
Acrocyanosis
-
iv.
Crackles heard on lung auscultation
-
i.
-
a.
-
3.
Diagnostic tests
-
a.
Chest X-ray often shows bilateral diffuse alveolar opacities which could be confirmed by CT scan imaging (Fig. 22.1) as ground glass opacities. These findings are not specific and may be seen in many other conditions.
Fig. 22.1 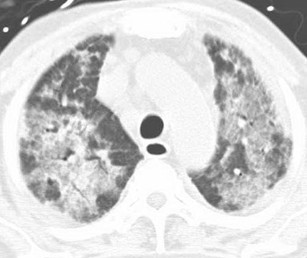
Diffuse ground glass opacities in diffuse alveolar hemorrhage, confirmed by BAL. BAL bronchoalveolar lavage
-
b.
Pulmonary function tests (PFTs) show increased DLCO; however, often these patients cannot participate in such testing.
-
c.
Bronchoscopy with BAL is the confirmatory diagnostic method. BAL shows progressive bloody return. Cytology with Prussian blue staining should show > 20 % hemosiderin-laden macrophages. This test is limited if alveolar hemorrhage occurred < 48–72 h before the procedure, as duration of time may be too short for red blood cells (RBC) phagocytosis by pulmonary macrophages.
-
a.
-
4.
Pathogenesis of DAH
There is no clear etiology for DAH post-HSCT. The development of DAH around the engraftment period suggests an inflammatory cascade involving the alveoli. Pre-HSCT conditioning regimens (including total body irradiation (TBI)) may initiate the inflammatory process.
-
5.
Management
Patients with suspected DAH should be transferred to the medical intensive care unit, given that respiratory failure may develop rapidly. Some patients require high-flow oxygen and subsequent mechanical ventilation for acute respiratory distress syndrome (ARDS). Supportive management and high-dose systemic steroids are the key elements of DAH treatment.
-
a.
Mechanical ventilation should be tailored to each individual, reflecting the ARDS mechanical ventilation protocol/low tidal volume for management of acute lung injury. This practice has not been validated in DAH, but the pathological pattern of DAH is similar to acute lung injury/ARDS. Similarly, prone positioning may be of benefit in refractory cases.
-
b.
Immunosuppressive therapy with high-dose corticosteroids is the mainstay of therapy based on case reports and retrospective series. Doses of up to 1 g of methylprednisolone daily divided into 2–4 doses should be given daily for 3–5 days, followed by a slow taper over 1–3 months. Alternate dosing schedules have been suggested, beginning at 2 mg/kg daily in divided doses, tapering over a 2-month period.
-
c.
Correction of underlying coagulopathy by maintaining platelet count > 50,000/mm3 and INR < 2.
-
d.
BAL to rule out a concomitant infectious pathogen.
-
e.
Recombinant factor VIIa (NovoSeven®) has been used; however, no benefit has been demonstrated.
-
f.
Aminocaproic acid (Amicar®) has been used less frequently with limited supporting data.
-
a.

4 Idiopathic Pneumonia Syndrome
IPS is severe lung injury that develops after allogeneic HSCT with no evidence of an infectious process. The incidence ranges between 2 and 35 % with mortality rates ranging from 60 to 80 %. More recent studies report a lower incidence likely reflecting improved diagnosis of viral infections with newer PCR tests. If mechanical ventilation becomes necessary, mortality approaches 95 %. IPS typically occurs within the first 2 months post-HSCT. However, delayed onset has been reported.
Delayed pulmonary toxicity syndrome (DPTS) is considered distinct from IPS per the American Thoracic Society official statement due to its relationship with a specific conditioning regimen. DPTS occurs in up to 64 % in patients who receive a conditioning regimen containing bis-chloroethylnitrosourea (BCNU), cyclophosphamide, and cisplatin.
-
1.
Risk factors
-
a.
Grade 3–4 aGVHD
-
b.
Donor cytomegalovirus (CMV) positivity
-
c.
Conditioning regimens containing TBI
-
d.
Older age
-
e.
Certain malignancies (acute leukemia, myelodysplastic syndrome)
-
f.
Drug toxicity has been implicated; however, there is no method to discriminate between drug-induced lung damage and IPS.
-
a.
-
2.
Clinical findings
Findings are indistinguishable from pneumonia which include fever, cough usually productive of scant or no phlegm, shortness of breath, and hypoxia.
-
3.
Diagnostic tests
All patients with suspected IPS should undergo chest imaging and bronchoscopy with BAL to rule out infection. Occasionally, chest X-ray does not show obvious infiltrates and CT scan of the chest is warranted. The criteria for diagnosis of IPS proposed by the National Heart Lung and Blood Institute in 1993 include:
-
a.
Radiologic imaging evidence of multilobar diffuse alveolar infiltrates.
-
b.
Hypoxia or elevated alveolar–arterial gradient.
-
c.
Negative BAL for blood and cultures for bacterial, fungal, and viral pathogens.
-
d.
Negative infectious studies from the blood, specifically for CMV.
-
a.
-
4.
Pathogenesis of IPS
Evaluation of BAL fluid from IPS patients shows elevated inflammatory cytokine markers compared to negative or healthy controls. IPS is likely a complex cytotoxic and immune-mediated attack of the lung.
-
5.
Management
-
a.
Corticosteroids should be started early in the disease course. Historically, patients who developed IPS around engraftment responded better to steroids. A reasonable starting dose is 2 mg/kg daily of methylprednisolone (or equivalent) for the first week followed by a slow taper over the course of 2–3 months.
-
b.
PCP and fungal prophylaxis are recommended.
-
c.
Etanercept (Enbrel®) 25 mg SQ twice weekly for 8 weeks has been used in conjunction with corticosteroids; however in small case series, no additional benefit was seen when compared with placebo.
-
a.
5 Bronchiolitis Obliterans Syndrome
The most common late pulmonary complication following allogeneic HSCT is BOS . The reported incidence varies from 2 to 6 % with estimate as high as 20 %. However, recent studies suggest the incidence is more prevalent than previously reported. The median time to onset is 1 year post-HSCT. However, the onset varies from 3 months to > 10 years post-HSCT. BOS is rarely reported after autologous HSCT or umbilical cord blood HSCT. Most investigators consider BOS to be GVHD of the lung. It is also important to recognize BOS as a separate clinical entity from cryptogenic organizing pneumonia (COP) .
-
1.
Risk factors reported by the Center for International Blood and Marrow Transplant Research (CIBMTR) include:
-
a.
Blood-derived stem cells
-
b.
Busulfan-based conditioning regimen
-
c.
Degree of human leukocyte antigen (HLA) mismatch
-
d.
Presence of gastroesophageal reflux
-
e.
Prior interstitial pneumonitis
-
f.
An episode of grade 3–4 aGVHD
-
a.
-
Additional risk factors include:
-
a.
Personal tobacco use
-
b.
Older age
-
c.
Preexisting airflow obstruction
-
d.
Previous respiratory viral infection (CMV, respiratory syncytial virus (RSV), or parainfluenzae)
-
e.
Immunoglobulin G (IgG) level < 400 results in a two- to threefold risk of developing BOS
-
a.
-
2.
Definition
The National Institutes of Health (NIH) diagnosis and staging working group prepared a consensus definition for BOS to provide uniform inclusion criteria for future studies. To make the diagnosis of BOS, these four criteria must be present along with active chronic GVHD in at least one organ other than the lung:
-
a.
FEV1 < 75 % of predicted normal
-
b.
Evidence of airway obstruction with a ratio of FEV1/FVC < 0.7
-
c.
Expiratory high-resolution chest CT that reveals air trapping, small airway thickening, or bronchiectasis or RV > 120 % of predicted normal
-
d.
Absence of active infection or pathologic confirmation
-
i.
Lung biopsy typically shows cicatricial bronchial obliterans (i.e., obliteration of airways by dense fibrous scar tissues)
-
i.
-
a.
-
3.
Clinical findings
Insidious course manifested by nonproductive cough, wheezing, and dyspnea. Early in BOS, pulmonary exam may be normal; however, later stages are manifested by wheezing, prolonged expiratory phase, and inspiratory crackles.
-
4.
Diagnostic tests
-
a.
Chest imaging should be carried out in all patients undergoing workup for BOS. Chest X-rays may be normal early in BOS. As the disease progresses, hyperinflation may be present.
-
b.
High-resolution CT (HRCT) of the chest is more specific (see Fig. 22.2). Inspiratory and expiratory phases should be included to evaluate for air trapping or “mosaic lung appearance” which indicates regional airflow obstruction during the expiratory phase.
Fig. 22.2 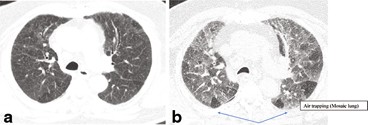
a Inspiratory CT scan of the chest. b Expiratory phase CT scan chest in a patient with BOS. CT computed tomography, BOS bronchiolitis obliterans syndrome
-
c.
PFTs are obtained as part of every patient’s pre-HSCT baseline evaluation.
-
i.
The definition of airflow obstruction includes FEV1 < 75 %, FEV1/FVC < 0.70, or a decline in FEV1 > 10 % in 1 year.
-
ii.
Also noted is air trapping or increased RV and RV to total lung capacity (RV:TLC) ratio.
-
iii.
DLCO is not expected to be reduced but is often low pre-transplant and/or after induction chemotherapy .
-
i.
-
d.
Bronchoscopy is not routinely performed during the workup of BOS unless imaging is suspicious for an infectious process.
-
e.
Transbronchial biopsy is often nondiagnostic as the disease process is patchy.
-
f.
Surgical lung biopsy has higher chance of demonstrating constrictive bronchiolitis, the pathology seen in BOS.
-
i.
With the introduction of HRCT, surgical lung biopsy is often not required to confirm a diagnosis of BOS.
-
i.
-
a.
-
5.
Pathogenesis of BOS
BOS may be a manifestation of primarily chronic GVHD with the etiology related to recognition of disparate antigens present in the context of HLA class I and class II major histocompatibility complex (MHC) molecules. It begins with fibroproliferative disease of the small airways, which results in inflammation, epithelial metaplasia, and denudification. Submucosal/mucosal fibrosis then develops, resulting in obliteration of the airways. Allogenic inflammatory conditions such as viral infections may also contribute to the development of BOS.
-
6.
Management
Management of BOS mainly involves intensifying immunosuppressive therapy and supportive care. There are no specific recommendations associated with treatment of BOS. The management of BOS mimics that of chronic GVHD.
-
a.
Response to bronchodilators is often minimal but nevertheless should be considered because of presence of airflow obstruction.
-
b.
Corticosteroids 1–1.5 mg/kg prednisone per day for 2–6 weeks, then tapered over 6–12 months if there is a response. This regimen is based on case series and expert opinions.
-
c.
Other immunosuppressive medications maybe effective as steroid-sparing agents, including calcineurin inhibitors . Tacrolimus may reduce the incidence of BOS as compared to cyclosporine.
-
d.
Macrolides have been used post-transplant to prevent BOS. Small case series have reported stabilization of FEV1. Azithromycin 250 mgpo three times each week is a suggested regimen.
-
e.
Leukotrienes have been reported to be elevated in BAL fluid of patients with BOS. Trials of montelukast (Singulair®), a leukotriene inhibitor, are underway.
-
f.
A small phase II trial etanercept (Enbrel®) in patients with subacute lung injury showed improvement in lung function with a 5-year overall survival of 67 %, and 90 % in patients who responded to therapy.
-
g.
Patients should be assessed for oxygen needs using 6-min walk test and/or nocturnal O2 monitor study.
-
h.
Echocardiogram can screen for pulmonary hypertension and left ventricular dysfunction, both accompanied by dyspnea.
-
i.
Lung transplant may be considered for very selected patients with severe respiratory impairment.
-
a.

The management of BOS is complicated and requires a multispecialty approach (bone marrow, pulmonary, and radiology specialists). Prognosis of progressive BOS (> 10 % FEV1 decline per year) is poor. Two-year overall survival has been reported at 45 % with a 5-year survival rate of only 13 %. The majority of patients die of respiratory failure triggered by infection. Attention to dyspnea and early and frequent PFTs may allow for earlier identification of BOS before permanent (fibrotic) airway changes, respiratory insufficiency, and pneumonia occur.
6 Cryptogenic Organizing Pneumonia
COP, previously known as bronchiolitis obliterans organizing pneumonia (BOOP), is a disease process of unknown etiology that differs from BOS in clinical findings, response to treatment, and prognosis. One case series of open-lung biopsies done in patients who underwent HSCT found that COP was the most common inflammatory pathology (52 %) .
-
1.
Risk factors
-
a.
No risk factors have been identified. However, a correlation has been demonstrated between the development of COP and viruses, radiation exposure, connective tissue disease, inhalational drugs (cocaine), amiodarone, and inflammatory bowel disease.
-
a.
-
2.
Clinical findings
-
The presentation of COP is similar to many respiratory disorders; most commonly, dyspnea is accompanied by nonproductive cough and fever. Physical exam is primarily notable for the presence of crackles and the absence of wheezing.
-
3.
Diagnostic tests
-
a.
Chest X-ray may show patchy consolidation with ground glass or nodular infiltrates.
-
b.
CT scan of the chest is typically required to demonstrate areas of bilateral organizing pneumonia and consolidation in subpleural or peribronchial distribution associated with areas of ground glass opacities. Migratory opacities on CT scan chest have been described in 25 % of patients with COP.
-
c.
PFTs typically show a restrictive pattern with decreased FVC, FEV1/FVC >70%, and decreased DLCO; airflow obstruction (decreased FEV1/FVC) is generally absent.
-
d.
Bronchoscopy with BAL may be helpful in determining the diagnosis. BAL fluid demonstrates lymphocytes with a decreased CD4/CD8 ratio.
-
e.
Lung biopsy, either by transbronchial biopsy or by video-assisted thoracic surgery (VATS), is occasionally required to confirm the diagnosis. Typical pathology shows granulation tissue plugs in the bronchioles and alveolar ducts associated with surrounding chronic interstitial inflammation.
-
a.
-
4.
Management
-
a.
Prognosis of COP is favorable; 80 % of patients can be expected to recover.
-
b.
Bronchoscopy with BAL is often required to rule out infectious processes.
-
c.
Corticosteroids have been used with great efficacy. However, relapses may occur if steroids are tapered too rapidly.
-
a.
Bibliography
Afessa B, Tefferi A, Litzow MR, Krowka MJ, Wylam ME, Peters SG. Diffuse alveolar hemorrhage in hematopoietic stem cell transplant recipients. Am J Respir Crit Care Med. 2002;166:641–5.
Au BKC, Au MA, Chien JW. Bronchiolitis obliterans syndrome epidemiology after allogeneic hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2011;17:1072–8.
Barker AF, Bergeron A, Rom WN, Hertz MI. Obliterative Bronchiolitis. NEJM. 2014;370:1820–28.
Clark J, Hansen J, Hertz M, Parkman R, Jensen L, Peavy H. NHLBI workshop summary. Idiopathic pneumonia syndrome after bone marrow transplantation. Am Rev Resp Diseases. 1993;147:1601–6.
Fukuda T, Hackman RG, Sandmaier B, Boeckh M, Maris M, Maloney D, et al. Risks and outcomes of idiopathic pneumonia syndrome after nonmyeloablative and conventional conditioning regimens for allogeneic hematopoietic stem cell transplantation. Blood. 2003;102:2777–85.
Kotloff RM, Ahya VN, Crawford SW. Pulmonary complications of solid organ and hematopoietic stem cell transplantation. Am J Respir Crit Care Med. 2004;170:22–48.
Majhail NS, Rizzo JD, Lee SJ, Aljurf M, Atsuta Y, Bonfim C, et al. Recommended screening and preventive practices for long-term survivors after hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2012;18:348–71.
Panoskaltsis-Mortari A, Griese M, Madtes DK, Belperio JA, Haddad IY, Folz RJ, et al. An official American Thoracic Society research statement: noninfectious lung injury after hematopoietic stem cell transplantation: idiopathic pneumonia syndrome. Am J Respir Crit Care Med. 2011;183:1262–79.
Parimon T, Au DH, Martin PJ, Chien JW. A risk score for mortality after allogeneic hematopoietic stem cell transplantation. Ann Intern Med. 2006;144:407–14.
Vasu ST, Cavalazzi R, Hirani A, Kane K. Clinical and radiologic distinctions between secondary bronchiolitis obliterans organizing pneumonia and cryptogenic organizing pneumonia. Resp Care. 2009;54:1028–32.
Williams K, Chien JG, Pavletic S. Bronchiolitis obliterans after allogeneic hematopoietic stem cell transplantation. JAMA. 2009;302:306–14.
Yanik GA, Mineishi S, Levine JE, Kitko CL, White ES, Lander Lugt MT, et al. Soluble tumor necrosis factor receptor: Enbrel (etanercept) for subacute pulmonary dysfunction following allogeneic stem cell transplantation. Biol Blood Marrow Transplant. 2012;18:1044–54.
Yanik GA, Horowitz MM, Weisdorf DJ, Logan BR, Ho VT, Soiffere RJ, et al. A randomized double-blind, placebo-controlled trial of soluble tumor necrosis factor receptor: Enbrel (etanercept) for the treatment of idiopathic pneumonia syndrome following allogeneic stem cell transplantation. A Blood and Marrow Transplant Clinical Trials Network (BMT CTN) protocol. Biol Blood Marrow Transplant. 2014;20(6):858–64. doi:10.1016/j.bbmt.2014.02.026.
Yoshihara S, Yanik G, Cooke KR, Mineishi S. Bronchiolitis obliterans syndrome (BOS), bronchiolitis obliterans organizing pneumonia (BOOP), and other late-onset noninfectious pulmonary complications following allogeneic hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2007;13:749–59.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media, LLC
About this chapter
Cite this chapter
Moulton, B., Barker, A. (2015). Pulmonary Complications. In: Maziarz, R., Slater, S. (eds) Blood and Marrow Transplant Handbook. Springer, Cham. https://doi.org/10.1007/978-3-319-13832-9_22
Download citation
DOI: https://doi.org/10.1007/978-3-319-13832-9_22
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-13831-2
Online ISBN: 978-3-319-13832-9
eBook Packages: MedicineMedicine (R0)