
Abstract
In 2008, an estimated 33.4 million individuals worldwide were infected with the human immunodeficiency virus (HIV) [1]. Only a few years ago, infection with HIV almost invariably culminated in the development of the acquired immunodeficiency syndrome (AIDS), characterized by severe depletion of CD4+ lymphocytes leading to derangements predominantly affecting cell-mediated immunity, but affecting humoral immunity as well [2]. In the later stages of AIDS, neutropenia and neutrophil functional deficits were common sequelae of HIV infection, other opportunistic infections, or HIV- or opportunistic infection-related treatment [3]. The care of the HIV-infected patient was palliative in nature, and the possibility that use of filgrastim (rHuG-CSF) might extend survival in late-stage AIDS patients with severe neutropenia or severe opportunistic infections, or might be a treatment for HIV infection itself, was explored [4]. Subsequently, however, the development of protease inhibitors and the widespread adoption of their use in multidrug regimens of highly active antiretroviral therapy (HAART) revolutionized the care of HIV-infected patients, and the number of patients dying from HIV decreased dramatically [5].
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
- Human Immunodeficiency Virus
- Human Immunodeficiency Virus Infection
- Lymphocyte Count
- Absolute Neutrophil Count
- Invasive Aspergillosis
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
In 2008, an estimated 33.4 million individuals worldwide were infected with the human immunodeficiency virus (HIV) [1]. Only a few years ago, infection with HIV almost invariably culminated in the development of the acquired immunodeficiency syndrome (AIDS), characterized by severe depletion of CD4+ lymphocytes leading to derangements predominantly affecting cell-mediated immunity, but affecting humoral immunity as well [2]. In the later stages of AIDS, neutropenia and neutrophil functional deficits were common sequelae of HIV infection, other opportunistic infections, or HIV- or opportunistic infection-related treatment [3]. The care of the HIV-infected patient was palliative in nature, and the possibility that use of filgrastim (rHuG-CSF) might extend survival in late-stage AIDS patients with severe neutropenia or severe opportunistic infections, or might be a treatment for HIV infection itself, was explored [4]. Subsequently, however, the development of protease inhibitors and the widespread adoption of their use in multidrug regimens of highly active antiretroviral therapy (HAART) revolutionized the care of HIV-infected patients, and the number of patients dying from HIV decreased dramatically [5]. Patients with HIV can, with current regimens, achieve prolonged survival with preservation of immunologic function, although patients infected with HIV have shortened lifespans compared with uninfected people [6] secondary to comorbid conditions and increased rates of cardiovascular [7] and oncologic death [8]. However, despite the widespread availability of HAART in the developed world, patients still present with late-stage AIDS and its attendant complications, including neutropenia, because of late diagnosis of HIV [9] or progression of HIV infection due to nonadherence to HAART [10]. Furthermore, patients with HIV face an increased risk of malignancy and the subsequent need to be treated with cytotoxic chemotherapy [11]. Accordingly, filgrastim has continued to play a role in the management of selected patients with HIV.
2 Epidemiology of Neutropenia in HIV-Infected Individuals
From the earliest days of the AIDS pandemic, neutropenia was identified as a consequence of HIV infection. In 1987, an absolute neutrophil count (ANC) of <2.0 × 109/L was reported in 4 of 20 patients with clinically diagnosed AIDS and 15 of 59 with persistent generalized lymphadenopathy [12]. As this report predates the development of antibody testing for HIV, it was not possible to determine whether patients with persistent generalized lymphadenopathy were truly HIV-infected or not. No patient had an ANC <1.0 × 109/L in this report, although the same author had noted an ANC of 0.4 × 109/L in one patient in a case series of homosexual men with neutropenia in 1985 [13].
Neutropenia is primarily a consequence of late-stage AIDS, with the mean CD4+ lymphocyte count during the first episode of neutropenia in one large study being 85 cells/mm3. However, 14% of patients with a neutropenic episode in this study were observed to have a CD4+ lymphocyte count >200 cells/mm3, and one patient’s CD4+ lymphocyte count at the time of neutropenia was 858 cells/mm3 [14]. It is worth noting that several case reports have associated neutropenia with acute HIV infection [15–18]. Since most instances of acute HIV infection are unrecognized [19], the true incidence of neutropenia associated with acute HIV infection remains unknown.
The epidemiology of neutropenia was examined in the Women’s Interagency HIV Study, a prospective cohort study of 2,059 HIV-infected women enrolled in 1994 and 1995. In this cohort, 1,729 women had a documented ANC measured. It was observed that 7% of women were neutropenic at enrollment, which reflected the prevalence of neutropenia in the pre-HAART era, and that 31% of the study cohort experienced at least one episode of neutropenia (defined as a measured ANC <1.0 × 109/L) during the study. Low CD4+ lymphocyte count and high viral load, suggestive of progression of disease, were associated with the development of neutropenia [20].
Neutropenia is often multifactorial in AIDS patients, with HIV itself, myelosuppressive drugs, opportunistic infections, and malignancy most frequently identified as the etiology. Although zidovudine is the most common antiretroviral associated with neutropenia, other nucleoside reverse transcriptase inhibitors have been implicated in drug-induced neutropenia as well [21]. Indinavir-induced neutropenia has been reported [22], as has neutropenia exacerbated by efavirenz [23]. Noteworthy also are case reports of patients receiving chemotherapy concomitantly with antiretroviral regimens containing ritonavir, a potent inhibitor of the CYP450 system, and subsequently developing neutropenia due to increased concentrations of chemotherapeutic agents [24–26]. Other prophylactic agents including dapsone [27], antifungals, and beta-lactam antibiotics [28] have also been reported to cause neutropenia. Disseminated infections with bone marrow involvement caused by fungal (e.g., endemic mycoses, cryptococcosis) [29], mycobacterial (e.g., tuberculosis or Mycobacterium avium complex), protozoal (e.g., leishmaniasis), or viral (e.g., cytomegaloviral) pathogens have been identified as contributors to HIV-associated neutropenia [30]. Finally, infiltration of bone marrow with lymphoma is not infrequently a cause of HIV-associated neutropenia [31], and this possibility should be considered before ascribing neutropenia to medications alone.
The proportion of neutropenic episodes attributable to each of the above causes depends on the patient population. In one Italian study including 81 neutropenic patients in the pre-HAART era, most of whom were intravenous drug users, neutropenia was attributed to HIV itself in 18.5% of the patients, to infiltration of bone marrow with lymphoma or infection in 24.6% of patients, and drugs in 56.7%. Of patients with drug-induced neutropenia, zidovudine was a contributor to 48.2% of cases, chemotherapy to 21.3% of cases, trimethoprim-sulfamethoxazole to 18.7%, amphotericin B to 17.5%, ganciclovir to 13.6%, pyrimethamine to 11.1%, and dapsone to 6.4% of cases [32]. In a different study, zidovudine therapy was a contributing factor to neutropenia in 51% of patients, trimethoprim–sulphamethoxazole treatment in 45% of patients, ganciclovir therapy in 18% of patients, and cytotoxic chemotherapy in 11.3% of patients; neutropenia was attributed to lymphoma in 6.5% of cases and HIV infection itself in 1.6% of patients [31].
The epidemiology of neutropenia in HIV patients has drastically changed with the advent of HAART. HAART prevents progression of HIV, and was found to prevent the development of neutropenia in the Women’s Interagency HIV study cohort [20]. Furthermore, HAART itself is an effective long-term treatment for HIV-associated neutropenia [33, 34]. In addition, the decreased dose of zidovudine employed as part of HAART regimens may be less likely to cause neutropenia than the higher dose used in the pre-HAART era. One study where patients were routinely converted from stavudine to zidovudine after 6 months of HAART therapy reported that only 7.7% of patients developed an ANC <0.75 × 109/L [33], and a similar conversion study of 78 HIV-infected children reported that only 6% developed an ANC <1.0 × 109/L. In the latter study, no individual’s ANC decreased to <0.75 × 109/L [34].
3 Impaired Neutrophil Function in HIV Infection
In addition to neutropenia, there are functional defects of neutrophils, as well as monocytes and macrophages, in HIV infection and other lentivirus infections. These defects are not unique to HIV infection, and a number of viral infections have been associated with impaired neutrophil function [35]. A wide range of functional defects exist, including defects in chemotaxis, phagocytosis, the respiratory (oxidative) burst, and microbicidal capacity [36–41]. Neutrophils isolated from HIV-infected patients have a profound defect in chemotaxis in response to interleukin (IL)-8 and bacterial chemoattractant peptides, such as f-met-leu-phe (fMLP), and the degree of impairment correlates with the degree of CD4+ T-cell depletion. Other physiologic functions related to recruitment to sites of infection, rolling, adhesion, and emigration are also affected, as shown in a feline leukemia virus (FIV) infection model. Evidence that this may be due to a maturation defect is decreased granularity of neutrophils from the blood and bone marrow of FIV-infected animals. The results of different studies of neutrophil function in HIV infection are at times conflicting and can be explained by different assays, different conditions, and differences in the patient populations studied. The most important clinical variable is the stage of HIV disease as evidenced by absolute CD4+ T-cell count.
The respiratory burst is a very important part of the microbial killing by neutrophils, generating superoxide and other bactericidal reactive oxygen species. Our group previously examined the neutrophil respiratory burst by chemiluminescence in a cohort of 78 patients with HIV infection at different stages of disease [42]. Patients with HIV infection had altered oxidative metabolism in response to opsonin receptor-dependent stimulation with zymosan opsonized with purified human complement (C3bi) or immune globulin (IgG). Patients with early HIV infection with CD4+ lymphocyte counts >500 cells/mm3 exhibited increased neutrophil chemiluminescence in response to opsonized zymosan compared with controls, while patients with advanced disease with low CD4+ lymphocyte counts showed significantly decreased chemiluminescence. Absolute CD4+ lymphocyte count was the only patient variable significantly correlated with opsonin-dependent neutrophil chemiluminscence activity according to multiple regression analysis. Despite a good correlation between ANC and CD4+ lymphocyte count (R = 0.24; p = 0.04), ANC was not an independent predictor of impaired neutrophil chemiluminescence by multiple regression analysis.
4 Pathogenesis of Neutropenia and Neutrophil Dysfunction
The pathophysiology of neutropenia and neutrophil dysfunction in HIV infection unrelated to drug therapy or secondary complications has been better elucidated in the past few years. A subset of neutropenic HIV-infected patients may have autoimmune neutropenia; however, this probably accounts for a small proportion of cases of neutropenia [13, 43]. A study of neutropenic children with HIV infection showed that while many children had circulating antineutrophil antibodies, the presence of these antibodies did not correlate with the ANC [44].
The various immune abnormalities observed in HIV infection occur in the setting of immune systemic activation. There has been considerable interest in immune system activation occurring as a result of T-cell depletion in gut-associated lymphoid tissue (GALT) with loss of mucosal barrier function, which results in translocation of lipopolysaccharide (LPS) and other bacterial products that activate the immune system [45]. A number of investigators have shown that neutrophils are activated in vivo throughout the course of HIV infection, even in the absence of any clinical signs of secondary infectious complications [46]. Early in the course of HIV infection in vivo, activation or priming may actually result in enhanced function. This in vivo activation continues throughout the course of HIV infection, but eventually the functional capacity of the neutrophil begins to decrease significantly. It should also be noted that immune system activation has been proposed as a mechanism for impaired neutrophil function in patients with chronic hepatitis B infection [47].
Our studies of neutrophil chemiluminescence suggest that immune system activation may contribute to neutrophil dysfunction [42]. Maximum opsonin receptor expression (MOR) is achieved by exposing neutrophil to quantities of proinflammatory mediators (primers: fMLP, complement fragment C5a, and platelet-activating factor) to induce a maximal number of CD11b (C3bi receptor) and CD35 (C3b receptor or complement receptor 1) on the neutrophil surface. Priming may also enhance oxidative responses to a second stimulus by increasing the affinity of opsonin receptors for their particular ligand or enhancing intracellular signaling. Our experiments showed increases in the ratio of the chemiluminescence unprimed neutrophil at circulating opsonin receptor expression (COR) to chemiluminescence with MOR, i.e., an increased COR/MOR ratio. By whatever mechanism, neutrophils from HIV-infected patients behave as if they have been primed or activated by proinflammatory mediators in vivo. Opsonin receptor-independent NADPH-oxidase and myeloperoxidase activities, basal and stimulated, were significantly increased for HIV-infected patients, especially those with advanced disease with CD4+ lymphocyte count <200 cells/mm3. The increase in enzyme activities of NADPH-oxidase and myeloperoxidase may also be the result of in vivo activation. The decrease in myeloperoxidase activity for patients with very advanced HIV infection with CD4+ lymphocyte count <100 cells/mm3, although significantly higher than values seen in control subjects without HIV infection, may be due to degranulation resulting from in vivo activation. This chronic in vivo activation may lead to metabolic exhaustion or “burnout,” and contributes to impaired neutrophil oxidative responses in HIV-infected patients at advanced stages of disease.
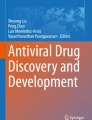
In vivo activation is not the only process that contributes to neutrophil dysfunction in HIV infection. Neutrophils isolated from patients with advanced HIV disease undergo accelerated apoptosis or programmed cell death. We studied apoptosis of neutrophils isolated from ten individuals with advanced HIV infection and seven control subjects [48]. Ex vivo apoptosis was examined morphologically by fluorescent microscopy after dual staining with acridine orange and ethidium bromide, fluorescent stains that intercalate DNA. Acridine orange stains the nucleus bright green and allows visualization of the nuclear chromatin pattern, while ethidium bromide identifies nonviable cells by staining the nucleus orange. Little apoptosis was evident immediately after isolation, but over time, apoptosis was observed and the proportion of apoptotic cells was significantly higher for the patients with advanced HIV infection at 3, 6, and 18 h (Fig. 1). Apoptotic cells eventually die, and at 18 h there was a significant decrease in viability for the HIV patient’s neutrophils due to an increased number of nonviable, apoptotic cells. As neutrophils become apoptotic, they become functionally impaired, and the accelerated apoptosis of neutrophils may in part explain the impairment of neutrophil function seen in this patient population, as well as neutropenia. A number of possible mechanisms for accelerated apoptosis exist, including increased levels of proinflammatory mediators that may accelerate the process. Other mechanisms may also be involved, including direct effects of viral proteins. HIV protease can directly induce apoptosis of a variety of leukocyte populations [49]. Alternatively, growth factor deficiency could result in accelerated apoptosis.

Neutrophil apoptosis and viability in patients with AIDS compared with normal controls
Granulocyte precursors can be infected by HIV, and this may affect normal proliferation and development of neutrophils, but mature cells are not targets and express very little, if any, HIV [50]. Infection of bone marrow stromal cells may affect the microenvironment for myelopoiesis. Both HIV and cytomegalovirus (CMV) can infect bone marrow stromal cells and impair production of endogenous colony-stimulating factors such as granulocyte colony-stimulating factor (G-CSF) and granulocyte-macrophage colony-stimulating factor (GM-CSF) [51, 52]. Altered cytokine secretion may result in abnormal neutrophil maturation. G-CSF is a key growth factor important in maintaining the normal number of circulating neutrophils. Although several growth factors can stimulate myelopoiesis, studies of G-CSF-deficient knock-out mice indicate G-CSF is a cytokine necessary to maintain normal neutrophil counts [53]. Evidence is accumulating that HIV infection results in a state of endogenous G-CSF deficiency [54, 55]. Patients with HIV have lower serum levels of endogenous G-CSF for a given degree of neutropenia compared with patients with neutropenia from other etiologies, such as aplastic anemia and cancer chemotherapy. The low levels of G-CSF may not only impair myelopoiesis and affect neutrophil maturation, but also reduce the circulating half-life of neutrophils. The principle way growth factors cause clonal expansion of different bone marrow precursors is by inhibiting apoptosis of these cells [56]. Our data show that accelerated neutrophil apoptosis in HIV infection is reversible in vitro and ex vivo in patients receiving filgrastim [48, 57].
Why should a decrease in growth factor(s) required for neutrophil maturation occur in a disease characterized by abnormal cell-mediated immunity? The source of G-CSF, directly or indirectly, is activated T-cells, monocytes, and macrophages, all targets for HIV infection. Depletion or dysfunction of these cells as a result of HIV infection may result in decreased production of G-CSF that is required to support normal granulopoiesis and/or neutrophilic responses to infection. We previously reported that peripheral blood mononuclear cells (PBMC) isolated from patients with AIDS produce significantly less G-CSF in response to a challenge with LPS [54]. Local G-CSF production by bone marrow stromal cells is likely to be very important in granulopoiesis, and there is a decreased G-CSF response by bone marrow stromal cells from patients with HIV infection ex vivo in response to IL-1 and LPS [51].
More is known about how CD4+ T-helper cells recruit and activate a wide variety of cell types, including macrophages, mast cells, neutrophils, eosinophils, and basophils, in addition to adaptive immune effector cells. Several different types of CD4+ T-cells have been described that differentiate from naïve CD4+ T-cells [55]. In addition to Th1 and Th2 cells, we now recognize regulatory T-cells (Treg) [58]. These cells not only are involved in immunosuppression, but also can differentiate into effector T-cells. More has also been discovered about the interactions between phagocytic cells and T-cells. The Th17 pathway has been characterized [59]. Th17 cells have been classified as a new lineage, distinct from Th1, Th2, and Treg cells. T17 cells develop as a result of a unique set of cytokines secreted by effector cells of the innate immune system (e.g., neutrophils) and additive effects of IL-1β and tumor-necrosis factor (TNF)-α. Transforming growth factor (TGF)-β and IL-6 are crucial factors in the generation of Th17 cells from naive T-cells. The functional capacity of Th17 cells depends on the additional cytokines IL-23 and IL-1.
Th17 cells are characterized by production of the proinflammatory cytokines IL-17A, IL-17F, IL-22, and IL-26. The activity of IL-17A and IL-17F is defined by induction of increased production of a number of proinflammatory mediators, including IL-1, IL-6, CXC chemokines, TNF-α, G-CSF, and GM-CSF by epithelial and endothelial cells, macrophages, and other stromal cells. IL-17A also promotes stem-cell factor (SCF)- and G-CSF-mediated granulopoiesis [60]. It has been controversial as to whether or not neutrophils directly respond to IL-17A or IL-17F, but the downstream production of cytokines induced by IL-17A and IL-17F leads to granulopoiesis, neutrophil recruitment, and neutrophil activation. Substantial evidence exists of cross-talk between neutrophils and Th17 CD4+ T-cells [61]. Purified human neutrophils produce chemokines that attract Th1 and Th17 cells, while Th17 cells produce CXCL8, a potent chemoattractant for neutrophils.
Th17 cells are important in host defense against infections caused by both intracellular pathogens, such as listeriosis, salmonellosis, cryptococcosis, leishmaniasis, and tularemia, and a variety of extracellular bacterial and fungal pathogens. The role of Th17 cells in specific infections is not completely understood and, in some infections such as invasive aspergillosis, the data are conflicting. It appears, however, that Th17 cells are very important for mucosal host defense against oral candidiasis, mainly through the recruitment of neutrophils, and may also be important in disseminated disease [62]. Th17 cells are also involved in the response to Staphylococcus aureus infection [63].
Th17 cells express CD4, so it is not surprising that dysfunction and depletion of Th17 cells occur in HIV infection. Th17 cells are efficiently infected by HIV-1 in vitro [64], which may help explain the broad range of bacterial and fungal pathogens, particularly extracellular pathogens, that infect patients with HIV. CD4+IL-17+ populations are greatly reduced in antiretroviral-naive HIV-infected patients compared to HIV-negative controls, but this subset is greatly increased after the initiation of HAART, while IFN-α T-cells (Th1) are unchanged [65]. Depletion of Th17 cells in the gut has been associated with decreased microbial barrier function of the gut and persistent immune activation due to gut translocation [66]. Other studies have even shown a decrease in TH17 cells and the Th17:Th1 ratio with preferential depletion of Th17 cells from GALT within weeks of simian immunodeficiency virus (SIV) infection in macaques [67].
The cross-talk between Th17 cells and neutrophils and other phagocytic cells of the innate immune system may explain previous observations that rHuG-CSF may be of potential benefit for immune reconstitution in HIV infection. Previously, our group was part of a study that demonstrated that rHuG-CSF can restore IL-2 production in the blood of HIV-infected individuals [68]. At that time, it was unknown how rHuG-CSF affected T-cell function or production of a lymphocyte growth factor. In retrospect, neutrophil activation may lead to IL-6 release, subsequent Th17 differentiation, and IL-17 production. An inverse relationship exists between Treg and Th17 cells, so an increase in Th17-inducing cytokines may lead to a decrease in Tregs that mediate immunosuppression. Furthermore, T-cells are not only the source but also the target of IL-17. IL-17 can modulate Th1 cell polarization both in vitro and in vivo by directly acting on CD4+ T-cells [69]. Overall, however, the effects of rHuG-CSF on CD4+ lymphocyte counts have been variable [70, 71].
5 Risk of Infections in HIV-Induced Neutropenia
Initial reports in the pre-HAART era suggested that the risk of infection in patients with HIV-associated neutropenia was less than the risk of infection in patients with neutropenia due to chemotherapy or hematologic malignancy, a fact attributed to, among other factors, the lack of mucosal injury in neutropenia not due to cytotoxic chemotherapy and the relatively mild nature of HIV-associated neutropenia compared to neutropenia associated with hematologic malignancy or cytotoxic chemotherapy. Farber et al., in one of the first studies to examine the risk of infection, retrospectively examined the records of 30 HIV-infected patients with ANC <1.0 × 109/L and CD4+ lymphocyte count <200 cells/mm3, comparing infection rates during neutropenic periods and non-neutropenic periods and comparing infection rates in these patients with 37 patients with hematologic malignancies as controls. In that study, no difference was found between infection rates in HIV patients during neutropenic periods compared with non-neutropenic periods [72]. Piliero et al., in reviewing blood culture data from 38 HIV-infected patients with ANC <0.5 × 109/L and 1,071 non-neutropenic HIV patients, found that the presence of a central venous catheter, but not neutropenia, was a risk factor for positive blood cultures in a multiple logistic regression model [73].
A number of subsequent studies, however, have suggested that HIV-associated neutropenia is associated with an increased risk of infection. Shaunik and Bartlett, in an era when zidovudine monotherapy dosed at 1,200 mg/day was the standard of care for HIV treatment (compared with the dose of 600 mg/day used in current HAART regimens), found in a study of 30 patients that an ANC <0.5 × 109/L was associated with an incidence of bacterial infection that was 600% higher than the incidence observed when ANC was >1.0 × 109/L [74]. Keizer et al. performed a case–control study comparing 29 HIV-infected patients followed from 1991 to 1993 with two consecutive measured ANC <1.0 × 109/L with 29 HIV-infected controls without history of neutropenia matched for age, sex, CD4+ lymphocyte count, and month of entry into the clinic. An incidence of 12.6 episodes of bacteremia per 100 patient-months was observed in the patients with a history of neutropenia compared with an incidence of 0.87 episodes of bacteremia per 100 patient-months observed in the controls, a statistically significant difference (p = 0.0027). In a multiple logistic regression model, neutropenia (OR = 22.7) and the presence of a central venous catheter (OR = 8.5) were independent predictors of the development of bacteremia [75]. Hambleton et al. compared the outcomes of HIV-infected inpatients who developed neutropenia after treatment with cytotoxic chemotherapy and those who developed neutropenia for other reasons from 1987 to 1990. In their cohort, few patients received filgrastim, and most patients were white men who had sex with men. They found no statistically significant difference in the rates of bacteremia or mortality between the two groups in both bivariate analysis and in multiple logistic regression models [70]. At the same center, but examining a different time period (1992–1993), Jacobsen et al. examined the rates of hospitalization for HIV-infected outpatients stratified by ANC, using ICD-9 codes to evaluate for the presence of infection. A total of 2047 outpatients were analyzed for this study. A progressive and statistically significant increase in the risk of hospitalization was noted as the nadir ANC decreased. The number of days hospitalized per 10,000 days of risk increased from 61 for patients whose ANC was always >0.5 × 109/L during the study period to 487 for patients with ANC nadir <0.3 × 109/L [71].
Moore et al. performed a case–control study of patients followed from 1990 to 1994; 118 HIV-infected patients with a measured ANC <1.0 × 109/L were matched with HIV-infected non-neutropenic controls on the basis of history of intravenous drug use, CD4+ lymphocyte count, enrollment date in the clinic, and duration of follow-up. A statistically significant association between neutropenia and the development of a bacterial infection was observed. In an adjusted analysis, the relative risk for developing a bacterial infection was 2.33 times higher in patients with an ANC <1.0 × 109/L, and 7.92 times higher for patients with an ANC <0.5 × 109/L, compared with patients with an ANC >1.0 × 109/L; the incidence of bacterial infections was estimated as 3.5–4.5 per 100 patient-months of neutropenia [76].
Eng et al. performed a retrospective cohort study examining the records of patients who received HIV care from 1990 to 1992. Of 930 patients, 85 experienced at least one episode of neutropenia, and of 12 patients with “severe” neutropenia (ANC <0.3 × 109/L), 3 experienced gram-negative bacteremia, compared with four episodes of gram-negative bacteremia in 61 patients with less severe neutropenia [77].
Subsequently, Caperna et al. performed a retrospective cohort study examining patients who had at least two ANC measurements between 1991 and 1995. As the degree of neutropenia worsened, increases in the observed incidence of bacteremia with Escherichia coli, Pseudomonas aeruginosa, and Klebsiella pneumoniae were noted in this cohort of 1,645 patients [78]. A subsequent nested case–control study from the same cohort during the same time interval concluded that, adjusting for CD4+ lymphocyte count, clinical stage of HIV infection, and other confounders, a measured ANC <0.5 × 109/L conferred an eightfold increased risk of bacteremia with one of the three aforementioned pathogens [79].
Tumbarello et al. retrospectively examined 9 years of patient records from a single center in Italy, comparing HIV-infected patients with bacteremia with both HIV nonbacteremic and HIV-uninfected bacteremic controls. In a multivariate analysis of HIV-infected patients, most of whom were intravenous drug users, low CD4+ lymphocyte count, presence of a central venous catheter, and ANC <1.0 × 109/L (OR 3.05; p = 0.04) were independent risk factors for the development of bacteremia [32].
Hermans et al., from a cohort of 1,870 HIV-infected patients seen at a Belgian HIV care center from 1982 to 1993, found 1,403 whose ANC had been measured at least once. From this sample, they identified 484 patients with episodes of neutropenia, defined in this study as a measured ANC <1.0 × 109/L. A history of neutropenia was associated with bacteremia or bacterial pneumonia. Subsequently, 177 neutropenic patients from this cohort were compared with 177 non-neutropenic controls matched for initial CD4+ lymphocyte count and duration of follow-up. Although, in unadjusted analysis, neutropenia was associated with increased odds of developing infection (OR 3.29), this association disappeared in a multiple logistic regression model which also included clinical stage of AIDS and hemoglobin concentration [80].
Meynard et al. performed a single-institution prospective study that enrolled 62 HIV-infected patients with a measured ANC <1.0 × 109/L. In their study, a higher risk of infection was noted in neutropenic patients with malignancy compared with other neutropenic patients, and logistic regression modeling identified a history of neutropenia, the presence of a central venous catheter, and trough ANC as independent predictors of developing an infection [31].
Moore et al. retrospectively identified 328 HIV-infected individuals at their center in the United Kingdom with an ANC <1.0 × 109/L from 1994 to 1995, excluding 78 patients receiving cytotoxic chemotherapy. Bacteremias were documented in 21% of patients and were observed more commonly in patients with brief, profound neutropenias, rather than in patients with milder but more prolonged neutropenic episodes, and the degree of neutropenia correlated with the risk of infection [14]. A subsequent prospective study at the same center enrolled 87 patients in 1996 and 1997. No patients were receiving chemotherapy. Upon enrollment in the study, blood was sampled weekly to measure the duration of neutropenia. Filgrastim was only given for documented infection. The median duration of neutropenia was 13 days. Twelve subjects (17%) were diagnosed with neutropenia-associated infection, in whom six were found to have infection serious enough to warrant filgrastim therapy, and four required hospital admission. All serious infections occurred in patients with ANC <0.5 × 109/L. A further four patients received filgrastim due to prolonged neutropenia [81].
Most of the studies on the risk of infection in neutropenia were conducted in the pre-HAART era. Relatively fewer studies have attempted to assess the link between neutropenia and infection after the widespread implementation of HAART. In the Women’s Interagency HIV study, which began in the pre-HAART era but extended through the development of HAART, it was observed that, independent of CD4+ lymphocyte count and viral load, which were strong predictors of mortality, the presence or absence of neutropenia was not predictive of mortality [20].
Toure et al., in examining the incidence of neutropenia in a prospective cohort of 533 African patients over 6 years taking trimethoprim–sulfamethoxazole prophylaxis in a setting where HAART was available if indicated, found that 36% of patients had at least one measured ANC <1.0 × 109/L during the study, that developing neutropenia was associated with low initial CD4+ lymphocyte count, and that the adjusted hazard ratio of developing bacterial morbidity was 1.50 for patients with a history of neutropenia to that degree, but the overall likelihood of bacterial morbidity was low (36 patients overall) [82].
Most of the preceding discussion has focused on bacterial infections. In patients with hematologic malignancy or in patients undergoing stem cell transplantation, invasive aspergillosis is a feared complication of the prolonged neutropenia that these patients experience [83]. Case reports and case series have noted the occurrence of aspergillosis in patients with advanced HIV [84]; however, aspergillosis as a complication of neutropenia was an uncommon event in HIV-infected patients even before the advent of HAART [85]. Case series suggest that neutropenia or steroid use may predispose to invasive aspergillosis in HIV-infected patients [86, 87]. Mylonakis et al. reviewed 342 reported cases of aspergillosis in HIV-infected patients obtained by MEDLINE and AIDSLINE searches through 1997, and found that 93 patients were diagnosed with “definite” invasive aspergillosis, of whom 16 were reported to have an ANC <0.5 × 109/L [88].
6 The Use of Filgrastim in Nonmalignant Conditions in HIV Infection
Since the beginning of the HIV epidemic, several dozen case reports, case series, and clinical trials have described the use of filgrastim and other formulations of rHuG-CSF in HIV-infected individuals without malignancy and have described outcomes (summarized in Table 1). Kimura et al. were the first to publish their experience, reporting on the use of rHuG-CSF in 14 Japanese patients, 11 of whom were neutropenic. The patient cohort primarily consisted of 12 patients with hemophilia, eight of whom demonstrated concurrent infection at the time of enrollment, and two of whom were experiencing fever of unknown origin. Patients were randomly assigned to receive 100 μg/m2 or 200 μg/m2 rHuG-CSF daily intravenously. The dose was subsequently titrated to maintain the ANC >3.0 × 109/L. A dose-dependent increase in ANC was observed in patients not receiving zidovudine, and escalation of rHuG-CSF dosage prevented the development of neutropenia in patients receiving zidovudine [89].
Miles published the first reports specifically evaluating the benefit of filgrastim in neutropenic patients with HIV. In the first report, 13 patients were selected to receive filgrastim, which was initially dosed at 3 μg/kg daily with subsequent dose escalation until ANC >6.0 × 109/L. Once an adequate dose was established, it was maintained for 2 weeks; rHuEPO was subsequently given. Of the 13 patients selected, 1 died and 1 was removed from the study for noncompliance. In the other 11 patients, filgrastim therapy alone was associated with an increase in BFU-E (burst forming unit-erythron) levels, as well as a statistically significant mean hemoglobin increase of 1.04 g/dL [90]. Patients were then given zidovudine, dosed at either 1,000 or 1,500 mg/day. In the full analysis based on 22 recruited patients, 20 of whom were included in the final analysis, growth factors ensured that no patient needed to discontinue zidovudine therapy secondary to neutropenia, although eight patients developed transfusion dependence necessitating cessation of therapy [91].
Bratt et al. were among the first to describe long-term outcomes from rHuG-CSF therapy, noting in their series of 17 patients that appropriate white blood cell counts could be maintained for up to 7 months in patients with initial counts <1.0 × 109/L [92]. Several small case series and small pilot studies were published in the ensuing years, but a pair of studies notable due to their size are the retrospective cohort studies reported by Grutzmeier and colleagues in 1996, reflecting treatment experience in the pre-HAART era. In one cohort of gay men with CD4+ lymphocyte counts <50 cells/mm3 in Sweden, treatment with rHuG-CSF was initiated upon measuring a white blood cell count <1.0 × 109/L or ANC <0.5 × 109/L. Median survival in the 60 patients who received rHuG-CSF was 658 days, compared with a median survival of 511 days in the 104 patients who did not receive rHuG-CSF (p < 0.01). A similar analysis by the same authors performed on data from a similar cohort in Denmark found that the 60 patients who had received rHuG-CSF lived for a median of 248 days, compared with a median survival of 145 days in the 65 patients who did not receive rHuG-CSF [93].
Also notable for both its size and its prospective nature is the multicenter trial conducted by the G-CSF 92105 group and published in 1996. Patients were eligible if, on at least three occasions within a 2-week period, their measured ANC was found to be <1.0 × 109/L. Filgrastim dose was titrated to maintain ANC >2.0 × 109/L, a target obtained in 98% of patients. Patients received filgrastim for at least 28 days, but could receive it for a longer duration at the discretion of their physicians. The number of patients receiving what were considered to be the drugs most associated with neutropenia (zidovudine, trimethoprim-sulfamethoxazole, ganciclovir, and pyrimethamine) increased 20% over the course of the study [94].
The results of the largest prospective randomized control trial to investigate the outcome of filgrastim administration to neutropenic patients with HIV were published by Kuritzkes et al. in 1998. Of note, patients were accrued in the pre-HAART era. Eligibility requirements for this multicenter, nonblinded study included at least one measured ANC between 0.75 and 1.0 × 109/L, CD4+ lymphocyte count <200 cells/mm3, platelet count >50.0 × 109/L, Karnovsky score >50%, and life expectancy >6 months. Malignancy was the most notable exclusion criterion. In all, 258 patients were randomly assigned to daily, intermittent, or no filgrastim administration for 24 weeks, with filgrastim dose subsequently titrated to maintain white cell count in the 2.0–10.0 × 109/L range. Control patients receiving no filgrastim who developed an ANC <0.5 × 109/L were censored and subsequently re-randomized to one of the two treatment groups, an event which occurred in 18 patients. In all, 34.1% of patients who were assigned to receive no filgrastim developed the primary endpoint of severe neutropenia or death, compared with 12.8% of patients in the intermittent filgrastim group and 8.2% of patients in the daily filgrastim group. Patients who received filgrastim were 54% less likely than controls to develop a serious bacterial infection (p = 0.005) [95].
The most recent large study to examine the effect of filgrastim administration on outcomes in patients with HIV was the retrospective cohort study published by Davidson et al. in 2002. This study was a retrospective analysis of data from several prospectively conducted studies of HIV-infected patients with CMV retinitis. Of note, significant heterogeneity in the use of filgrastim was present in the original trials. In an analysis made complex by the need to correct for the inherent biases of a retrospective analysis, filgrastim use was associated with a 56% reduction in death in a multivariate model (p < 0.01). Associations between filgrastim use and such outcomes as catheter-associated bacteremia and repeat bacterial infection were significant in unadjusted analysis but not after adjustment for confounders [96].
Other interesting uses for rHuG-CSF which single reports have explored include the use of filgrastim as an adjunct to a tagged white blood cell scan in a neutropenic HIV-infected patient in the workup of postoperative fever [97], and the use of filgrastim concomitantly with antimicrobials in the treatment of disseminated mycobacterial infection [98].
7 The Use of Filgrastim in Malignant Conditions in HIV Infection
The benefits of more widespread use of colony-stimulating factors in HIV-negative patients undergoing chemotherapy are now widely accepted, as demonstrated by recently written clinical guidelines which expand the criteria for their use [99]. This change in practice applies to HIV-infected patients as well. Although no randomized trial specifically has addressed the use of filgrastim in HIV-associated malignancy, several nonrandomized comparative studies looking at the benefits of adding rHuG-CSF to a chemotherapy regimen in patients with HIV-associated lymphoma have been published. In a pre- and postintervention trial where 65 HIV-infected patients with non-Hodgkin’s lymphoma (NHL) either received a dose-reduced variant of the CHOP regimen (chemotherapy with cyclophosphamide, doxorubicin, vincristine, and prednisone) or full-dose CHOP augmented by filgrastim, grade 3 or 4 neutropenia occurred in fewer patients receiving full-dose CHOP with filgrastim (13% vs. 25%), a nonsignificant difference. The study was neither intended to nor powered to measure the effect of filgrastim independently [100]. A similar, nonrandomized study by Rossi found that HIV-positive patients receiving rHuG-CSF during chemotherapy were more likely than those who did not to receive full doses of chemotherapy and to receive cycles without delays, although the likelihood of complete response was actually lower in those who received rHuG-CSF [101]. A third study, also nonrandomized, compared the outcomes of HIV-positive patients undergoing chemotherapy for NHL, finding a decrease in mean duration of treatment delays between cycles from 9d to 4d (p = 0.01). Again, however, mean duration of survival was worse in the group receiving rHuG-CSF, which also trended toward having more advanced HIV [102]. Further discussion of the role of rHuG-CSF in HIV-associated malignancies is beyond the scope of this chapter; a review of the use of hematopoietic growth factors in HIV-associated malignancies has been previously published [103].
8 Adverse Effects of Use
The most common side effect of filgrastim is bone pain, with headache, nausea, and vomiting also frequently reported [104]. Although generally safe, filgrastim usage in HIV patients has been associated with disseminated intravascular coagulation [105], hepatitis, and pancreatitis [106]. In non-HIV patients, a review of case reports of adverse effects of filgrastim noted a number of rare adverse events, many of which were attributed to increased inflammation (ARDS, shock, worsening autoimmune disease) or leukostasis (arterial thrombosis or myocardial infarction, interstitial nephritis, bone marrow necrosis) [107].
Nevertheless, the adverse effect of filgrastim that serves as the biggest barrier to its use is its cost. However, filgrastim may be effective in HIV-infected patients at doses lower than those traditionally used for patients with chemotherapy-induced neutropenia [108]. One center developed a clinical pharmacist-driven protocol for dosing filgrastim in HIV-infected inpatients based on ANC; subsequently, the quarterly cost for filgrastim for the HIV service decreased from US$90,000 to US$22,000 [109].
9 Conclusion
The incidence of neutropenia in HIV-infected patients has decreased with the advent of therapies that arrest and reverse the progression of AIDS. In the future, most patients with HIV who develop neutropenia will likely do so from oncologic disease and its treatment, not HIV itself. However, the inability of all HIV-infected patients to benefit from the advances in HIV treatment means that filgrastim will continue to play a role in the management of complications of advanced HIV and its treatment.
References
UNAIDS (2009) AIDS epidemic update: November 2009. UNAIDS, Geneva, Switzerland
Moir S, Chun TW, Fauci AS (2011) Pathogenic mechanisms of HIV disease. Annu Rev Pathol 6:223–248
Israel DS, Plaisance KI (1991) Neutropenia in patients infected with human immunodeficiency virus. Clin Pharm 10:268–279
Pitrak DL (1998) Use of filgrastim (r-metHuG-CSF) in human immunodeficiency virus infection. In: Morstyn G, Dexter TM, Foote M (eds) Filgrastim (r-metHuG-CSF) in clinical practice, 2nd edn. Marcel Dekker, New York, pp 441–468
Palella FJJ, Baker RK, Moorman AC et al (2006) Mortality in the highly active antiretroviral therapy era: changing causes of death and disease in the HIV outpatient study. J Acquir Immune Defic Syndr 43:27–34
Losina E, Schackman Bruce R, Sadownik Sara N et al (2009) Racial and sex disparities in life expectancy losses among HIV-infected persons in the United States: impact of risk behavior, late initiation, and early discontinuation of antiretroviral therapy. Clin Infect Dis 49:1570–1578
Isabella S, Lukas ES, Georg N, Roberto C, Rainer W, Thomas FL (2006) Cardiovascular disease in HIV infection. Am Heart J 151:1147–1155
Sigel K, Wisnivesky J, Justice A, et al (2010) HIV infection is an independent risk factor for lung cancer. 7th Conference on retroviruses and opportunistic infections (CROI 2010). San Francisco
Mugavero MJ, Castellano C, Edelman D, Hicks C (2007) Late diagnosis of HIV infection: the role of age and sex. Am J Med 120:370–373
Wood E, Hogg RS, Yip B, Moore D, Harrigan PR, Montaner JS (2006) Impact of baseline viral load and adherence on survival of HIV-infected adults with baseline CD4 cell counts ≥200 cells/μl. AIDS 20:1117–1123
Crum-Cianflone N, Hullsiek KH, Marconi V et al (2009) Trends in the incidence of cancers among HIV-infected persons and the impact of antiretroviral therapy: a 20-year cohort study. AIDS 23:41–50
Murphy MF, Metcalfe P, Waters AH et al (1987) Incidence and mechanism of neutropenia and thrombocytopenia in patients with human immunodeficiency virus infection. Br J Haematol 66:337–340
Murphy MF, Metcalfe P, Waters AH et al (1985) Immune neutropenia in homosexual men. Lancet 325:217–218
Moore DA, Sullivan A, Hilstead P, Gazzard BG (2000) A retrospective study of neutropenia in HIV disease. Int J STD AIDS 11:8–14
Ben-Galim P, Shaked Y, Garty M, Vonsover A (1996) Immediate immunosuppression caused by acute HIV-1 infection: a fulminant multisystemic disease 2 days post infection. Infection 24:332–335
Philippe C, Cédric F, Malika M, Catherine T (2005) Severe transient neutropenia associated with acute human immunodeficiency virus type 1 infection. Eur J Intern Med 16:120–122
Ribera E, Ocaña I, Almirante B, Gómez J, Monreal P, Martinez Vázquez JM (1989) Autoimmune neutropenia and thrombocytopenia associated with development of antibodies to human immunodeficiency virus. J Infect 18:167–170
Skiest DJ, King ME (1994) Granulocytopenia secondary to acute infection with the human immunodeficiency virus. J Infect 28:315–318
Schacker T, Collier AC, Hughes J, Shea T, Corey L (1996) Clinical and epidemiologic features of primary HIV infection. Ann Intern Med 125:257–264
Levine AM, Karim R, Mack W et al (2006) Neutropenia in human immunodeficiency virus infection: data from the women’s interagency HIV study. Arch Intern Med 166:405–410
Benson CA, van der Horst C, LaMarca A et al (2004) A randomized study of emtricitabine and lamivudine in stably suppressed patients with HIV. AIDS 18:2269–2276
Albrecht D, Vieler T, Horst HA (2002) Rash-associated severe neutropenia as a side-effect of indinavir in HIV postexposure prophylaxis. AIDS 16:2098–2099
Healy BJ, Freedman AR (2006) HIV-related neutropenia exacerbated by efavirenz. HIV Med 7:129–131
Makinson A, Martelli N, Peyriere H, Turriere C, Le Moing V, Reynes J (2007) Profound neutropenia resulting from interaction between antiretroviral therapy and vinblastine in a patient with HIV-associated Hodgkin’s disease. Eur J Haematol 78:358–360
Cingolani A, Torti L, Pinnetti C et al (2010) Detrimental clinical interaction between ritonavir-boosted protease inhibitors and vinblastine in HIV-infected patients with Hodgkin’s lymphoma. AIDS 24:2408–2412
Mir O, Dessard-Diana B, Louet AL et al (2010) Severe toxicity related to a pharmacokinetic interaction between docetaxel and ritonavir in HIV-infected patients. Br J Clin Pharmacol 69:99–101
Coleman MD (2001) Dapsone-mediated agranulocytosis: risks, possible mechanisms and prevention. Toxicology 162:53–60
Olaison L, Belin L, Hogevik H, Alestig K (1999) Incidence of {beta}-lactam-induced delayed hypersensitivity and neutropenia during treatment of infective endocarditis. Arch Intern Med 159:607–615
Zuger A (1996) Profound neutropenia in an HIV-infected man. AIDS Clin Care 8(67):69–70
Lim PL (2009) HIV-related haematological conditions. In: Menon A, Kamarulzaman A (eds) Is it HIV? A handbook for health care providers. Australasian Society for HIV Medicine, Darlinghurst, NSW, pp 52–56
Meynard J-L, Guiguet M, Arsac S, Frottier J, Meyohas MC (1997) Frequency and risk factors of infectious complications in neutropenic patients infected with HIV. AIDS 11:995–998
Tumbarello M, Tacconelli E, Caponera S, Cauda R, Ortona L (1995) The impact of bacteraemia on HIV infection. Nine years experience in a large Italian University Hospital. J Infect 31:123–131
Toeung P, Pouv S, Chel S, et al (2007) Routine switch after 6 months from d4t to AZT containing antiretroviral therapy, at an outpatient HIV clinic in Phnom Penh, Cambodia. International AIDS society conference on HIV pathogenesis, treatment, and prevention. Sydney
Aurpibul L, Puthanakit T, Sirisanthana T, Sirisanthana V (2008) Haematological changes after switching from stavudine to zidovudine in HIV-infected children receiving highly active antiretroviral therapy. HIV Med 9:317–321
Abramson JS, Mills EL (1988) Depression of neutrophil function induced by viruses and its role in secondary microbial infections. Rev Infect Dis 10:326–341
Valone FH, Payan DG, Abrams DI, Goetzl EJ (1984) Defective polymorphonuclear leukocyte chemotaxis in homosexual men with persistent lymph node syndrome. J Infect Dis 150:267–271
Lazzarin A, Uberti Foppa C, Galli M et al (1986) Impairment of polymorphonuclear leucocyte function in patients with acquired immunodeficiency syndrome and with lymphadenopathy syndrome. Clin Exp Immunol 65:105–111
Nielsen H, Kharazmi A, Faber V (1986) Blood monocyte and neutrophil functions in the acquired immune deficiency syndrome. Scand J Immunol 24:291–296
Ellis M, Gupta S, Galant S et al (1988) Impaired neutrophil function in patients with AIDS or AIDS-related complex: a comprehensive evaluation. J Infect Dis 158:1268–1276
Murphy PM, Lane HC, Fauci AS, Gallin JI (1988) Impairment of neutrophil bactericidal capacity in patients with AIDS. J Infect Dis 158:627–630
Pitrak DL, Bak PM, DeMarais P, Novak RM, Burton RA (1993) Depressed neutrophil superoxide production in human immunodeficiency virus infection. J Infect Dis 167:1406–1410
Mullane K, Pitrak D, Bilek M, Novak R, Allen R, Stevens P (1994) In vivo neutrophil activation and burnout in HIV infection. Clin Res 42:155a
Outwater E, McCutchan J (1985) Neutrophil-associated antibodies and granulocytopenia in AIDS. Clin Res 33:413a
Weinberg GA, Gigliotti F, Stroncek DF et al (1997) Lack of relation of granulocyte antibodies (antineutrophil antibodies) to neutropenia in children with human immunodeficiency virus infection. Pediatr Infect Dis J 16:881–884
Nilsson J, Kinloch de Loes S, Granath A, Sönnerborg A, Goh LE, Andersson J (2007) Early immune activation in gut-associated and peripheral lymphoid tissue during acute HIV infection. AIDS 21:565–574
Elbim C, Prevot M, Bouscarat F et al (1994) Polymorphonuclear neutrophils from human immunodeficiency virus-infected patients show enhanced activation, diminished fMLP-induced L-selectin shedding, and an impaired oxidative burst after cytokine priming. Blood 84:2759–2766
Vierucci A, De Martino M, Graziani E, Rossi ME, London WT, Blumberg BS (1983) A mechanism for liver cell injury in viral hepatitis: effects of hepatitis B virus on neutrophil function in vitro and in children with chronic active hepatitis. Pediatr Res 17:814–820
Pitrak DL, Tsai HC, Mullane KM, Sutton SH, Stevens P (1996) Accelerated neutrophil apoptosis in the acquired immunodeficiency syndrome. J Clin Invest 98:2714–2719
Nie Z, Phenix BN, Lum JJ et al (2002) HIV-1 protease processes procaspase 8 to cause mitochondrial release of cytochrome c, caspase cleavage and nuclear fragmentation. Cell Death Differ 9:1172–1184
Busch M, Beckstead J, Gantz D, Vyas G (1986) Detection of human immunodeficiency virus infection of myeloid precursors in bone marrow samples from AIDS patients. Blood 68:122a
Moses A, Heneveld M, Nelson J, Williams S, Rarick M, Bagby G (1995) CD34+ bone marrow microvascular endothelial cells (MVEC) are consistently infected by HIV-1 in patients with AIDS: suboptimal release of IL-6 and G-CSF by infected stromal cells does not depend on release of soluble inhibitory factors. Blood 86:287a
Lagneaux L, Delforge A, Snoeck R et al (1996) Imbalance in production of cytokines by bone marrowstromal cells following cytomegalovirus infection. J Infect Dis 174:913–919
Lieschke G, Grail D, Hodgson G et al (1994) Mice lacking granulocyte colony-stimulating factor have chronic neutropenia, granulocyte and macrophage progenitor cell deficiency, and impaired neutrophil mobilization. Blood 84:1737–1746
Pitrak D, Mullane K, Bilek M, et al (1996) Filgrastim (r-metHuG-CSF) treatment of HIV-infected patients improves neutrophil function. International conference on AIDS. Vancouver
Zhu J, Paul WE (2009) Heterogeneity and plasticity of T helper cells. Cell Res 20:4–12
Williams GT, Smith CA, Spooncer E, Dexter TM, Taylor DR (1990) Haemopoietic colony stimulating factors promote cell survival by suppressing apoptosis. Nature 343:76–79
Pitrak DL, Sutton SH, Tsai HC, Mullane KM, Pau AK (1999) Reversal of accelerated neutrophil apoptosis and restoration of respiratory burst activity with r-metHuG-CSF (Filgrastim therapy in patients with AIDS. AIDS 13:427–429
Wan YY (2010) T regulatory cells: immune suppression and beyond. Cell Mol Immunol 7:204–210
Korn T, Bettelli E, Oukka M, Kuchroo VK (2009) IL-17 and Th17 Cells. Annu Rev Immunol 27:485–517
Schwarzenberger P, Huang W, Ye P et al (2000) Requirement of endogenous stem cell factor and granulocyte colony-stimulating factor for IL-17-mediated granulopoiesis. J Immunol 164:4783–4789
Pelletier M, Maggi L, Micheletti A et al (2010) Evidence for a cross-talk between human neutrophils and Th17 cells. Blood 115:335–343
Conti HR, Shen F, Nayyar N et al (2009) Th17 cells and IL-17 receptor signaling are essential for mucosal host defense against oral candidiasis. J Exp Med 206:299–311
Lin L, Ibrahim AS, Xu X et al (2009) Th1-Th17 cells mediate protective adaptive immunity against Staphylococcus aureus and Candida albicans infection in mice. PLoS Pathog 5:e1000703
ElHed A, Unutmaz D (2010) Th17 cells and HIV infection. Curr Opin HIV AIDS 5:146–150
Peng QL, Zhang MX, Li GY, Liu YX, Zhou BP, Wang H (2010) [Loss of the balance between Th17 and Th1 populations in HIV/AIDS patients]. Zhonghua Shi Yan He Lin Chuang Bing Du Xue Za Zhi 24:17–20
Hunt PW (2010) Th17, gut, and HIV: therapeutic implications. Curr Opin HIV AIDS 5:189–193
Milner JD, Sandler NG, Douek DC (2010) Th17 cells, Job’s syndrome and HIV: opportunities for bacterial and fungal infections. Curr Opin HIV AIDS 5:179–183
Hartung T, Pitrak DL, Foote MA, Shatzen EM, Verral SC, Wendel A (1998) Filgrastim restores interleukin-2 production in blood from patients with advanced human immunodeficiency virus infection. J Infect Dis 178:686–692
O’Connor W Jr, Kamanaka M, Booth CJ et al (2009) A protective function for interleukin 17A in T cell-mediated intestinal inflammation. Nat Immunol 10:603–609
Hambleton J, Aragon T, Modin G, Northfelt DW, Sande MA (1995) Outcome for hospitalized patients with fever and neutropenia who are infected with the human immunodeficiency virus. Clin Infect Dis 20:363–371
Jacobson MA, Liu RC, Davies D, Cohen PT (1997) Human immunodeficiency virus disease-related neutropenia and the risk of hospitalization for bacterial infection. Arch Intern Med 157:1825–1831
Farber BF, Lesser M, Kaplan MH, Woltmann J, Napolitano B, Armellino D (1991) Clinical significance of neutropenia in patients with human immunodeficiency virus infection. Infect Control Hosp Epidemiol 12:429–434
Piliero P, Currier J, Barlam T, Ives D (1995) Risk of bacteremia in HIV-infected person with neutropenia. Second national conference on human retroviruses and related infections. Washington, DC
Shaunak S, Bartlett J (1989) Zidovudine-induced neutropenia. Are we too cautious? Lancet 334:91–92
Keiser P, Higgs E, Smith J (1996) Neutropenia is associated with bacteremia in patients infected with the human immunodeficiency virus. Am J Med Sci 312:118–122
Moore RD, Keruly JC, Chaisson RE (1995) Neutropenia and bacterial infection in acquired immunodeficiency syndrome. Arch Intern Med 155:1965–1970
Eng RHK, Yen K, Tecson-Tumang F, Smith SM, Akgun K (1994) Risk of gram-negative bacteremia during neutropenia in patients with AIDS. Infect Dis Clin Pract 3:373–375
Caperna J, Barber RE, Toerner JG, Mathews WC (1998) Estimation of the effect of neutropenia on rates of clinical bacteraemia in HIV-infected patients. Epidemiol Infect 120:71–80
Mathews WC, Caperna J, Toerner JG, Barber RE, Morgenstern H (1998) Neutropenia is a risk factor for gram-negative bacillus bacteremia in human immunodeficiency virus-infected patients: results of a nested case-control study. Am J Epidemiol 148:1175–1183
Hermans P, Sommereijns B, Van Cutsem N, Clumeck N (1999) Neutropenia in patients with HIV infection: a case control study in a cohort of 1403 patients between 1982 and 1993. J Hematother Stem Cell Res 8:S23–S32
Moore DA, Benepal T, Portsmouth S, Gill J, Gazzard BG (2001) Etiology and natural history of neutropenia in human immunodeficiency virus disease: a prospective study. Clin Infect Dis 32:469–475
Toure S, Gabillard D, Inwoley A, Seyler C, Gourvellec G, Anglaret X (2006) Incidence of neutropenia in HIV-infected African adults receiving co-trimoxazole prophylaxis: a 6-year cohort study in Abidjan, Cote d'Ivoire. Trans R Soc Trop Med Hyg 100:785–790
Vehreschild JJ, Rüping MJ, Steinbach A, Cornely OA (2010) Diagnosis and treatment of fungal infections in allogeneic stem cell and solid organ transplant recipients. Expert Opin Pharmacother 11:95–113
Libanore M, Sighinolfi L, Ghinelli F (2010) Invasive Aspergillosis and HIV infection. In: Comarú Pasqualotto A (ed) Aspergillosis: from diagnosis to prevention. Springer, Netherlands, pp 559–566
Khoo SH, Denning DW (1994) Invasive aspergillosis in patients with AIDS. Clin Infect Dis 19:S41–S48
Pursell KJ, Telzak EE, Armstrong D (1992) Aspergillus species colonization and invasive disease in patients with AIDS. Clin Infect Dis 14:141–148
Libanore M, Prini E, Mazzetti M et al (2002) Invasive aspergillosis in Italian AIDS patients. Infection 30:341–345
Mylonakis E, Flanigan T, Rich JD, Barlam TF (1998) Pulmonary aspergillosis and invasive disease in AIDS. Chest 114:251–262
Kimura S, Matsuda J, Ikematsu S et al (1990) Efficacy of recombinant human granulocyte colony-stimulating factor on neutropenia in patients with AIDS. AIDS 4:1251–1255
Miles S, Mitsuyasu R, Lee K et al (1990) Recombinant human granulocyte colony-stimulating factor increases circulating burst forming unit-erythron and red blood cell production in patients with severe human immunodeficiency virus infection. Blood 75:2137–2142
Miles S, Mitsuyasu R, Moreno J et al (1991) Combined therapy with recombinant granulocyte colony-stimulating factor and erythropoietin decreases hematologic toxicity from zidovudine. Blood 77:2109–2117
Bratt G, Grutzmeier S, Lund B, Sandstrom E. (1992) Granulocyte-colony stimulating factor G-CSF in AIDS-patients with leukocytes less than or equal to 1.0 × 10(9)/L. International Conference on AIDS. Amsterdam Jul 19–24; 8:Mo6 (abstract M0A 0007)
Grutzmeier S, Gerstoft J, Boje Hansen P, Sandstrom E (1996) Filgrastim (G-CSF) use is associated with prolonged survival in AIDS-patients with leukopenia and CD4 cells less than 50 x 106/l. International Conference on AIDS. Vancouver, Canada
Hermans P, Rozenbaum W, Jou A et al (1996) Filgrastim to treat neutropenia and support myelosuppressive medication dosing in HIV infection. AIDS 10:1627–1633
Kuritzkes DR, Parenti D, Ward DJ et al (1998) Filgrastim prevents severe neutropenia and reduces infective morbidity in patients with advanced HIV infection: results of a randomized, multicenter, controlled trial. AIDS 12:65–74
Davidson M, Min Y-I, Holbrook JT et al (2002) Use of filgrastim as adjuvant therapy in patients with AIDS-related cytomegalovirus retinitis. AIDS 16:757–765
Lin S, Marcus CS (1996) Augmentation of leukocyte count with G-CSF in a patient with neutropenia before In-111 WBC scintigraphy. Clin Nucl Med 21:544–546
Keiser P, Rademacher S, Smith J, Skiest D (1998) G CSF association with prolonged survival in HIV infected patients with disseminated Mycobacterium avium complex infection. Int J STD AIDS 9:394–399
Aapro MS, Cameron DA, Pettengell R et al (2006) EORTC guidelines for the use of granulocyte-colony stimulating factor to reduce the incidence of chemotherapy-induced febrile neutropenia in adult patients with lymphomas and solid tumours. Eur J Cancer 42:2433–2453
Ratner L, Lee J, Tang S et al (2001) Chemotherapy for human immunodeficiency virus-associated non-Hodgkin’s lymphoma in combination with highly active antiretroviral therapy. J Clin Oncol 19:2171–2178
Rossi G, Donisi A, Casari S et al (1998) Effects of recombinant granulocyte colony-stimulating factor (G-CSF) in patients treated with ProMACE-CytaBOM for HIV-related non-Hodgkin’s lymphoma (NHL). Haematologica 83:317–322
Tirelli U, Vaccher E (1994) Economic and clinical evaluation of therapy of HIV-related non-Hodgkin’s lymphoma with chemotherapy and granulocyte colony-stimulating factor (G-CSF). Eur J Cancer 30:1589–1590
Foote M (2004) Use of hematopoietic growth factors in AIDS-related malignancies. In: Morstyn G, Foote M, Lieschke G (eds) Hematopoietic growth factors in oncology. Humana Press, Totowa, NJ, pp 357–371
Anderlini P, Donato M, Chan KW et al (1999) Allogeneic blood progenitor cell collection in normal donors after mobilization with filgrastim: the M.D. Anderson Cancer Center experience. Transfusion 39:555–560
Mueller BU, Burt R, Gulick L, Jacobsen F, Pizzo PA, Horne M (1995) Disseminated intravascular coagulation associated with granulocyte colony-stimulating factor therapy in a child with human immunodeficiency virus infection. J Pediatr 126:749–752
Hervé Z, Louis Z, Hervé H, Stéphane H, Isabelle G, Michel C (1995) Probable G-CSF-induced hepatitis and pancreatitis in an HIV-seropositive patient. J Hepatol 22:596–597
D’Souza A, Jaiyesimi I, Trainor L, Venuturumili P (2008) Granulocyte colony-stimulating factor administration: adverse events. Transfus Med Rev 22:280–290
van der Wouw PA, van Leeuwen R, van Oers RH, Lange JM, Danner SA (1991) Effects of recombinant human granulocyte colony-stimulating factor on leucopenia in zidovudine-treated patients with AIDS and AIDS related complex, a phase I/II study. Br J Haematol 78:319–324
Engles-Horton LL, Skowronski C, Mostashari F, Altice FL (1999) Clinical guidelines and pharmacist intervention program for HIV-infected patients requiring granulocyte colony-stimulating factor therapy. Pharmacotherapy 19:356–362
Clumeck N, Wit SD, Hermans P, Franchioly P, Sommereijns B (1992) Recombinant granulocyte colony-stimulating factor (rG-CSF) in HIV patients with zidovudine related neutropenia. J Nutr Sci Vitaminol (Tokyo) Spec no.: 353–356
Garavelli PL (1992) Efficacy of granulocyte colony-stimulating factor (G-CSF) on neutropenia in zidovudine-treated patients with AIDS and ARC: a preliminary report. Haematologica 77:293–294
Goebel FD, Bogner JR, Matuschke A, Heinrich B, Kronawitter U (1992) Effects of granulocyte-colony-stimulating factor in neutropenic AIDS-patients. J Nutr Sci Vitaminol (Tokyo) Spec No. : 357–360
Hengge UR, Brockmeyer NH, Goos M (1992) Granulocyte colony-stimulating factor treatment in AIDS patients. Clin Investig 70:922–926
Jacobson MA, Heard SE (1992) Ganciclovir with recombinant methionyl human granulocyte colony-stimulating factor for treatment of cytomegalovirus disease in AIDS patients. AIDS 6:515–516
Mueller BU, Jacobsen F, Butler KM, Husson RN, Lewis LL, Pizzo PA (1992) Combination treatment with azidothymidine and granulocyte colony-stimulating factor in children with human immunodeficiency virus infection. J Pediatr 121:797–802
Garavelli PL, Berti P (1993) Efficacy of recombinant granulocyte colony-stimulating factor in the long-term treatment of AIDS-related neutropenia. AIDS 7:589–590
Zuccotti GV, Flumine P, Locatelli V, Banderali G, Riva E (1993) Growth factors and HIV-infection in children. J Int Med Res 21:342–345
Hermans P, Franchioly P, Thioux C, Gray SJ, Vannerom H, Clumeck N (1996) Minimum effective dose and duration to reverse neutropenia in non-cancer patients with advanced HIV disease. AIDS 10:1050–1051
Luzzi GA, Jones BJ (1996) Treatment of neutropenic oral ulceration in human immunodeficiency virus infection with G-CSF. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 81:53–54
Perrella O, Finelli E, Perrella A, Tartaglia G, Scognamiglio P, Scalera G (1996) Combined therapy with zidovudine, recombinant granulocyte colony stimulating factors and erythropoietin in asymptomatic HIV patients. J Chemother 8:63–66
Stricker RB, Goldberg B (1996) Increase in lymphocyte subsets following treatment of HIV-associated neutropenia with granulocyte colony-stimulating factor. Clin Immunol Immunopathol 79:194–196
Zuccotti GV, Plebani A, Biasucci G et al (1996) Granulocyte-colony stimulating factor and erythropoietin therapy in children with human immunodeficiency virus infection. J Int Med Res 24:115–121
Ambati BK, Perlman DC, Salomon N (1998) Outcomes of granulocyte colony-stimulating factor or granulocyte-macrophage colony-stimulating factor use in neutropenic patients infected with human immunodeficiency virus. Int J Infect Dis 3:70–75
Keiser P, Rademacher S, Smith JW, Skiest D, Vadde V (1998) Granulocyte colony-stimulating factor use is associated with decreased bacteremia and increased survival in neutropenic HIV-infected patients. Am J Med 104:48–55
Mullane KM. (1998) Rapid clearance of Mycobacterium avium from the blood of nonneutropenic AIDS patients treated with G-CSF (Filgrastim) and antimycobacterial therapy. International congress on infectious diseases. Boston
Dubreuil-Lemaire ML, Gori A, Vittecoq D et al (2000) Lenograstim for the treatment of neutropenia in patients receiving ganciclovir for cytomegalovirus infection: a randomised, placebo-controlled trial in AIDS patients. Eur J Haematol 65:337–343
Aladdin H, Ullum H, Katzenstein T, Gerstoft J, Skinhoslash P, Klarlund B (2005) Immunological and virological changes in antiretroviral naïve human immunodeficiency virus infected patients randomized to G-CSF or placebo simultaneously with initiation of HAART. Scand J Immunol 51:520–525
Aladdin H, Ullum H, Nielsen SD et al (2000) Granulocyte colony-stimulating factor increases CD4+ T cell counts of human immunodeficiency virus-infected patients receiving stable, highly active antiretroviral therapy: results from a randomized, placebo-controlled trial. J Infect Dis 181:1148–1152
Campbell TB, Sevin A, Coombs RW et al (2000) Changes in human immunodeficiency virus type 1 virus load during mobilization and harvesting of hemopoietic progenitor cells. Blood 95:48–55
Nielsen, SøRensen, Aladdin et al (2000) The effect of long-term treatment with granulocyte colony-stimulating factor on hematopoiesis in HIV-infected individuals. Scand J Immunol 52:298–303
Davidson M, Min Y-I, Holbrook JT et al (2002) Influence of filgrastim (granulocyte colony-stimulating factor) on human immunodeficiency virus type 1 RNA in patients with cytomegalovirus retinitis. J Infect Dis 186:1013–1018
Campbell TB, Rapaport E, Schooley RT, Kuritzkes DR (2004) Increased replication of HIV-1 minor variants during hematopoietic stem-cell mobilization with filgrastim. J Infect Dis 190:257–266
Neid JM, Schooley RT, Campbell TB (2004) Stimulation of Kaposi’s sarcoma-associated herpesvirus viremia during hematopoietic stem cell mobilization with filgrastim. Am J Hematol 77:410–412
Pau AK, McLaughlin MM, Hu Z, Agyemang AF, Polis MA, Kottilil S (2006) Predictors for hematopoietic growth factors use in HIV/HCV-coinfected patients treated with peginterferon alfa 2b and ribavirin. AIDS Patient Care STDS 20:612–619
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2012 Springer Basel AG
About this chapter
Cite this chapter
Hemmige, V., Liles, W.C., Pitrak, D.L. (2012). Use of Filgrastim (r-metHuG-CSF) in Human Immunodeficiency Virus Infection. In: Molineux, G., Foote, M., Arvedson, T. (eds) Twenty Years of G-CSF. Milestones in Drug Therapy. Springer, Basel. https://doi.org/10.1007/978-3-0348-0218-5_18
Download citation
DOI: https://doi.org/10.1007/978-3-0348-0218-5_18
Published:
Publisher Name: Springer, Basel
Print ISBN: 978-3-0348-0217-8
Online ISBN: 978-3-0348-0218-5
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)