
Abstract
This introductory chapter argues that tackling the escalating cancer crisis in Africa and India is essential for human wellbeing and inclusive health care, while having much to teach about how to build better local health security in low- and middle-income contexts. Global health security is built on the foundations of strong local health security. Local health security in turn relies on effective and innovative industrial supply chains to provide essential medicines, devices and other commodities at manageable prices, and effective industrial-health sector policy collaboration to ensure broad health benefit, lessons the pandemic has hammered home.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Cancer Care Through a Pandemic Lens: African and Indian Perspectives
This is a book about improving cancer care in Africa and India that is a child of its pandemic times. It has been collaboratively researched and written by colleagues in Kenya, Tanzania, India and the UK, working within a cross-country, multidisciplinary research project, Innovation for Cancer Care in Africa (ICCA).1 We began international meetings and fieldwork in late 2018. We then found ourselves working at a distance and under pandemic restrictions from March 2020 until the time of writing. The project researchers—like so many others across the world—have sustained this research and collaboration through lockdown, personal trauma, illness, bereavement, over-work, frustration, mutual support—and through many virtual international meetings.
Since this was a health-focused research project, ICCA researchers during the pandemic not only continued to work on the cancer research project but were also called upon by their governments to respond to immediate pandemic needs. The variety of those demands to which ICCA researchers responded stretched from supporting and documenting local innovations in African countries, through finding ways to fill supply gaps as international import supply chains collapsed in 2020 (Banda et al., 2021a), to deep involvement of some colleagues in day-to-day management of the pandemic in their respective countries. At the same time, cancer services like other health services were widely undermined by pandemic constraints (Barasa et al., 2021, Martei et al., 2021, Nnaji & Moodley, 2021, Ranganathan et al., 2021).
In combining these two concerns, for improving cancer care and responding to pandemic needs, our original project aims have been challenged, deepened and reworked. ICCA’s initial collaborative research focus included—against the grain of most global health literature—the potential role of enhanced local production of essential healthcare supplies for improving cancer care in African countries. That research focus was built on results of sustained earlier work by some of the ICCA researchers into industrial-health linkages in Africa and in India, and their implications for revisiting theory, research methodology and policy (Mackintosh et al., 2016, 2018a; Srinivas, 2012). The pandemic experience has strikingly validated these earlier findings on the importance of industrial development for health care. That experience identified for national governments and multilateral agencies the central importance of deepening and redirecting industrialisation in African countries as well as other continents to improve healthcare inclusion and strengthen local health security. It has also strongly demonstrated the scale of the opportunity for local industrial/health collaboration, its complexities and its substantial potential benefits.
As a result, the pandemic crystallised for researchers and policymakers an often overlooked phenomenon: global health security is built on the foundations of strong local health security. The whole chain is as strong as the weakest link, especially as concerns highly transmissible infections. We argue in this book that new analytical thinking from social scientists and others is required on how to build local health security. We use the “lens” of original research on cancer care in East Africa and India to build up an understanding of the scope for the development of stronger synergies between local health industries and health care, in order to strengthen local health security and develop tools for policy making. The rethinking and reimagining presented here is required for different African countries, for India and the wider world, and this research on cancer care has taught us that this imperative goes much wider than infectious diseases.
The Cancer Research Focus
The growing challenge of non-communicable diseases in Africa was well recognised by the mid-2010s. Kenyan colleagues, in a research workshop in 2017 aiming to build on our earlier work, presented a reasoned argument for tackling cancer specifically, as an emergent, serious and under-studied non-communicable disease challenge that was gaining a high profile in Kenyan public and policy debate. In contrast to the limited international focus on cancer in low- and middle-income countries when we began in 2018, we find ourselves at the time of writing in 2022 contributing to an expanding research literature on cancer in Sub-Saharan Africa.
As a team of multidisciplinary researchers, we are conscious of the multiple ways that cancer care can be framed, especially with our attention focused on different types of innovation, notably those that can lower cost and simplify delivery but are not antagonistic to scientific advances or the latest technologies. The urgent context of the pandemic also made our diverse training and methods lenses even more visible than at the start. Collaborators on this project had different disciplinary, professional, geographic, national and personal responses to the challenges we were facing. The authors include social scientists from a range of disciplines including economics, researchers with science, engineering, finance and business backgrounds, pharmacists, health systems analysts and clinicians. The chapters are all shaped by these disciplinary divides and include efforts at synthesis, attempting the integration of acutely differing perspectives.
The theme and structure of this book reflect this complex experience. Our sustained argument—in some sense, perhaps, a manifesto—is that African countries and India, like other low- and middle-income countries, can enhance their populations’ health care and health security, regarding both communicable and non-communicable disease, by bringing much closer together health needs, health systems strengthening, health innovations and improved industrial capabilities within new local (national or regional) collaborations. Cancer care provides a key challenge and research field for this argument, since cancer is a hard case (or “wicked problem”) in terms of the number and complexity of cancers and the socio-economic, technical and financial challenges in addressing this complexity.
The book thus argues that tackling the difficult case of cancer care is crucial in itself for human wellbeing and inclusive health care, while the findings and experiences also have much to teach about building better local health security in low- and middle-income contexts with specific reference to Africa and India. Notably, the book advocates for a broader view of cancer care, expanding it beyond the clinic and patient to the supporting social and economic networks and the wider industrial sphere. We bring together industry, health, economic and public policy linkages in new ways, and call for new institutions, infrastructures and processes that can help generate better cancer care. The pandemic can be a turning point towards a greater focus on building local health security in low- and middle-income countries through sustained and purposive linkages of industrial and health capabilities. The book points forward to how that can be achieved.
In a book of this scope, the contributions are several, to improved evidence, more fine-grained analysis, and contributions to theory and methods. This chapter first sets out the motivation for this research, in the scale of the cancer crisis facing low- and middle-income countries and specifically Sub-Saharan Africa and India. We explain why we chose to study cancer care broadly, not initially focusing on specific cancers, and outline our methodologies. This chapter also briefly identifies aspects of the political economy of the health systems in Kenya, Tanzania and India that are relevant for the chapters that follow. It then introduces the industrial context for this research and explains the focus on linkages between industry and health, with reference to the state of the health industries across Africa and in India, and the pandemic context which has brought these linkages to the fore. Finally, we outline the structure of the book.
The Cancer Care Challenge in Low-resource Health Systems
Cancer care is now internationally recognised as an emergent crisis in the health systems of African countries and in other low-resource health systems (WHO, 2020). Since 2017, when the World Health Assembly passed a resolution requesting WHO guidance on cancer prevention and control, there has been a sharp rise in international documentation of the ways in which health systems across the globe are very severely failing cancer patients (Hack et al., 2019; Knaul et al., 2018; Ngwa et al., 2022a; Sullivan et al., 2017). The prevalence of cancers is rising across low- and middle-income countries (WHO, 2020), where evidence of severe suffering and exclusion from cancer care are rightly alarming national and international policymakers.
Sub-Saharan African countries are facing a dual challenge: high and rising levels of non-communicable disease including cancers, and continuing severity of infectious diseases, now sharply worsened by Covid-19. This has put huge pressure on fragile health services. Furthermore, infections and cancers interact: a higher proportion of cancers are linked to infection in Africa than in most other parts of the world (de Martel et al., 2020). The Global Cancer Observatory estimated 1.1 million new cancer cases in Africa (North and Sub-Saharan) in 2020 (Globocan, 2020a). The most commonly reported cancers in Sub-Saharan Africa in 2020 were cervical and breast cancer in women, and prostate cancer in men. Strikingly women’s cumulative risk of dying from cancer was higher in Eastern Africa (11.0%) than in North America or Western Europe (Sung et al., 2021). Cervical cancer was the leading cause of cancer death for women in much of Eastern and Southern Africa: countries including Kenya, Uganda and South Africa record rising premature mortality from cervical cancer, a largely preventable illness (Jedy-Agba et al., 2020). Breast cancer incidence is also rising rapidly in Sub-Saharan Africa, where breast cancer mortality rates are now some of the highest in the world (Joko-Fru et al., 2020). Both incidence and mortality rates for prostate cancer have also risen in Eastern and Southern Africa, and this is the leading cause of cancer mortality among Sub-Saharan men (Seraphin et al., 2021).
A major cause of high cancer mortality in Sub-Saharan African countries is late stage diagnosis, and therefore starting treatment at stages 3 or 4. High case fatality rates are closely associated with late stage diagnosis and treatment (WHO, 2020). It is recognised that downstaging cancer diagnosis and treatment can improve outcomes even in low-resource systems. Furthermore, downstaging can be achieved for cancers with external symptom markers, for example breast and cervical cancer, without population-based mammography, and by using trained health aides (Duggan et al., 2021; Ngoma et al., 2015). More broadly, it is recognised that low-resource health systems suffer from a very severe shortage of diagnostic capabilities (Fleming et al., 2021).
Pathology limitations are a major constraint on cancer diagnosis, alongside a failure by high-income country-based funders to focus on pathology requirements (Horton et al., 2018). Other barriers to timely cancer diagnosis include stigma and lack of public awareness of symptoms; misdiagnosis within the health system and financial barriers to diagnostics such as imaging (Brand et al., 2019). There are also documented delays, financial barriers and lack of availability of treatment including chemotherapy and radiography resources (Elmore et al., 2021). Finally, the widespread lack of access to palliation and pain control has been described as an “abyss” (Knaul et al., 2018). All this has been worsened by the pandemic impact on access to cancer care (Mutebi, 2021).
Despite higher levels of resource, India has also long struggled to provide effective cancer care for its population. Incidence has been rising (Mallath et al., 2014; Smith & Mallath, 2019), with an estimated 1.3 million new cancer sufferers in India in 2020 (Globocan, 2020b). Patients face continuing problems of misdiagnosis, late-stage diagnosis and poor treatment outcomes, and inequality in access to care is compounded by the burden of out-of-pocket payments (Pramesh et al., 2014). Covid-19 has had a documented major impact in further impeding access to cancer care in India, from screening to treatment (Ranganathan et al., 2021). Delivering affordable and equitable cancer care in India’s complex health system has been described as “one of India’s greatest public health challenges” (Pramesh et al., 2014, p. e223).
Across Sub-Saharan Africa, and also in India, governments have recently been giving greater policy attention to cancer care. Public pressure has helped to push cancer care up the political agenda in African countries. Cancer registries and data are improving in quality and scale. In East Africa, some countries have recently added oncology medicines to their essential medicines lists, following WHO essential medicines guidance, and have developed or updated cancer treatment guidelines MoH Kenya (MoH, 2017, 2019). India has had a National Cancer Control Programme since the 1970s.2 India’s ambitious new National Cancer Grid brings together a vast network of cancer centres that work at setting standards for care, providing training and supporting research (Pramesh et al., 2014)3 North-eastern India which faces a high cancer burden now has several regional cancer centres in Assam, new hospitals and training centres and education efforts serving the region.4 There is an increasing focus on adapting cancer care to improve access and outcomes in low-resource countries including India (Pramesh et al., 2019; Sullivan et al., 2017).
Cancer and the Health Industries
Industrial organisation is a vital foundation for the study of cancer care innovation and a key contributor to improvements in care. This argument, a core theme of this book, remains rarely reflected in frameworks of analysis of health systems in general and cancer care in particular. The quality of health care self-evidently relies on the timely availability of industrial supplies of essential medicines, medical devices and equipment, diagnostics, laboratory reagents and other essential commodities such as disinfectants. The Covid-19 pandemic has reinforced awareness of the fragility of international supply chains for health care. It is time for the industrial building blocks of health systems to be now integrated into revised frameworks for health analysis and policy as well as interventions.
By “health industries” in this book we mean all these industrial suppliers, and also their upstream reliance on active pharmaceutical ingredients (APIs) and other major inputs from the chemicals, plastics and other industries. And by “local production”, we mean all such manufacturing undertaken within a specified country or region, whatever the ownership structure.
In these terms, the contrast between India and Sub-Saharan African countries is sharp, and some aspects of that contrast are explored in this book. India benefits from depth and breadth of industrial scale and capabilities in the health industries developed over many decades. India’s pharmaceutical companies, many multinational in operation, are global suppliers of generic medicines and are increasingly innovative. They are the dominant suppliers of essential medicines in Eastern and Southern Africa. India’s medical device industries, though less internationally dominant, are extensive, growing and highly innovative. India also displays industrial depth in upstream suppliers and input products from plastics to design consulting services.
While the Indian pharmaceutical and other health industries have been extensively studied, this is not the case for the health industries of Sub-Saharan Africa. We therefore briefly survey here the current state of these industries, as a background to the chapters to follow.
The State of Health-related Manufacturing Across Africa
Many Sub-Saharan African countries have a long history of pharmaceutical production, from the colonial period onwards (Banda et al., 2016b). Some countries, including South Africa, Kenya, Nigeria and Ghana, have substantial industrial clusters of pharmaceutical firms, predominantly locally owned, which have survived the exit of most large US- and Europe-based multinationals in the 1980s and 1990s (Mackintosh et al., 2016).
Figure 1.1 summarises the current footprint of medicines production across Africa.5 The African continent is home to over 689 pharmaceutical manufacturers, many of which fall in the small to medium enterprise category. North Africa has the greatest number (estimated at 272), followed by West Africa (estimated at 213), Southern Africa (estimated at 139) and East Africa (estimated at 65). The largest industrial clusters of local pharmaceutical manufacturing are in South Africa (122), Egypt (120) and Nigeria (150). Others with 30 or more plants include Algeria, Tunisia and Morocco; Kenya, the East African hub and Ghana. Smaller industrial clusters exist in Sudan, Cameroon, Ethiopia and Uganda.

(Source Author’s calculations)
The African pharmaceutical manufacturing footprint as of 2022
Most of this production is of basic generics (tablets and capsules including antibiotics; topical preparations and syrups for children). Some firms in Kenya, South Africa and elsewhere can produce injectables under sterile conditions. Product ranges are limited, and few firms can produce more complex generics such as those required for non-communicable diseases, or those embodying slow-release or dual-layer tablets. At the time of writing there is very little oncology drug production in Sub-Saharan Africa.
North Africa is the most vibrant region and Egypt has the most local pharmaceutical manufacturers. North Africa leads in formulations and technological capabilities and has successfully used technology transfer to move upstream in drugs and biologics technologies. The vaccine manufacturing footprint on the continent is much smaller. There are only four countries with vaccine manufacturing plants: Egypt, Senegal, Tunisia and South Africa (Fig. 1.1). These four countries manufacture drugs, vaccines (hatched pattern in Fig. 1.1), and feature prominently in current efforts for local Covid-19 vaccine manufacture on the continent.
The only API manufacturing companies are in South Africa, with a very limited product range. APIs and excipients are otherwise imported from China, India and some European countries. This very high import dependence for APIs creates a concentration risk for Africa with particular regard to China.
Medical devices and diagnostics manufacturing is a much smaller segment of the health industries in Africa (Mkwashi, 2020). The limited device manufacturing placed the continent on a poor footing to be prepared for Covid-19. There remains high dependence on imports of raw materials from India, China and elsewhere for the medical devices and diagnostic industry, and for chemical reagents, the scale and range of locally produced products is very limited. China is an increasingly important supplier of devices and equipment to African countries’ health systems. The lethargic development of the medical device sector may be attributable to a lack of concerted policy efforts to develop the sector by supporting entrepreneurs and providing appropriate regulatory and governance systems for devices and diagnostics (Mkwashi, 2020; WHO, 2016b).
Sub-Saharan African countries’ health systems thus remain very heavily import-dependent for manufactured health commodities, in sharp contrast to India’s deep industrial capabilities in these health-related industries, and indeed in contrast to the somewhat stronger industrial base of some North African countries such as Egypt and Morocco. This import dependence is in sharp contrast to India’s ability to supply a large proportion of its medicines requirements from its highly successful pharmaceutical sector, and India’s lively medical device industry.
Even before Covid-19, new national government policy attention was being paid to local pharmaceutical production in a number of African countries, including Tanzania and Kenya. New investors were also coming into the East African pharmaceutical industry from India, Bangladesh and South Africa, and this investment was associated with industrial upgrading and expansion of product range (Wangwe et al., 2021). The pandemic however transformed this policy landscape. As imports dried up, prices of inputs rose vertiginously, and international transport stopped, the limitations of local industrial production became evident (Banda et al., 2021a). Even India, with its far stronger industrial base, reflected more sharply on its dependence on China for bulk imports of active pharmaceutical ingredients (APIs) for its medicines’ production (Chatterjee, 2020). And the lack of vaccine manufacturing in SSA was thrown into particularly sharp relief. The shift in thinking within global health debates towards support for more local production of essential health commodities within low- and middle-income countries, including Africa, was sharply illustrated by the WHO’s convening of the first World Local Production Forum in June 2021 (WHO, 2021c).
It became clear, as the pandemic developed, that those African countries with a somewhat stronger industrial base were able to respond more effectively to the pressure for import substitution by health industries, from local production of protective equipment and sanitiser to test kits and oxygen supply (Banda et al., 2021a). India, with a large vaccine producer in addition to its other industrial strengths, was able to do much more.
In Africa, furthermore, the crisis added fuel to the local policy debates on routes to greater self-reliance, adaptation of health care to local needs, local industrial-health sector collaboration and arguments for decolonisation of research and policy priorities. African governments, multilateral African institutions and high-income country-based funders have focused attention on localising vaccine production in African countries, and the investment and technology transfer required (Irwin, 2021; Nkengasong et al., 2020). Internationally there are cautions about the industrial and trade strategies to accomplish this (Fransen et al., 2021).
A Kenyan clinician also recorded a pandemic-induced upsurge of virtual networks and clinical knowledge sharing that has helped to “democratise” access to learning resources, including an East African weekly medical education event in oncology (Mutebi, 2021). She argued for more global attention to local solutions to tackling complex systemic problems, citing “Choosing Wisely Africa” (Rubagumya et al., 2020) as a practical exercise in identifying locally appropriate clinical approaches in cancer care. A contrast is often drawn in East Africa between the international financial and infrastructural support for HIV and TB treatments versus the lack of such support for cancer treatment. However, there are warning voices that high-income country-based support for expanding cancer treatment needs to avoid “onco-colonialism” by building collaborative partnerships that meet rather than override national priorities, and that strengthen local health system integration (Hack et al., 2019).
Researching Cancer Care: Methods and Contexts
“Cancer is a deeply personal disease”. Tedros Adhanom Ghebreyesus, Director-General, World Health Organization. (WHO, 2020)
While most writing on cancer is clinically focused, cancer is, as the WHO Director-General noted, “personal”: a disease that affects us all, and generates huge levels of “physical, emotional and financial strain on individuals, families, communities, health systems, and countries” (WHO, 2020, p. 12). A key argument in this book is that cancer is deeply social in its impact on patients, families, carers, communities and economies. The research on cancer care in this book is therefore rooted in social science methodologies appropriate for tracing these effects, though the research teams also included expert clinicians. We aim to explore and present in this book a range of predominantly African and Indian perspectives on cancer care, including the perspectives of those who have experienced the disease as well as their carers, health professionals, policymakers and industrialists in Eastern and Southern Africa and India. A variety of robust research methodologies were applied across the three countries, mixing quantitative and qualitative study design and drawing on a range of analytical frameworks.
Perspectives on Cancer Care
The ICCA project of which this book is an outcome took the decision at the start not to focus on specific cancers, but to seek experiences of cancer care in general and the scope for policy responses. We are aware that “cancer” refers to a wide and complex range of illnesses. But we recognised, and have seen it confirmed, that policymakers and patients do also think about cancer as a general category of disease, despite the complex range and diversity of interventions needed, which makes private sector involvements unpredictable and difficult to regulate (Srinivas, 2021b). We identified across the cancer care spectrum shared issues for cancer patients and for all those impacted by the disease, from diagnostic costs and cost of treatment, through fear and stigma, and access to pain control, to industrial production and trade in essential supplies such as oncology drugs. We also refer to experiences of distinct cancers where appropriate, especially those that are most prevalent and those for which earlier diagnosis would be both possible and life-sustaining.
While the literature on cancer in Africa and India is expanding rapidly, it largely continues to operate in a health system research “silo”, within which the industrial and distributive institutional structures that shape the supply of essential commodities are not considered. Yet improving cancer care centrally includes effective industrial supply chains and the innovation required to provide essential medicines, devices and other commodities at manageable prices, a lesson the pandemic has hammered home.
It is our contention in this book therefore, for the important and challenging case of cancer care, that building local health security while moving towards Universal Health Coverage (UHC), in East Africa and India as elsewhere, must include close attention to building the linkages and mutual interactions of investment and innovation in industry, regulation, market management, health system demand and procurement, as well as health system organisation. We locate our research findings within the perspective of strengthening local health systems partly through reinforcing linkages with local industrialisation efforts. We identify major challenges for cancer care that can be addressed through cross-sectoral, multidisciplinary collaborations within resource-constrained systems and demonstrate practical broad-spectrum approaches to policy making for this purpose.
The development of our argument in this book is mainly narratival. We draw on some quantitative survey results and secondary data analysis where appropriate, using them as elements of our arguments from the extensive qualitative primary interviews. Our aim as a multidisciplinary team is to reflect and convey, through the use of narrative cases and summary evidence, the perspectives of the hundreds of stakeholders in cancer care, who gave their time in difficult circumstances, on the current functioning of cancer care and the scope for improvement through innovations that link industry and health. We describe the research methods below.
Health Sector Research Methods
Extensive fieldwork was carried out for the ICCA project on the experience of cancer care in Tanzania and Kenya, from the perspectives of patients, carers, cancer survivors, health professionals and other stakeholders including procurement agents and policymakers. The research included a survey of 467 cancer patients’ experiences (405 in Kenya and 62 in Tanzania). The interviews invited patients to narrate their “pathways”, using a structured questionnaire. Patients were asked to start from first recognising worrying symptoms and to recount their experience to date as a series of self-defined events. For each event, patients were asked what they did, when, where, what happened as a result, what they paid and how they paid; also how they travelled if required. Background information on gender, hometown or village, economic activity and estimated household income was included, and patients were finally asked for comments, including missed requirements and aspects that could be improved. This interview structure, innovative in this field at the time, allowed us to combine gathering narratives in which the steps reflected patients’ perspectives on events and hurdles. Later, the analysis could identify clinical hurdles such as diagnosis and analyse patients’ experiences for aspects such as length of delays before diagnosis and amounts expended in relation to self-estimated household income.
A parallel set of in-depth interviews in Tanzania and Kenya sought the perspectives of health professionals (doctors, nurses, clinical officers, pharmacists and community health workers) and also caregivers and policymakers (43 interviews in total). Focus groups with cancer survivors and health workers added to qualitative understanding, allowing discussion of perspectives. The study participants were recruited in three Kenyan counties and three regions in Tanzania.
Industrial Research Methods
In the most innovative aspect of this project’s methodology, in addition to the health data, in-depth interviews were conducted with health-related industrialists in both East Africa and India. In Tanzania and Kenya, we interviewed local manufacturers (16 in total in East Africa including also one Ugandan manufacturer), plus public and private importers/distributors (3) and regulators and policymakers (5). The interviews explored manufacturers’ product range, their interest in expanding into cancer-related production, and their understanding of local market demand for cancer-related items in short supply or unavailable to respond to need. The range of manufacturing organisations included firms producing pharmaceuticals and other health-related products such as medical devices, chemicals and plastics.
In India, with its large and innovative industrial base, the initial research focus was exclusively on the industrial organisation of firms and the “cancer industry” of diverse products and services. A central concern was Indian industrial and technological innovations relevant to cancer care in resource-constrained health services. However, early interviewing rapidly expanded the research focus to investigate the interconnections (and lack of connections) between healthcare provision and industrial change, including interviews with clinicians, scientists and industrialists working on this interface. It became clear, in part through pandemic experience, that the Indian team needed to explore the often disconnected but often separately analysed productive ecosystem of economics, surgery, entrepreneurship, regional care hospitals and laboratory science. Findings from 25 in-depth interviews and discussions, many with follow-up discussions and emails, are drawn on in this book, alongside innovative open-resource podcasts and video materials,6 created by the Indian team as a dividend of the new at-distance world we were inhabiting, and a necessary action to identify and create public dialogues between disparate actors.
The chapters in this book draw extensively on this large data resource, collected both before and during the pandemic. In addition, the chapters draw on wider interviewing of industrialists in the context of related work on pandemic responses and pandemic-incentivised investment initiatives, notably in vaccines,7 as well as secondary sources and literature review as indicated in the chapters that follow.
Health System Organisation: Key Aspects
The Tanzanian and Kenyan health systems share a number of characteristics relevant to tackling cancer care. Each has a public health system under constant stress from funding constraints and high levels of need and demand; in each country the bulk of the population survive on low incomes and rely on public health care. In both countries, most health facility visits require payment out-of-pocket in cash. Efforts to mitigate the impact of these charges on access to care include insurance initiatives and exemptions from payment for certain categories of patients or types of care, but out-of-pocket payments remain a major impediment to patients’ access to care.
In both countries the public health system is hierarchically structured. In this book, we refer to primary levels of care including community health workers, dispensaries and health centres; first-line or local hospitals including district hospitals in Tanzania and sub-County hospitals in Kenya, that is, the general hospitals most accessible to most patients; and referral hospitals including those offering different levels of specialist care, typically including diagnostic testing and cancer treatment centres. Patients are typically envisaged to start at lower levels and be referred upwards as needed; as will be seen, cancer patients’ experiences are however rather different.
In addition, both Tanzania and Kenya have a private sector in health care, with the Kenyan private sector markedly larger. The private facilities vary greatly, but include private dispensaries and maternity homes, private diagnostic laboratories and higher-end private hospitals. The pattern of public and private provision can have a marked effect on the experience of cancer patients, including access to timely diagnosis.
In India, healthcare structure and performance vary sharply between states. However, both not-for-profit organisations and the businesses of the private sector are acknowledged to be central to health service performance across the country, even those often seen to be “public” or “community health”. There is now an emerging debate on the relative roles of public and private cancer care, in Africa and more broadly in LMICs including India. In East Africa, Indian private sector cancer care is also known as a resource for African cancer patients with comprehensive insurance or high incomes, who pre-pandemic travelled to Indian hospitals such as the Apollo chain for diagnosis, treatments and follow-up. This can provide a misleading impression in Africa of Indian cancer care which however suffers, more broadly, from many problems familiar in African contexts, including public sector cancer treatment centres overwhelmed by high demand (Pramesh et al., 2014; Sirohi et al., 2018) and widespread failures of timely diagnosis.
On both continents, the evolving role of the private sector and private funding in cancer care therefore poses policy challenges for moving towards UHC. Public and non-profit hospitals may rely on international philanthropic support for diagnostic equipment, training and staffing and struggle when that support is reduced. The concentration of expertise in a small number of cancer centres, while supporting the retention of expertise and research development can force patients to travel very long distances in search of care. Challenges for policymakers include finding and applying models that bring aspects of cancer care much closer to patients, and creating stronger links between private and public sector care. India’s Cancer Grid, Kenya’s external partnerships such as AMPATH, and Uganda’s success in bringing pain control closer to patients are some of the many current responses to these challenges.
Book Structure: Evidencing and Reframing the Challenges
This book begins by locating the research on cancer within the pandemic context that has shaped our work since 2020. Chapter 2 surveys the pandemic context in both Africa and India within which this research has been done. It documents the immense scale of the resultant healthcare supply crisis, especially in Sub-Saharan Africa, and identifies the extent to which a stronger industrial base allowed India, and some African countries, to better tackle the pandemic supply gaps. The scale of the rethinking forced on governments by Covid-19 can be understood, the chapter argues, as a shift in socio-technical imaginaries: new manageable, social and technical, shared visions of what is possible and important in addressing local health security. The pandemic also confirmed the widespread pre-pandemic African predictions that in a major crisis, African countries would find themselves at the back of the queue, while wealthier countries first looked after their own. Recognition of that truth and its implications are driving the new view of industrialisation’s role in local health security. This book applies this new imaginary to the huge challenge of cancer care in Africa.
The next section of the book, “The cancer care experience in East Africa” (Chapters 3–5) explores key aspects of how the “cancer explosion” in Africa (Ngwa et al., 2022, p. e252) is experienced in Kenya and Tanzania, drawing on the health system fieldwork. Each chapter argues for a specific reframing of the understanding of the cancer care challenge in these countries. Chapter 3 reframes the scale of cancer crisis through the concept of “social pain”. This concept, used by the interviewees themselves, understands cancer as a whole-society problem, with psychological, social, economic and spiritual impacts much wider than the sufferer. The chapter argues for much more attention to survivability and human dignity in policies, practices and provision.
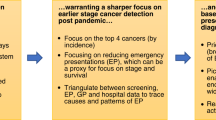
Chapter 4 turns to the experience of individual sufferers and creates an image of how cancer care appears to them in the narratives they shared. The image frames their experience as being confronted by a “maze”, through which they grope largely on their own initiative. Too often, patients lacked maps or guides to aid their search for information, diagnosis and treatment. The chapter presents patterns of experience within the maze and implications for access to care. Chapter 5 then steps back from that maze and examines it from the perspective of health system professionals aiming to create a smooth, managed pathway to and through cancer care. The chapter reframes the challenge of late diagnosis, a key cause of poor patient outcomes. Instead of the familiar frame of “late presentation”, a concept tending to focus attention on patients’ behaviour as a source of delay, the chapter identifies core bottlenecks once patients come to the health services and points of leverage for improvement.
The next section, “Local industry and cancer care in India and Africa” (Chapters 6–8), examines the disjunctions and gaps between cancer care and industrial production in both India and East Africa. Chapter 6 is written from the Indian perspective of a country with a much stronger local industrial base and innovative capabilities, yet struggling to build on that advantage to sharply improve access to timely cancer diagnosis and treatment. The framing of the chapter challenges the reader to understand the complexity of responsibility in designing viable policy, the linkages and gaps between the economic basis for the industrial “building blocks” of cancer care and the health system that uses the products. The chapter draws directly on the author’s Covid-19 experiences of working across health/industrial boundaries under pressure and forces attention to conceptual frames and gaps in policy that block effective translation of need into secure supply.
Chapters 7 and 8 then explore the current state of the health industries in East Africa, the failure to address cancer-related requirements and the scope for investment and innovation. Chapter 7 surveys the current state of development of the health industries in Kenya and Tanzania. It frames this, perhaps controversially, as a lack of ambition on the part of the entire local industrial/innovation ecosystem, including manufacturers, entrepreneurs, regulators and policymakers. The pharmaceutical firms were failing to upgrade, expand product ranges and develop new markets, though that was starting to change before the pandemic. The chapter identifies market disorganisation and fragmentation as one of a number of key constraints on improving cancer-related manufacturing and points to the scope for institutional change to link industrial incentives to health needs. Chapter 8 then focuses on the scope for local production of oncology medication, drawing on local clinical needs in East Africa, on Indian data on markets for generic oncology medication, and on industrial and regulatory experience.
The next section, “Industrial innovation and industrial policy” (Chapters 9–11), examines three areas where industrial innovation and investment have high potential for health-linked industrial development and health improvement: medical devices, vaccines and biologics and medication for severe pain. Chapter 9 describes and discusses several Indian medical device start-ups with potential for improving cancer care in low-resource health systems. It explains the emerging business models of these firms in India’s innovative medical devices sector, identifying regulatory and policy successes and failures and the adaptations of innovative start-ups to the complexity of cancer care markets in India. It identifies innovative ways in which India supports entrepreneurship through incubators and funding in the medical devices sector and draws some lessons for African policy actors on how to structure innovation ecosystems that can support emerging local health-industry complexes.
Chapter 10 then turns to the high-profile topic of vaccines. Charting the explosion of international interest and investment in vaccine production in Africa, the chapter argues for a rethinking of the scope for investment. The chapter argues that better cancer care entails the expansion of technological capabilities in biologics manufacture. The current vaccine manufacturers are the possible candidates to transition into the biologics sector because this is an incremental innovation for them. It argues that the current interests in vaccine manufacture can be seized by national policymakers as an opportunity to develop broader biotechnology manufacturing capabilities.
Chapter 11 is the first of two chapters to explore the local specificities of a broad cancer care crisis that crosses countries and types of cancer: pain management. There is a well-acknowledged failure to provide effective strong pain medication for late-stage cancer sufferers in Sub-Saharan Africa and India and elsewhere outside high-income countries (Knaul et al., 2018). Chapter 11 tackles this problem in the first of two sharply contrasting contexts: India, where the entire supply chain of industrial production of morphine is within the country, yet the need remains unmet. It shows that cost is not the main constraint on access to pain relief and explores the systemic institutional gaps between clinical training, decentralised care, ambition and scope of supply chain management and ability to carve out national autonomy on palliation needs that prevent resolution of this crisis. In India, the complexity is increased by the state-level responsibility for most areas of health policy.
The final section of the book, “Tackling institutional gaps: using scenarios” (Chapters 12–14) looks forward. Chapter 12 picks up the analysis of the crisis in access to pain medication in Tanzania, where all opiate medication is imported and needs are also largely unmet. The chapter analyses the complex sources of this cancer care failure and contrasts the Tanzanian situation to the Ugandan approach to providing more widespread access to opiate medication for severe pain. It reports the findings of multi-sectoral and multidisciplinary workshops in Tanzania aiming to find a way forward.
Chapter 13 then builds on the evidence in Chapter 12, as part of an exploration of a practical tool for addressing complex social and economic challenges of this type: scenario building. The interviews in Kenya and Tanzania had identified a number of serious unmet needs for cancer patients that could in principle be met without unmanageable requirements for additional funding. In addition to the lack of control of severe pain, cancer patients and cancer survivors were eloquent about the difficulty of obtaining, at all or at manageable prices, commodities that are essential for living with cancer productively and with dignity, including colostomy bags and prostheses. Chapter 13 describes in practical terms the use of collaborative scenario building with stakeholders from industry and healthcare, including clinicians, policymakers and regulators to identify interlocking constraints and scope for intervention to create virtuous circles of improvement.
The concluding Chapter 14 pulls together analytical themes and practical lessons from the book as a whole.
Notes
-
1.
See Acknowledgements for details: the authors are grateful to the Economic and Social Research Council, UK for research funding; the authors are solely responsible for the book content.
-
2.
https://main.mohfw.gov.in/Organisation/Departments-of-Health-and-Family-Welfare/national-cancer-control-programme. Accessed 23/03/22.
-
3.
See also https://tmc.gov.in/ncg/. Accessed 23/03/22.
-
4.
See https://www.tatatrusts.org/media/press-releases/pm-inaugurates-multi-level-cancer-care-network-in-assam; https://theprint.in/india/ayushman-bharat-scheme-helped-in-early-detection-of-cancer-pm-modi/934803/. Last accessed 18-10-2022.
-
5.
These data were updated with funding support from the Open Society Foundation for a project at the Institute of Economic Justice, Johannesburg. Research collaboration including data collection and analysis by Andrew Mkwashi and Julius Mugwagwa is gratefully acknowledged. The content of this chapter is the sole responsibility of the authors.
-
6.
ICCA India podcast series 2021 https://www.youtube.com/watch?v=03T3pFKufHQ. See also https://www.lgcw.org.uk/event/economics-and-updating-the-war-on-cancer-hosted-by-the-open-unversity/.
-
7.
One of the authors is a member of the African Vaccine Manufacturing Initiative (AVMI). AVMI is an association composed of current and aspiring African vaccine manufacturers, and its remit is promoting local vaccine manufacture through advocacy, technology transfer and industrial development.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2024 The Author(s)
About this chapter

Cite this chapter
Mackintosh, M., Banda, G., Njeru, M.K., Srinivas, S., Makene, F.S. (2024). The Cancer Care Challenge in the Light of Pandemic Experience. In: Banda, G., Mackintosh, M., Njeru, M.K., Makene, F.S., Srinivas, S. (eds) Cancer Care in Pandemic Times: Building Inclusive Local Health Security in Africa and India. International Political Economy Series. Palgrave Macmillan, Cham. https://doi.org/10.1007/978-3-031-44123-3_1
Download citation
DOI: https://doi.org/10.1007/978-3-031-44123-3_1
Published:
Publisher Name: Palgrave Macmillan, Cham
Print ISBN: 978-3-031-44122-6
Online ISBN: 978-3-031-44123-3
eBook Packages: Political Science and International StudiesPolitical Science and International Studies (R0)