
Abstract
The concentrations of a number of polybrominated substances were determined in pooled human milk samples collected from up to 80 countries from all the United Nations Regional Groups. The samples were taken from one or more of the five exposure studies on persistent organic pollutants coordinated by the World Health Organization and the United Nations Environment Programme between 2000 and 2019.
Large differences in levels were found for polybrominated diphenyl ethers (PBDE). The concentration of the sum of 6 PBDE congeners (∑PBDE6: BDE-47, BDE-99, BDE-100, BDE-153, BDE-154, BDE-183) of 135 pooled samples from 80 countries was in the range between 0.3 and 352 ng/g lipid (median 1.6 ng/g lipid). The highest concentrations were detected in the Western European and Others Group (including Australia, Israel, New Zealand, and the USA) in 2003. Time trends were assessed for 36 countries with repeated participation. Rates of decrease tend to fluctuate at near background levels; but at higher levels, a decreasing trend was observed for nearly all countries. Deca-BDE (BDE-209) contributed on average about 13% to ∑PBDE7 (sum of ∑PBDE6 plus BDE-209). The contribution of the octa-brominated diphenyl ether (octa-BDE) BDE-197 and nona-BDEs-206, -207, and -208 to the sum of 25 PBDE was in the range of the six recommended analytes and BDE-209. Therefore, their addition to the list of recommended analytes should be considered.
The α-HBCDD levels of 102 pooled samples from 72 countries collected between 2006 and 2019 ranged between <0.1 and 15 ng/g lipid (median: 0.5 ng/g lipid). β-HBCDD and γ-HBCDD were in nearly all samples below the limit of quantification (LOQ for 90% of the samples: <0.1 ng/g lipid) or around the LOQ (max: 0.8 ng/g lipid). Thus, it can be concluded that α-HBCD is the predominant stereoisomer in human milk.
Hexabromobiphenyl (PBB 153) was below the limit of quantification (0.5 ng/g lipid) in 106 of 110 pooled samples from 69 countries. In four samples, low concentrations of between 1.0 and 1.7 ng/g lipid were found.
In addition to these chemicals listed by the Stockholm Convention on Persistent Organic Pollutants, in 38 pooled samples from 28 countries concentrations of polybrominated dibenzodioxins and -furans (PBDD/PBDF) were determined to assess their contribution to the overall sum of WHO2005 toxic equivalents (TEQ) with polychlorinated dibenzo-p-dioxins (PCDD) and polychlorinated dibenzofurans (PCDF). PBDD and PBDF provided on average about 10% to the overall TEQ calculated as sum of WHO-PCDD/PCDF-TEQ and WHO-PBDD/PBDF-TEQ, when assuming the same toxic equivalency factors for brominated congeners as assigned to their chlorinated analogs. No correlations between PCDD/PCDF and PBDD/PBDF, or PBDD/PBDF and PBDE were found.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others

Keywords
- Human milk biomonitoring
- Stockholm Convention on Persistent Organic Pollutants
- Polybrominated diphenyl ether (PBDE)
- Hexabromocyclododecane (HBCD or HBCDD)
- Hexabromobiphenyl (HBB)
- Polybrominated dibenzo-p-dioxins and dibenzofurans (PBDD/PBDF)
- Global WHO/UNEP human milk studies
- UN regional groups
- Time trends
1 Introduction
A number of organobromine compounds with an inhibitory effect on combustion processes are used as flame retardants (brominated flame retardants [BFR]). Among them are the polybrominated diphenyl ethers (PBDE), hexabromocyclododecanes (usual abbreviations: HBCD or HBCDD; in this article used: HBCDD), and hexabromobiphenyl (HBB). As chemically and physiologically stable substances, they persist in the environmental and biological systems. Due to their lipophilic properties and often slow metabolization, biomagnification in the food chain and bioaccumulation in fatty tissues of animals and humans occurs readily. For these reasons, these compounds are formally classified as persistent organic pollutants (POPs) (UNEP 2017).
To protect human health and the environment, the Stockholm Convention on POPs has identified selected POPs to reduce or eliminate their release into the environment (UNEP 2001). In 2009, hexabromobiphenyl and tetra-, penta-, hexa-, and heptabromodiphenyl ethers were listed under the Convention, followed in 2013 by HBCDD and in 2017 by decabromodiphenyl ether (Deca-BDE) (UNEP 2020). As a result, these POPs are now subject to Article 16, which requires that they be monitored to evaluate the effectiveness of the Convention. The analysis of those POPs in human milk has been recommended as one of the core matrices within the framework of the Global Monitoring Plan on POPs (GMP) (UNEP 2019).
Polybrominated dibenzo-p-dioxins and dibenzofurans (PBDD/PBDF) can be found in a wide variety of abiotic and biological matrices. Sources for environmental release include commercial mixtures of BFR, in which PBDD and PBDF may occur as impurities. In addition, de novo formation of these compounds occurs during combustion processes in which bromine is present. During these processes, significant amounts of PBDD and PBDF can be formed, including those congeners that are analogs of the most toxic chlorinated dioxins and dibenzofurans (PCDD/PCDF) in terms of their halogen substitution pattern. Because of their similarity in biological and toxicological properties with chlorinated analogs, the World Health Organization (WHO) has established interim values for Toxicity Equivalency Factors (TEF). Due to the similarity in toxic properties between chlorinated and brominated dioxins and dibenzofurans both groups of compounds should be combined in this TEF concept (van den Berg et al. 2013), until sufficient data on their toxicity is available to propose more specific values. In contrast to PCDD and PCDF, PBDD and PBDF are not listed by the Stockholm Convention on POPs. However, their determination is of scientific interest to assess the contribution of brominated dioxins and dibenzofurans to toxic equivalents (TEQ).
Human milk surveys are reviewed in this compendium from various aspects. The general introduction (Part I) gives a review of human milk surveys on POPs (Fürst 2023), an overview of the WHO and United Nations Environment Programme (UNEP) coordinated exposure studies performed between 1987 and 2019 (Malisch et al. 2023a) and a review of the Stockholm Convention on POPs and its implementation by regional and global monitoring reports (Šebková 2023). In Part II, specific analytical aspects are presented, including methods used for determination of PBDE, HBCDD, HBB, and PBDD/PBDF (Schächtele et al. 2023). In various articles of Part III, the analytical results for chlorinated and brominated POPs between 2000 and 2019 are reported and discussed. Part IV includes an assessment of time trends based on these WHO/UNEP-coordinated human milk surveys and is finalized with a review of possible health risks and benefits for the breastfed infant deriving from dioxin-like compounds. Conclusions and key messages are presented in Part V.
A former publication presented the results of the third round of WHO-coordinated exposure studies (2000–2003) and showed that PBDE levels in human milk from the USA were a factor of 35–500 higher than those in other countries. The correlation between PBDE and PBDD/PBDF was assessed (Kotz et al. 2005; Kotz 2006). A comprehensive report for the 6th Conference of the Parties to the Stockholm Convention in 2013 provided an overview on all samples of the three studies spanning the period 2000–2012. It revealed large global differences among various POPs, including PBDE (UNEP 2013).
A global overview on the spatial and temporal trends of Stockholm Convention POPs in breast milk reviews scientific publications between 1995 and 2011. It includes summaries of data for concentrations of PBDE and HBCDD (Fång et al. 2015). The regional and global monitoring reports for the GMP assess datasets in the core media—ambient air, human tissues (human breast milk or blood), and water for hydrophilic POPs, but also other media such as soil, biota, plants are used to support interpretation of observed levels and their trends (UNEP 2022).
All substance-specific data are deposited at the Global Monitoring Plan Data Warehouse (GMP DWH), which can be publicly accessed. This serves as the source of information for the regional and global reports of the GMP and for the evaluation of the effectiveness of the convention to eliminate or reduce emissions of selected POPs (GMP DWH 2020).
In this article, the results for up to 135 pooled samples from up to 80 countries collected between 2000 and 2019 are discussed from various perspectives in the following sections, namely: Sect. 2 General aspects; Sect. 3 Polybrominated diphenyl ethers (PBDE); Sect. 4 Hexabromocyclododecanes (HBCDD); Sect. 5 Hexabromobiphenyl (PBB 153); and Sect. 6 Polybrominated dibenzodioxins and -furans (PBDD/PBDF).
2 General Aspects
2.1 Link to the General Introduction (Countries, UN Regions, Protocol)
An overview of the scope, protocols for collection of samples, expansion of analytes of interest over time by the Stockholm Convention, participation of countries with classification in UN regional groups and temporal differentiation are given in the general introduction in Part I (Malisch et al. 2023a). In brief, the collection of a number of individual samples and preparation of representative pooled samples in all rounds were supervised by a national coordinator in each country following the WHO/UNEP-standardized protocols. Equal aliquots of the individual samples were combined to give a composite sample, which is considered to represent the average levels of POPs for a country or a subpopulation at the time of sampling. The pooled samples were sent to the WHO/UNEP Reference Laboratories for analysis.
In accordance with the implementation of the GMP, parties report through one of the five United Nations regional organization groups. Therefore, countries are classified according to one of these five UN geopolitical groups: (1) African Group, (2) Asia-Pacific Group, (3) Eastern European Group, (4) Group of Latin American and Caribbean Countries (GRULAC), and (5) Western European and Others Group (WEOG). Note that Australia, Israel, New Zealand, and the USA (being informally a member) are included as “Others” in WEOG countries (for participating countries and regional distribution, see Section 6 in Malisch et al. 2023a). It should, furthermore, be noted that these results are not intended to be used for the ranking of individual countries or regions.
2.2 Analysis of Polybrominated Substances
The analytical methods for determination of polybrominated compounds and their validation are presented in Part II (Schächtele et al. 2023). All concentrations are reported on a lipid basis.
2.3 Number of Samples and Aggregation of Data
Due to the particular scope at the beginning of a study with regard to the expansion of analytes of interest over time, a total of 135 pooled samples from 80 countries submitted between 2000 and 2019 were analyzed for PBDE. In the 2000–2003 survey, countries were encouraged to submit at least two pooled samples, whereas in the following rounds, usually one pooled sample was submitted per country. If two or more pooled samples were available for a country in a certain round, the median of the individual results is used for aggregation purposes. This yielded eight median results that are used to represent the country for that round (Australia, 2013; Belgium, 2002; Fiji; 2006; Finland, 2007; Germany, 2002 and 2019; Ireland, 2001; USA, 2003). Thus, for 80 countries (with 36 countries participating repeatedly between 2000 and 2019), 124 “country results” are available for the “one country—one result for a certain period” approach. However, for the time trend analysis, data were not aggregated, and values of all 135 pooled samples were used for time trend analysis. As BDE-209 was not listed until 2017 in the annexes to the Stockholm Convention, only 40 samples from 39 countries submitted in the 2016–2019 period were analyzed for this compound.
In addition, 102 pooled samples from 72 countries collected between 2006 and 2019 were analyzed for the three stereoisomers α-, β-, and γ-HBCCD, 110 pooled samples from 69 countries for hexabromobiphenyl (PBB 153) and furthermore for scientific reasons 38 samples from 28 countries from the period 2001 and 2009 for PBDD/PBDF (not listed by the Stockholm Convention on POPs).
The detailed data for all these samples are included in the POPs Global Monitoring Plan Data Warehouse and can be publicly retrieved (GMP DWH 2020).
2.4 Methods of Statistical Data Treatment for Time Trends of PBDE in Countries with Repeated Participation
For the time trend analysis of PBDE in countries with repeated participation (Sect. 3.2), data were not aggregated. Instead, values of all submitted pooled samples were used for these trend analyses. For methods of statistical data treatment, see the chapter on time trends for PCB, PCDD, and PCDF in Part IV (Malisch et al. 2023c). In brief, the GMP guidance document recommends to apply simple linear regression or the Theil-Sen estimator for power analysis of statistical trends (UNEP 2019). Therefore, the non-parametric linear Theil-Sen trend estimator (Sen 1968; Theil 1992) was used for derivation of the exponential trends as expected after stop of production and application of chemicals (Sharma et al. 2021). This approach is in line with various elimination studies deriving half-lives for PBDE in rodents and humans. A review shows a wide range of elimination half-lives depending on the number of bromine substituents and congener, including a model for serum half-lives of PBDE with 7–10 bromine substituents after exposure of rubber workers and electronic dismantlers (EFSA 2011; Thuresson et al. 2006).
R package “Median-based Linear Models (mblm)” (Komsta 2013) was used for this regression. To prevent biased results in case the kinetics is different to the 1st order exponential decrease, an additional assessment was done considering a case with a small but persistent exposition to the compounds using the PORT method for non-linear regression (Fox 1984). For each trend, its statistical significance was estimated, showing on 95% confidence level whether the trend is not caused by random variance in the data and R2 value was used as an indicative measure of a goodness of fit. In the assessment of temporal trends, improper results can be induced by use of samples from different countries in different times (“Simpson’s paradox” as a statistical phenomenon in which a trend appears in certain groups of data but disappears or reverses when the groups are combined, Simpson 1951). To prevent this, two additional analyses were made: (1) computing of annual decrease rates separately for two decades and comparison of slopes of trends using z-scores (Fisher 1915); (2) deriving the regional or global trend as a median of trends in countries within the region or globally (“median method”).
2.5 Background Concentrations Versus High Concentrations After Exposure
Background concentrations are defined as that portion of the measured human milk levels that is found in the absence of specific sources and therefore not attributable to a known exposure such as use of the chemical of interest or emissions within the study area. In contrast to findings of high concentrations caused by use or emissions of a chemical, considerably lower concentrations might be found for many POPs when its use or emissions have ceased for a longer period of time. These levels are then described as “background levels.”
Reduction rates should be seen in context with the concentration range (levels above or in the range of background contamination): If high levels are found, sources might be detected, which could be reduced or eliminated and would then result in decreasing trends. However, at low background levels, other factors, e.g., contamination of feed and food by air via long-range transport or from subsequent bioaccumulation, cannot be influenced locally. As a possible consequence, concentrations might level out or some fluctuation of calculated decrease rates might be observed.
It should be noted that the term “background level” does not imply per se any level of safety. With respect to potential adverse health effects, subsequent risk assessments need to consider a variety of factors, including the toxicity of the chemical of interest and the concentration found. For human milk, obviously the potential adverse effects have to be balanced against positive health aspects for (breastfed) infant. Such a risk–benefit evaluation of breastfeeding for dioxin-like compounds is included in the assessment chapters in Part IV (van den Berg et al. 2023).
3 Polybrominated Diphenyl Ethers (PBDE)
There are theoretically 209 congeners of polybrominated diphenyl ethers. The most important technical products were composed of a mixture of congeners and were named according to their average bromine content. To avoid confusion, EFSA proposed to use names in capital letters when referring to technical mixtures (e.g., PentaBDE), whereas lowercase letters were used to refer to the homologues itself (e.g., pentaBDE). The three commercial mixtures were: PentaBDE, Octa-BDE, and Deca-BDE (EFSA 2011). These have been produced in the past in large volumes (e.g., volume [metric tons] estimates in 2001: 56,100 t Deca-BDE, 3790 t Octa-BDE, 7500 t Penta-BDE (Birnbaum and Staskal 2004)). PBDE were widely used in polymers and textiles, construction materials, furniture, and electric and electronic equipment. As additive flame retardants, they are not chemically bound to the polymers and can therefore leach into the environment.
The commercial products contained mainly tetra- and pentabromodiphenyl ethers (Penta-BDE), hexa- to nonabromodiphenyl ethers (Octa-BDE) or decabromodiphenyl ether (Deca-BDE) (De Wit 2002; Alaee et al. 2003; La Guardia et al. 2006; EFSA 2011). Tetra-BDE and penta-BDE (as main components of commercial Penta-BDE products [UNEP 2009a]) and hexa-BDE and hepta-BDE (as main components of commercial Octa-BDE products [UNEP 2009b]) were listed under Annex A (for elimination) in the Stockholm Convention in 2009, deca-BDE (as main component of the commercial Deca-BDE mixture) in 2017 also in Annex A (UNEP 2020).
Although there is a large number of theoretically possible isomers as parent compounds, the Guidance Document on the Global Monitoring Plan for POPs recommends only six prevalent analytes (comprising seven congeners) from tetra-BDE to hepta-BDE (BDE-47, BDE-99, BDE-100, BDE-153, BDE-154, BDE-175/183 [co-eluting]) for commercial Penta-BDE and Octa-BDE products, furthermore BDE-209 for Deca-BDE (UNEP 2019) (Table 1).
However, questions were raised whether BDE-175 is an important enough component of commercial octabromodiphenyl ether mixtures to be listed in Annex A of the Stockholm Convention. Since BDE-175 and BDE-183 co-elute on common HRGC columns, the presence of BDE-175 as an important component in technical Octa-BDE mixtures has not been illustrated. The successful HRGC/LRMS separation of a 1:1 mixture of BDE-175 and BDE-183, as well as 1H NMR analysis of technical material, has allowed to confirm that this congener is not present in technical products (Great Lakes DE-79™ and Bromkal 79-8DE™) in quantifiable amounts (Konstantinov et al. 2011). Therefore, the “Guidance Document on the Determination of Organobromine Contaminants for analytical parameters in food and feed” recommends 9 PBDE congeners as analytes of interest: seven congeners covered by the GMP Guidance Document (BDE-47, BDE-99, BDE-100, BDE-153, BDE-154, BDE-183, and BDE-209) and in addition BDE-28 and BDE-49 (EURL for Halogenated POPs in Feed and Food 2022).
As summarizing parameter for human milk samples, the sum of the six recommended PBDE analytes (∑ PBDE6 as sum of BDE-47, BDE-99, BDE-100, BDE-153, BDE-154, and BDE-183, however without consideration of BDE-175) was reported by CVUA Freiburg until in 2017, when BDE-209 was added. The Second Global Monitoring Report uses two kinds of sum parameters for PBDE concentrations in human tissues: (1) for human milk, the sum of the six PBDE analytes is given as “sum 7 PBDEs”; (2) for blood of mothers, the sum of four congeners (sum of BDE-47, BDE-99, BDE-100, and BDE-153) is given (UNEP 2017).
All congeners recommended to be analyzed bioaccumulate in humans (Fürst 2023).
3.1 Sum of Six PBDE Congeners (BDE-47, BDE-99, BDE-100, BDE-153, BDE-154, BDE-183)
Table 2 compiles the most important statistical data (number of samples, minimum, median and maximum) of the sum of the six recommended PBDE congeners in human milk (expressed as ng ∑ PBDE6/g lipid) for the 124 country results (median as one result per country where data for two or more pooled samples for one period are available, see Sect. 2.3) for 80 countries from the five UN Regional Groups. A considerable variation of the PBDE concentrations in human milk in the five periods between 2000 and 2019 was observed, depending on the inclusion of individual countries in a certain round. Of all samples, 80% were in a range below 5 ng ∑ PBDE6/g lipid, including all samples from Africa and the Eastern European Group. The highest concentration of 223 ng ∑ PBDE6/g lipid was found in the 2000–2003 period in the Western European and Others Group (WEOG), followed by 107 ng ∑ PBDE6/g lipid in the Asia-Pacific Group in the 2016–2019 period. The WEOG group comprises Australia, Israel, New Zealand, and the USA as “Others.” Therefore, with regard to the different history of use of PBDE, this UN Regional Group was further split into two subgroups “Western European countries” and “Other countries.” Whereas 21 country results from the subgroup “Western European countries” had ∑ PBDE6 concentrations in the range 0.76–7.72 ng/g, five country results from the subgroup “Other countries” were in the range 5.16–223 ng/g, with highest concentrations in the 2000–2003 period in both subgroups (for a more detailed discussion, see the end of this Sect. 3.1).
Based on the compilation of results in Table 2, a general estimation of time trends is quite difficult. In particular in the Asia-Pacific Group, the Group of Latin American and Caribbean Countries and in the Western European and Others Group, median or maximal concentrations don’t appear to have a continuous downward time trend. The median of all country results shows a decrease of about 50% from the 2.62 ng ∑ PBDE6/g lipid in 2000–2003 period to 1.38 ng ∑ PBDE6/g lipid in the 2016–2019 period. These are seen as current background levels as defined in Sect. 2.5 (found in the absence of specific sources and therefore not attributable to a known exposure). As explained, time trends should be seen in context with the concentration range: If high levels are found, sources might be detected, which could be eliminated. Though, at “background levels”, other factors, e.g., contamination of feed and food by air via long-range transport and subsequent bioaccumulation, cannot be influenced locally. Therefore, conclusions on time trends in the different UN regional groups or globally cannot easily be drawn. Generally, a more precise approach for the assessment of temporal trends is based on consideration of results only from countries with repeated participation in the studies (see Sect. 3.2). For comparison of data in a literature review and conclusions on temporal tendencies, see Fürst (2023) and Fång et al. (2015).
Figure 1 illustrates the country results for the African region. As in the following figures for other regions, the 4-year periods between 2000 and 2019 are shown in different colors; results for Africa are available for the three periods between 2008 and 2019. All countries had at all times ∑ PBDE6 concentrations approximately between 0.5 and 3 ng/g lipid, with quite comparable ranges between the 2008–2011 period (median of 11 samples: 1.60 ng/g lipid, range 0.67–2.83 ng/g) and the 2016–2019 period (median of 15 samples: 1.38 ng/g lipid, range 0.39–2.31 ng/g). For the assessment of time trends in ten countries with repeated participation (Democratic Republic of Congo, Côte d’Ivoire, Ghana, Kenya, Mauritius, Niger, Nigeria, Senegal, Togo, Uganda), see Sect. 3.2.1.

Concentrations of ∑ PBDE6 in human milk from countries in the African Group with submission of samples in three periods between 2008 and 2019 (country results expressed as ng ∑ PBDE6/g lipid)
In the Asia-Pacific Group, most samples had concentrations below 5 ng ∑ PBDE6/g lipid (Fig. 2), in many cases around 0.5–1 ng/g lipid. Five samples from the 2016–2019 period and two samples from earlier periods had significantly higher levels, >5 ng/g lipid, with a maximum of 107 ng ∑ PBDE6/g found in 2019 in the Marshall Islands. For only two countries, data for the assessment of time trends from repeated participation are available (Fiji; Kiribati), see Sect. 3.2.2.

Concentrations of ∑ PBDE6 in human milk from countries in the Asia-Pacific Group with submission of samples in four periods between 2000 and 2019 (country results expressed as ng ∑ PBDE6/g lipid)
Figure 3 illustrates the ∑ PBDE6 results with the period of participation between 2000 and 2019 indicated for Latin American and Caribbean countries. A range between 0.39 ng ∑ PBDE6/g lipid (Uruguay, 2019) and 62.7 ng ∑ PBDE6/g lipid (Haiti, 2011) was found. For the assessment of time trends in eight countries with repeated participation (Antigua and Barbuda, Barbados, Chile, Haiti, Jamaica, Mexico, Peru, and Uruguay), see Sect. 3.2.3.

Concentrations of ∑ PBDE6 in human milk from countries in the Group of Latin American and Caribbean Countries with submission of samples in five periods between 2000 and 2019 (country results expressed as ng ∑ PBDE6/g lipid)
All Eastern European countries had at all times ∑ PBDE6 concentrations approximately between 0.5 and 2 ng/g lipid (Fig. 4). For the assessment of time trends in eight countries with repeated participation (Bulgaria, Croatia, Czech Republic, Georgia, Hungary, Moldova, Romania, and Slovakia), see Sect. 3.2.4.

Concentrations of ∑ PBDE6 in human milk from countries in the Eastern European Group with submission of samples in five periods from 2000 to 2019 (country results expressed as ng ∑ PBDE6/g lipid)
As explained above, the Western European and Others Group (WEOG) includes Australia, Israel, New Zealand, and the USA (being informally a member) as “Others” (see section “regional distribution” in Malisch et al. 2023a). In the period 2000–2003, ∑ PBDE6 concentrations in human milk from Western European countries were in the range between 2.0 ng/g lipid (Belgium, 2002) and 7.7 ng/g lipid (Ireland, 2001), with downward trends until the 2016–2019 period (range between 0.76 ng/g lipid [Germany, 2019] and 1.73 ng/g lipid [Ireland, 2019]). In New Zealand, Australia, and Israel the ∑ PBDE6 concentrations were in the range between 5.16 ng/g lipid (New Zealand, 2011) and 11.8 ng/g lipid (Australia, 2002). As highest ∑ PBDE6 concentration observed in all countries between 2000 and 2019, 223 ng ∑ PBDE6/g lipid was the country result for samples collected in 2003 in the USA (as median of two pooled samples from North Carolina [92.6 ng/g lipid] and in California [352 ng/g lipid]) (Fig. 5).

Concentrations of ∑ PBDE6 in human milk from countries in the Western European and Others Group with submission of samples in five periods from 2000 to 2019 (country results expressed as ng ∑ PBDE6/g lipid)
These findings of the high PBDE levels in human milk from the USA in 2003 are in line with reports that levels of PBDE in US residents were 3–25 times higher than those of individuals in Europe at that time. The levels of PBDE in human tissue samples from California women were the highest reported then. The high PBDE levels (up to 462 ng/g lipid for the sum of 5 PBDE [BDE-47, BDE-99, BDE-100, BDE153, and BDE-154] in human breast adipose tissues) could be partially explained by the fact that California regulations required all furnishings to pass flammability tests for fire safety (She et al. 2002). The presence of few samples with unusually high PBDE levels in human milk from the Pacific Northwest of the US and Canada suggested, as did a number of other studies of human blood (e.g., Petreas et al. 2003), that the frequency of high (>300 ng/g lipid) levels for the sum of 12 PBDE was greater than predicted by a lognormal distribution (She et al. 2007). These 12 PBDE comprised the five most important congeners of the 2002 study, which made up about 90–95% of the sum of 12 PBDE. The other seven congeners were BDE-28, BDE-32, BDE-66, BDE-71, BDE-85, BDE-183, and BDE-209. The sum of the six recommended analytes (BDE 47, BDE-99, BDE-100, BDE-153, BDE-154, and BDE 175/183 [co-eluting]) and the sum of these six PBDE plus BDE-209 (UNEP 2019) was nearly the same as the sum of the five congeners (median contribution to the sum of 12 PBDE: ∑ PBDE5 92.4%; ∑ PBDE6 93.0%; ∑ PBDE6+BDE-209 94.0%). Thus, the recommended analytes cover most of ∑ PBDE12; the remaining ones represent very low levels.
The determination of up to 13 PBDE in 47 individual human milk samples from nursing mothers in the USA found a variation of the concentrations of the sum of PBDE congeners from 6.2 to 419 ng/g lipid. These findings showed extremely elevated levels (10–100 times) in many participants compared with contemporaneous studies reported in Europe. Comparing the legal situation at that time, it was noted that use of PBDE was permitted in the USA but had already been restricted in some European countries (Schecter et al. 2003).
California flammability standards became common for residential, business, and institutional upholstered furniture across North America. The flame retardant primarily used in polyurethane furniture foam through the mid-2000s was Penta-BDE. The use of Penta-BDE was banned in the European Union in 2004 and discontinued in the USA in 2005. In 2009, tetra-BDE and penta-BDE were added to the Stockholm Convention on POPs. By the time of these restrictions, millions of kilograms of Penta-BDE had been applied to upholstered furniture in order to meet flammability standards (Charbonnet et al. 2020). For a review of the exposure of Americans to PBDE at that time, see Lorber (2008), for discussion of toxicological concerns, see Birnbaum and Staskal (2004), and for decreasing PBDE levels in breast milk in California after implementation of new governmental regulatory policies on PBDE, see Guo et al. (2016). In view of the high amounts of PBDE produced commercially as flame retardants in combination with their environmental persistence, it can be expected that much of these PBDE may still be released into the environment in the near future as a result of disposal when the products containing them reach their end of life.
3.2 Temporal Tendencies for the Sum of Six PBDE Congeners Derived from Countries with Repeated Participation
One of the objectives of the WHO/UNEP-coordinated human milk exposure studies was to generate comparable and consistent monitoring data on the presence of these POPs in order to identify trends in levels. To provide reliable monitoring information for the Parties to the Stockholm Convention, as a quantitative objective for temporal studies The Guidance Document on the Global Monitoring Plan (GMP) proposed the ability to detect a 50% decrease in the levels of POPs within a 10-year period. However, there is no stipulation of a quantitative goal for the rate of decline in POPs levels. Clearly, the Convention’s objectives are either to eliminate or to reduce production, use and releases, depending on the annex where a chemical is listed, but the rate of the decline is nowhere specified or required (UNEP 2015, 2019).
For assessment of this goal, the exponential trends calculated by the Theil-Sen method comprise the overall decrease rates per 10 years. Trends can be derived if the trend test (significance of the Theil-Sen estimator) is positive on 95% confidence level of significance (i.e., p-values < 0.05). As simulations show that Theil-Sen p is never below 0.05 for fewer than 5 data points and as for most countries fewer than 5 data points were available, statistically significant trends could be derived only for few countries and for most UN regions (combining data from countries). If the minimum of five data points is not available allowing to derive statistically significant temporal trends, the existing data can indicate decreasing or increasing tendencies in POP concentrations.
To minimize possible sources of variation for time trend analysis of POPs, the concept of the WHO/UNEP-coordinated exposure studies has two basic elements: (1) preparation of pooled samples from a number of individual samples considered to be representative for a country or region/subgroup; (2) analysis by a reference laboratory.
The above Sect. 3.1 shows a considerable variation of the PBDE concentrations in human milk from 80 countries in the five periods between 2000 and 2019, depending on the inclusion of the individual countries in a certain round. As a result, a general estimation of time trends among the different UN regional groups and globally is difficult from a statistical point of view. Therefore, the following temporal trends are assessed based on results only from countries with a repeated participation in the different surveys. For 36 of the 80 countries, PBDE data for 90 pooled samples from participation in two or more rounds are available for this purpose. As explained above, time trends should be seen in context with the concentration range: If high levels are found, sources might be detected, which could be eliminated. In the range of background contamination, other factors cannot be influenced locally, and the concentrations might fluctuate over time.
3.2.1 African Group
As shown above in Sect. 3.1, all African countries always had ∑ PBDE6 concentrations in the range of background contamination, approximately between 0.5 and 3 ng/g lipid, with quite comparable ranges between the 2008–2011 period and the 2016–2019. Figure 6 (for aggregated data) shows the variation over time at these background levels for ten countries with data for two sampling periods. Figure 7 (comprising all individual pooled samples) shows the resulting Theil-Sen exponential time trends for the African Group. The overall decrease rates (%) per 10 years are compiled in Table 3. All temporal tendencies were statistically not significant, as well for the countries as the regional trend derived by pooling of the individual samples from all countries.

Overview of the changes in ∑ PBDE6 concentrations (ng ∑ PBDE6/g lipid) over time in African countries with repeated participation between 2000 and 2019

Theil-Sen exponential trends of ∑ PBDE6 concentrations in human milk of countries in the African Group (ng ∑ PBDE6/g lipid). The thick lines in the middle show the median value, the whiskers show 5th and 95th percentiles
In Fig. 7, results are shown on annual basis for the period 2008–2019, Fig. 6 uses 4-year periods, and Table 3 presents data for decrease (or increase as negative results) over 10 years. The annual basis in Fig. 7 combines different numbers of samples for the respective years, e.g. one sample in 2008 (2.32 ng/g), six samples in 2009 (range 0.96–2.83 ng/g), two samples in 2015 (1.10 ng/g; 1.20 ng/g) or three samples in 2019 (range 1.45–2.25 ng/g). The time interval between first and last participation illustrated in Fig. 6 covers a range between 5 years (Côte d’Ivoire, 2010 and 2015) and 10 years (Nigeria, 2008 and 2018), which is normalized into tendencies over 10 years as presented in Table 3. Therefore, a direct comparison of results of Table 3 with the illustrations in Figs. 6 and 7 is difficult.
As a conclusion for the African Group, ∑ PBDE6 concentrations fluctuate over time at background levels, but remained constantly in this low range. Overall rates over 10 years can be calculated for individual countries but are of little relevance in cases where background levels might be leveling out. This conclusion is more clearly visualized in Fig. 7.
3.2.2 Asia-Pacific Group
Some countries of the Asia-Pacific group did not participate repeatedly. In addition, some countries of the Pacific region did not send sufficient sample amounts necessary for the application of the various analytical methods to be applied: There is no multi-method for simultaneous determination of all POPs of interest for the Stockholm Convention that could limit the total amount of human milk needed for this combined POPs analysis. Consequently, PBDE data for assessment of time trends are available only for two countries (Fiji and Kiribati). Figure 8 shows the results for these two countries; Fig. 9 visualizes the summarizing time trend; and Table 4 lists the decrease rates over 10 years.

Overview of the changes in ∑ PBDE6 concentrations (ng ∑ PBDE6/g lipid) over time in countries of the Asia-Pacific Group with repeated participation between 2000 and 2019

Theil-Sen exponential trends of ∑ PBDE6 concentrations in human milk of countries in the Asia-Pacific Group (ng ∑ PBDE6/g lipid). The thick lines in the middle show the median value, the whiskers show 5th and 95th percentiles
For Fiji, results from four periods (with two samples submitted in 2006) are available showing a continuous downwards trend from 2002 (7.2 ng ∑ PBDE6/g) to 2019 (1.5 ng ∑ PBDE6/g). These five available data allow to determine a statistically significant decrease rate for Fiji, whereas the two samples sent by Kiribati in 2006, respectively, 2019 do not allow to derive statistically significant decrease rates. Based on these seven results from these two countries, statistically significant group rates can be calculated—however, certainly, more results from more countries would be necessary before conclusions for the whole Asia-Pacific Group can be drawn.
3.2.3 Group of Latin American and Caribbean Countries (GRULAC)
Figure 10 illustrates the time trends of ∑ PBDE6 concentrations in human milk of eight Latin American and Caribbean countries, Fig. 11 for this UN region.

Overview of the changes in ∑ PBDE6 concentrations (ng ∑ PBDE6/g lipid) over time in Latin American and Caribbean countries with repeated participation between 2000 and 2019

Theil-Sen exponential trends of ∑ PBDE6 concentrations in human milk of countries in the Group of Latin American and Caribbean Countries (ng ∑ PBDE6/g lipid). The thick lines in the middle show the median value, the whiskers show 5th and 95th percentiles
In Haiti, the ∑ PBDE6 concentrations before 2011 (in 2004 with 21.9 ng/g lipid) and after 2011 (in 2015 with 7.4 ng/g lipid) were considerably lower than the maximum found in the 2011 sample (62.7 ng/g lipid). The increasing trend from 2004 to 2011 and decreasing trend to 2019 might be discussed with the voluntarily withdrawal of Penta-BDE and Octa-BDE formulations from the US marketplace by their manufacturers at the end of 2004 as a result of findings of high ∑ PBDE6 concentrations in human milk from the USA (see results and discussion of “Western European and Others Group” in Sect. 3.1). Therefore, the up and down in Haiti might be explainable with the delay, before the withdrawal of penta- and octa-BDE from the US marketplace became effective.
Downtrends from the 2008–2011 period to the 2016–2019 period were observed in Antigua and Barbuda, Barbados, Chile, Jamaica, and Mexico. In Peru, ∑ PBDE6 remained quite constant around 1.5 ng/g lipid and in Uruguay around 0.5 ng/g lipid.
Table 5 compiles the decrease rates for 10 years. The limited number of samples did not allow to determine statistically significant time trends for countries. Furthermore, for the three countries below 3 ng ∑ PBDE6/g lipid in all periods (Chile, Peru and Uruguay), the calculated decrease rates have a wide variation due to the fluctuation near background levels, as concluded already for African countries (Sect. 3.2.1). For the Group of Latin American and Caribbean Countries, the decrease rate over 10 years of nearly 50% is statistically significant.
3.2.4 Eastern European Group
As shown above in Sect. 3.1, all Eastern European countries had at all times ∑ PBDE6 concentrations in the range of background contamination approximately between 0.5 and 2 ng/g lipid. Figure 12 illustrates the time trends of ∑ PBDE6 concentrations in human milk of eight Eastern European countries with repeated participation (Bulgaria, Croatia, Czech Republic, Georgia, Hungary, Moldova, Romania, and Slovakia); Fig. 13 for this UN region; and Table 6 compiles the decrease rates for 10 years. Due to limited data, the country-specific results are statistically not significant, however, pooling of the samples allows a trend for this group to be determined.

Overview of the changes in ∑ PBDE6 concentrations (ng ∑ PBDE6/g lipid) over time in countries of the Eastern European Group with repeated participation between 2000 and 2019

Theil-Sen exponential trends of ∑ PBDE6 concentrations in human milk of countries in the Eastern European Group (ng ∑ PBDE6/g lipid). The thick lines in the middle show the median value, the whiskers show 5th and 95th percentiles
As a conclusion, the ∑ PBDE6 concentrations tend to fluctuate at near background levels, but remain constant in this low range. For the Eastern European Group, the statistically significant decrease rate over 10 years was 15%.
3.2.5 Western European and Others Group (WEOG)
Figure 14 illustrates the time trends of ∑ PBDE6 concentrations in human milk of eight countries of the Western European and Others Group (WEOG) and Fig. 15 for this UN regional group. Table 7 compiles the decrease rates for 10 years.

Overview of the changes of ∑ PBDE6 concentrations (ng ∑ PBDE6/g lipid) over time in countries of the Western European and Others Group with repeated participation between 2000 and 2019

Time trends of ∑ PBDE6 concentrations in human milk of countries of the Western European and Others Group using the Theil-Sen method (ng ∑ PBDE6/g lipid). The thick lines in the middle show the median value, the whiskers show 5th and 95th percentiles
As shown above in Sect. 3.1, the two highest ∑ PBDE6 concentrations were found in the 2000–2003 period in the USA (223 ng/g lipid as median of two samples) and then in Australia (11.8 ng/g lipid). Unfortunately, time trends for the highest PBDE concentration could not be derived from WHO/UNEP-coordinated exposure studies, as the USA has not participated after 2003 again. However, significant declines in PBDE levels between 2003–2005 and 2009–2012 were found in breast milk of California women: The concentration of the sum of PBDE (Ʃ10PBDE = sum of BDE-28, -47, -66, -85, -99, -100, -153, -154, -183, and -209) over the ~7 year course declined by 39% (GeoMean = 67.8 ng/g lipid in 2003–2005; 41.5 ng/g lipid in 2009–2012) (Guo et al. 2016). In Australia, ∑ PBDE6 concentrations in human milk decreased by 53% between 2002 and 2013.
Western European countries were in the range between 2.0 and 7.7 ng/g lipid. For four Western European countries, data are available for the 2000–2003 period as well as the 2004–2007 period (Belgium, Finland, Luxembourg, and Sweden). Over this time, the ∑ PBDE6 concentrations remained quite constant. In comparison with these two periods, downward trends were observed afterward to the 2012–2015 and 2016–2019 surveys in all countries participating in these periods (Fig. 14). These observations are in line with the legal situation in the EU: A directive of the European Parliament and the Council of 2003 restricted the concentration of penta-BDE and octa-BDE in articles to 0.1% and entered into force in 2004 (Directive 2003/11/EC).
Due to lack of sufficient data, for most countries the decrease rates over 10 years for countries are statistically not significant (Table 7). Statistically significant is the decrease rate over 10 years of 60% in Germany and of 48% for this group of countries.
3.2.6 Global Level
The exponential trends of ∑ PBDE6 concentrations in human milk derived by the Theil-Sen method worldwide are illustrated in Fig. 16. At the global level calculated from 36 countries, the statistically significant overall decrease rate per 10 years was 32% calculated by the Theil-Sen method, respectively, 48% by the median method (Table 8).

Global time trends of ∑ PBDE6 concentrations in human milk using the Theil-Sen method (ng ∑ PBDE6/g lipid). The thick lines in the middle show the median value, the whiskers show 5th and 95th percentiles
3.3 Decabromodiphenyl Ether (BDE-209)
As explained in the introduction chapter, the number of target analytes in the global human milk studies gradually expanded as new POPs were listed in the annexes of the Stockholm Convention. BDE-209 was listed in 2017 and included in the analysis of human milk samples for the 2016–2019 period (Malisch et al. 2023a).
BDE-209 concentrations in 40 pooled human milk samples from 39 countries in this period were in the range between <0.06 and 5.92 ng/g, with a median of 0.21 ng/g and a 90%-percentile of 1.53 ng/g. The median of the contribution of BDE-209 to the sum of 7 PBDEs (∑ PBDE7 = ∑ PBDE6 + BDE-209) was 13% but ranged from 3 to 66% (75% quantile: 21%). This large difference in contribution of BDE-209 to ∑ PBDE7 could possibly be explained by the difference in local production and use of different commercial PBDE mixtures as flame retardants.
In nearly all 14 countries from Africa, the BDE-209 concentrations were below 0.4 ng/g lipid, in these cases with a contribution between 6 and 29% to ∑ PBDE7. As maximum, 1.51 ng BDE-209/g lipid was found in Tunisia exceeding the ∑ PBDE6 concentration. In these 14 countries, ∑ PBDE6 levels were in the range of background contamination between 0.39 and 2.31 ng/g lipid (Fig. 17).

Concentration of BDE-209 and ∑ PBDE6 in human milk from countries in the African Group for the period 2016–2019 (expressed as ng ∑ PBDE6/g lipid and ng BDE-209/g lipid, respectively)
In four Asian countries of the Asia-Pacific Group, the BDE-209 concentrations were below 0.3 ng/g lipid; with ∑ PBDE6 levels in the range of background contamination below 1 ng/g lipid. With increasing ∑ PBDE6 levels in the Pacific region, also higher BDE-209 concentrations were found, with a maximum of 5.92 ng BDE-209/g lipid in Marshall Islands, contributing 5% to ∑ PBDE7 (113 ng/g lipid). In Palau, BDE-209 results (3.31 ng/g lipid) contributed 18% to ∑ PBDE7 (15.3 ng/g lipid) (Fig. 18).

Concentration of BDE-209 and ∑ PBDE6 in human milk from countries in the Asia-Pacific Group for the period 2016–2019 (expressed as ng ∑ PBDE6/g lipid and ng BDE-209/g lipid, respectively)
In most Latin American and Caribbean countries, BDE-209 concentrations were below 1 ng/g lipid; with a maximum of 2.4 ng BDE-209/g lipid in Peru. ∑ PBDE6 levels were in the range of background contamination below 2 ng/g lipid in five countries; the maximum ∑ PBDE6 concentration was found in Antigua-Barbuda (13.8 ng ∑ PBDE6/g lipid) with BDE-209 levels below the limit of quantification (<0.06 ng/g lipid) (Fig. 19).

Concentration of BDE-209 and ∑ PBDE6 in human milk from countries in the Group of Latin American and Caribbean countries for the period 2016–2019 (expressed as ng ∑ PBDE6/g lipid and ng BDE-209/g lipid, respectively)
In nearly all European countries, the BDE-209 concentrations were below 0.3 ng/g lipid. As maximum, 0.88 ng BDE-209/g lipid was found in Austria (41% of ∑ PBDE7). The ∑ PBDE6 levels were in the range of background contamination between 0.49 and 1.73 ng/g lipid (Fig. 20).

Concentration of BDE-209 and ∑ PBDE6 in human milk from European countries for the period 2016–2019 (expressed as ng ∑ PBDE6/g lipid and ng BDE-209/g lipid, respectively)
3.4 Congener Patterns
Within the group of the recommended six analytes, generally, BDE-47 showed the highest contribution to the ∑ PBDE6 (49% as median of the five UN Regional Groups; range 16–73% in 134 pooled samples from 79 countries), followed by BDE-153 (21% as median of the five UN Regional Groups; range 4–55%), then BDE-99 (median 13%, range 7–35%) and BDE-100 (median 10%; range 6–20%). BDE-154 and BDE-175/183 contributed on average (as median) about 2% (for relevance of BDE-175 in this co-eluting pair and confirmation that BDE-175 is not present in technical products in quantifiable amounts, see discussion above in the introduction to Sect. 3 with reference to Konstantinov et al. 2011) (Fig. 21).

Contribution (%) of 6 PBDE analytes to ∑ PBDE6 in human milk from five UN Regional Groups (median of countries of the region)
In the period 2016–2019, in addition to the six recommended analytes and BDE-209, 18 other congeners were included in the analysis of 40 samples from 39 countries to cover a broader range (BDE-15, BDE-17, BDE-28, BDE-49, BDE-66, BDE-75; BDE-77; BDE-85; BDE-119; BDE-126; BDE-138; BDE-190; BDE-196; BDE-197; BDE-203; BDE-206; BDE-207; BDE-208). Whereas BDE-28 and BDE-49 were included in EURL proficiency test, the other additional congeners were not included in any proficiency tests, and therefore are currently not validated with the same degree of quality control as the seven recommended analytes (Schächtele et al. 2023). However, results can give a first provisional indication whether other congeners might be of interest in addition to the seven congeners recommended by the guidance document (UNEP 2019). PBDE congeners up to hepta-brominated congeners were determined at relatively low levels in comparison with the recommended six analytes, if exceeding the range of the limit of quantification at all. However, the octa-BDE 197 and nona-BDE 206, 207, and 208 should be considered as possible recommended analytes in human milk in future activities: The contribution of these analytes to ∑ PBDE25 was in the range of the six recommended analytes and BDE-209 (Fig. 22). These findings might be explained by suggestion of reductive debromination to nona- and octa-BDEs as the likely first step in the metabolism of BDE-209, with formation of BDE-206, BDE-207, and BDE-208 in the metabolic pathways as prerequisite for the formation of hydroxynona-BDE metabolites (EFSA 2011). The accumulation of higher brominated PBDEs in lactating cows was shown for BDE-196, BDE-197, and BDE-207, suggesting a metabolic debromination of BDE-209 to these BDEs (Kierkegaard et al. 2007). In human milk from China, BDE-209 a as congener considered to have less bioavailability was detected in about 50% of the samples at concentrations higher than that of other congeners. Other higher brominated congeners, including BDE-197 and BDE-207, were also prominent (Sudaryanto et al. 2008). Additionally, see the review on findings of POPs in human milk (Fürst 2023).

Provisional assessment of the median contribution (%) of 25 di- to deca-BDE congeners to ∑ PBDE25 in human milk in 39 countries from the five UN Regional Groups
4 Hexabromocyclododecanes (HBCDD)
Technical products of hexabromocyclododecane contain predominantly the three stereoisomers α-HBCDD, β-HBCDD, and γ-HBCDD, although other stereoisomers are theoretically possible. Whereas γ-HBCDD is the main compound in technical HBCDD, α-HBCDD is more persistent in the environment and biota, including humans (for literature review, see Fürst 2023 and Fång et al. 2015). This is possibly due to differences in persistence, or because of transformation processes (EFSA 2021).
The α-HBCDD levels of 102 pooled samples from 72 countries collected between 2006 and 2019 ranged between <0.1 and 15 ng/g lipid (median: 0.5 ng/g lipid; 90% of all results below 2 ng/g lipid). β-HBCDD and γ-HBCDD were in nearly all samples below the limit of quantification (LOQ for 90% of the samples: <0.1 ng/g lipid) or around the LOQ (max: 0.8 ng/g lipid). As a consequence, α-HBCDD is the predominant stereoisomer in human milk. Therefore, the sum parameter “sum of the three stereoisomers” is in close agreement with the α-HBCDD concentrations only: The lower bound “sum of the three stereoisomers” (where non-detects = 0) ranged between 0 and 15.7 ng/g lipid (median: 0.5 ng/g lipid; 90% of all results below 2.0 ng/g lipid) and the upper bound sum (where non-detects = limit of quantification) between 0.2 and 15.8 ng/g lipid (median: 0.7 ng/g lipid; 90% of all results below 2.4 ng/g lipid).
In all countries of the African Group (Fig. 23), the Asia-Pacific Group (Fig. 24) and the Group of Latin American and Caribbean Countries (Fig. 25), the α-HBCDD levels were in all surveys below 2 ng/g lipid. In the Eastern European Group (Fig. 26), five out of seven countries had α-HBCDD levels above 2 ng/g lipid in the 2012–2015 period, with a maximum of 15 ng/g lipid in Romania (2014). In Georgia and Moldova, the α-HBCDD increased from the 2008–2011 period (Georgia: 1.3 ng/g lipid; Moldova: 2.8 ng/g lipid) to the 2012–2015 period (Georgia: 4.0 ng/g lipid; Moldova: 8.0 ng/g lipid). In Czechia, the α-HBCDD concentration remained constant at 1.0 ng/g lipid between 2014 and 2019. In nearly all samples from countries of the Western European and Others Group (Fig. 27), the α-HBCDD concentration was below 2 ng/g lipid. The maximum level was from a sample from Austria (2016) that had a concentration of 5.6 ng/g lipid.

Concentration of α-HBCDD in human milk from countries of the African Group (ng/g lipid)

Concentration of α-HBCDD in human milk from countries of the Asia-Pacific Group (ng/g lipid)

Concentration of α-HBCDD in human milk from countries of the Group of Latin American and Caribbean Countries (ng/g lipid)

Concentration of α-HBCDD in human milk from Eastern European countries (ng/g lipid)

Concentration of α-HBCDD in human milk from countries of the Western European and Others Group (ng/g lipid)
It is not possible to derive a temporal tendency: In all non-European countries with repeated participation, α-HBCDD concentrations tend to fluctuate at near background levels below 1–2 ng/g lipid seeming partly to decrease, partly to remain quite constant or partly to increase until the 2016–2019 period. In two Eastern European countries with repeated participation until the 2012–2015 period, temporal tendencies seemed to increase up to 8 ng/g lipid. As explained for PBDE, overall decrease rates as proposed for the ability of temporal studies to detect time trends for the effectiveness evaluation can be calculated for individual countries, but are of little relevance in cases, when background levels might have leveled out over time. More data for countries with levels above 2 ng α-HBCDD/g lipid would be necessary to derive reliable time trends for the comparably higher concentration range.
5 Hexabromobiphenyl (PBB 153)
Hexabromobiphenyl comprises 42 isomers in one homolog group; PBB 153 is the recommended analyte (UNEP 2019). PBB 153 concentrations were below the limit of quantification (0.5 ng/g lipid) in 106 of 110 pooled samples from 69 countries. In four samples, low concentrations between 1.0 and 1.7 ng/g lipid were found.
6 Polybrominated Dibenzodioxins and Furans (PBDD/PBDF)
Thermal stress (waste combustion or accidental fires) of PBDE may result in formation of polybrominated dibenzodioxins and -furans (PBDD/PBDF congeners) or mixed brominated-chlorinated dibenzo-p-dioxins and dibenzofurans (PXDD/PXDF). Consequently, the use of PBDE as brominated flame retardants raised concern regarding environmental releases of brominated or mixed brominated-chlorinated dioxins and furans. Thus, for scientific reasons 38 samples from 28 countries collected between 2001 and 2009 were analyzed for PBDE (listed by the Stockholm Convention on POPs) as well as PBDD and PBDF (not listed by the Convention). Moreover, polychlorinated dibenzo-p-dioxins (PCDD) and polychlorinated dibenzofurans (PCDF) (both listed by the Convention) were also measured in these human milk samples. The analyses of these brominated as well as chlorinated analogs provided the possibility to determine the contribution of PBDD and PBDF to the total amount of TEQ.
The same toxic equivalency factors (TEF) as derived by an WHO expert meeting in 2005 (WHO-TEFs [2005]) for PCDD and PCDF (Van den Berg et al. 2006) were also applied for PBDD/PBDF congeners (Kotz et al. 2005; Kotz 2006), as recommended as an interim approach (van den Berg et al. 2013). For more details of these TEF schemes and calculation of toxic equivalents as WHO-TEQ as “upper bound” (where non-detects = limit of quantification) and “lower bound” concentrations (where non-detects = 0), see Malisch et al. 2023b.
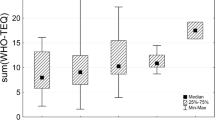
An overview of the results and the ratios between WHO-PBDD/PBDF-TEQ and WHO-PCDD/PCDF-TEQ are presented in Table 9. The differences between lower bound and upper bound WHO-PCDD/PCDF-TEQ concentrations are negligible (Malisch et al. 2023b). However, the considerably lower concentrations of the brominated compounds resulted in more cases of congeners below the limit of quantification, which causes higher upper bound values for WHO-PBDD/PBDF-TEQ and thus higher differences between lower and upper bound values. Then, for risk assessment, the application of the upper bound concentrations leads to an overestimation of the intake, the application of the lower bound concentrations to an underestimation of the intake. For these cases, the application of a “middle bound” TEQ concentration was recommended by the Joint FAO/WHO Expert Committee on Food Additives (JECFA) (Canady et al. 2002). Therefore, in addition also middle bound values are given for this parameter.
On average WHO-PBDD/PBDF-TEQ provided about 10% to the total amount of WHO-TEQ for both groups (chlorinated and brominated) of analogs combined. In view of this limited contribution of PBDD and PBDF to the total amount of WHO-TEQs, the risk–benefit analysis as done for the PCDD and PCDF (van den Berg et al. 2023) will only be influenced marginal and not change the main conclusions significantly.
Figure 28 compares levels of PBDD/PBDF and PCDD/PCDF (expressed as WHO-TEQ) with PBDE concentrations: Samples are sorted with ∑ PBDE6 concentrations increasing from about 1 to 350 ng/g lipid, however, no correlations between PBDE and PBDD/PBDF or between PBDD/PBDF and PCDD/PCDF were found: The PBDD/PBDF levels in two human milk samples from the USA with highest PBDE concentrations (93 respectively 352 ng ∑ PBDE6/g lipid; 0.58, respectively, 0.61 pg WHO-PBDD/PBDF-TEQ/g lipid, UB) were comparable to the other countries within the same order of magnitude (median of all samples: 0.77 pg WHO-PBDD/PBDF-TEQ/g lipid, UB; range 0.12–1.58 pg/g), although the PBDE concentrations exceeded the levels in most other countries by two orders of magnitude.

The mixed brominated-chlorinated PXDD/PXDF pose a particular challenge: Of the theoretically possible 4600 congeners, there are 984 2,3,7,8-substituted compounds alone, among them the toxicologically most interesting tetra- and penta-substituted PXDD/PXDF congeners. Four 2,3,7,8-substituted TXDD (a total of 254 congeners) and eight TXDF (a total of 496 congeners) can theoretically occur. Among the penta-substituted ones, there are already twenty 2,3,7,8-PeXDD (420 in total) and forty PeXDF (480 in total). As only 2,3,7,8-substituted PCDD and PCDF are found in humans at the end of the food chain, it can be assumed that if PXDD/PXDF are detected in the human milk samples, they are only 2,3,7,8-substituted congeners. However, already the very limited number of standards restricts the specific determination of the individual 2,3,7,8-substituted congeners significantly, apart from analytical problems, e.g., chromatographic separation. Therefore, it was checked whether tetra- and penta-substituted PXDD/PCDF could be detected at all in any of the human milk samples tested. However, they could not be detected in any sample. The limit of quantification of 0.05 pg/g fat for the TXDD/TXDF and PeXDD/PeXDF congeners was comparable to those of PBDD/PCDF. The calculation of the “WHO-PXDD/PXDF-TEQ” is not meaningful if too many congeners are not detectable (Kotz et al. 2005; Kotz 2006).
References
Alaee M, Arias P, Sjödin A, Bergman A (2003) An overview of commercially used brominated flame retardants, their applications, their use patterns in different countries/regions and possible modes of release. Environ Int 29:683–689
Birnbaum LS, Staskal DF (2004) Brominated flame retardants: cause for concern? Environ Health Perspect 112:9–17
Canady R, Crump K, Feeley M, Freujer J, Kogevinas M, Malisch R, Verger P, Wilson J, Zeilmaker M (2002) Polychlorinated dibenzodioxins, polychlorinated dibenzofurans and coplanar biphenyls. WHO Food Additives Series 48 “Safety evaluation of certain food additives and contaminants, prepared by the fifty-seventh meeting of the Joint FAO/WHO Expert Committee on Food Additives (JECFA)”. IPCS (International Programme on Chemical Safety), World Health Organization, Geneva, pp 451–664
Charbonnet JA, Weber R, Blum A (2020) Flammability standards for furniture, building insulation and electronics: benefit and risk. Emerg Contam. https://doi.org/10.1016/j.emcon.2020.05.002
De Wit CA (2002) An overview of brominated flame retardants in the environment. Chemosphere 46:583–624
Directive 2003/11/EC of the European Parliament and of the Council of 6 February 2003 amending for the 24th time Council Directive 76/769/EEC relating to restrictions on the marketing and use of certain dangerous substances and preparations (pentabromodiphenyl ether, octabromodiphenyl ether). Offic J Eur Union L42/45
EFSA (2011) Scientific opinion on polybrominated diphenyl ethers (PBDE) in food. EFSA Panel on Contaminants in the Food Chain. EFSA J 9(5):2156
EFSA (2021) Update of the risk assessment of hexabromocyclododecanes (HBCDDs) in food. EFSA J 19(3):6421. https://doi.org/10.2903/j.efsa.2021.6421
EURL for Halogenated POPs in Feed and Food (2022) Guidance document on the determination of organobromine contaminants (version 1.1 of 20 April 2022). https://eurl-pops.eu/news/guidance-document-bcon-parameters/guidance-document-bcon-parameters-2
Fång J, Nyberg E, Winnberg U, Bignert A, Bergman A (2015) Spatial and temporal trends of the Stockholm Convention POPs in mothers’ milk—a global review. Environ Sci Pollut Res 22:8989–9041
Fisher RA (1915) Frequency distribution of the values of the correlation coefficient in samples from an indefinitely large population. Biometrika 10:507. https://doi.org/10.2307/2331838
Fox PA (1984) The PORT mathematical subroutine library
Fürst P (2023) Human milk surveys on persistent organic pollutants from a historical perspective. In: Malisch R, Fürst P, Šebková K (eds) Persistent organic pollutants in human milk. Springer, Cham (in this volume, Part I)
GMP DWH (2020) Global monitoring plan data warehouse of the Stockholm Convention on Persistent Organic Pollutants: visualisation platform and on-line tool for the analysis of global levels of POPs in air, water, breast milk and blood, online at http://www.pops-gmp.org (Hůlek R, Borůvková J, Kalina J, Bednářová Z, Šebková K, Hruban T, Novotný V, Ismael M, Klánová J, Masaryk University)
Guo W, Holden A, Smith SC, Gephart R, Petreas M, Park JS (2016) PBDE levels in breast milk are decreasing in California. Chemosphere 150:505–513
Kierkegaard A, Asplund L, de Wit CA, McLachlan MS, Thomas GO, Sweetman AJ, Jones KC (2007) Fate of higher brominated PBDEs in lactating cows. Environ Sci Technol 41(2):417–423
Komsta Ł (2013) Package ‘mblm’
Konstantinov A, Chittim B, Potter D, Klein J, Riddell N, McCrindle R (2011) Is BDE-175 an important enough component of commercial octabromodiphenyl ether mixtures to be listed in Annex A of the Stockholm Convention? Chemosphere 82:778–781. https://doi.org/10.1016/j.chemosphere.2010.11.016
Kotz A (2006) Bestimmung von bromierten und gemischt bromiert-chlorierten Umweltkontaminanten in biologischen Matrizes mit HRGC-HRMS. Inauguraldissertation, Universität Basel
Kotz A, Malisch R, Kypke K, Oehme M (2005) PBDE, PBDD/F and mixed chlorinated-brominated PXDD/F in pooled human milk samples from different countries. Organohalogen Comp 67:1540–1533
La Guardia MJ, Hale RC, Harvey E (2006) Detailed polybrominated diphenyl ether (PBDE) congener composition of the widely used penta-, octa-, and deca-PBDE technical flame-retardant mixtures. Environ Sci Technol 40:6247–6254
Lorber M (2008) Exposure of Americans to polybrominated diphenyl ethers. J Expo Sci Environ Epidemiol 18:2–19
Malisch R, Malisch K, van Leeuwen FXR, Moy G, Tritscher A, Witt A, Alvarez J (2023a) Overview of WHO- and UNEP-coordinated human milk studies and their link to the Stockholm Convention on persistent organic pollutants. In: Malisch R, Fürst P, Šebková K (eds) Persistent organic pollutants in human milk. Springer, Cham (in this volume, Part I)
Malisch R, Schächtele A, van Leeuwen FXR, Moy G, Tritscher A (2023b) WHO- and UNEP-coordinated exposure studies 2000-2019: Findings of polychlorinated biphenyls, polychlorinated dibenzo-p-dioxins and polychlorinated dibenzofurans. In: Malisch R, Fürst P, Šebková K (eds) Persistent organic pollutants in human milk. Springer, Cham (in this volume, Part III)
Malisch R, Schächtele A, van Leeuwen FXR, Moy G, Tritscher A, Šebková K, Klánová J, Kalina J (2023c) Time trends in human milk derived from WHO- and UNEP-coordinated exposure studies, Chapter 1: polychlorinated biphenyls, polychlorinated dibenzo-p-dioxins and polychlorinated dibenzofurans. In: Malisch R, Fürst P, Šebková K (eds) Persistent organic pollutants in human milk. Springer, Cham (in this volume, Part IV)
Petreas M, She J, Brown FR, Winkler J, Windham G, Rogers E, Zhao G, Bhatia R, Charles MJ (2003) High body burdens of 2,2′,4,4′-tetrabromodiphenyl Ether (BDE-47) in California women. Environ Health Perspect 111:1175–1179
Schächtele A, Hardebusch B, Krätschmer K, Tschiggfrei K, Zwickel T, Malisch R (2023) Analysis and quality control of WHO- and UNEP-coordinated human milk studies 2000-2019: polybrominated diphenyl ethers, hexabromocyclododecanes, chlorinated paraffins and polychlorinated naphthalenes. In: Malisch R, Fürst P, Šebková K (eds) Persistent organic pollutants in human milk. Springer, Cham (in this volume, Part III)
Schecter A, Pavuk M, Päpke O, Ryan JJ, Birnbaum L, Rosen R (2003) Polybrominated diphenylethers (PBDEs) in U.S. mother’s milk. Environ Health Perspect 111:1723–1729
Šebková K (2023) The Stockholm Convention and its implementation by regional and global monitoring reports. In: Malisch R, Fürst P, Šebková K (eds) Persistent organic pollutants in human milk. Springer, Cham (in this volume, Part I)
Sen PK (1968) Estimates of the regression coefficient based on Kendall’s Tau. J Am Stat Assoc 63:1379–1389. https://doi.org/10.1080/01621459.1968.10480934
Sharma BM, Kalina J, Whaley P, Scheringer M (2021) Towards guidelines for time-trend reviews examining temporal variability in human biomonitoring data of pollutants. Environ Int 151:106437. https://doi.org/10.1016/j.envint.2021.106437
She J, Petreas M, Winkler J, Visita P, McKinney M, Kopec D (2002) PBDEs in the San Francisco Bay Area: measurements in harbor seal blubber and human breast adipose tissue. Chemosphere 46:697–707
She J, Holden A, Sharp M, Tanner M, Williams-Derry C, Hooper K (2007) Polybrominated diphenyl ethers (PBDEs) and polychlorinated biphenyls (PCBs) in breast milk from the Pacific Northwest. Chemosphere 67:S307–S317
Simpson EH (1951) The interpretation of interaction in contingency tables. J R Stat Soc 13:238–241
Sudaryanto A, Kajiwara N, Tsydenova O, Isobe T, Yu H, Takahashi S, Tanabe S (2008) Levels and congener profiles of PBDEs in human breast milk from China: Implication on exposure sources and pathways. Chemosphere 73:1661–1668
Theil H (1992) A rank-invariant method of linear and polynomial regression analysis. In: Raj B, Koerts J (eds) Henri Theil’s contributions to economics and econometrics. Advanced studies in theoretical and applied econometrics, vol 23. Springer, Dordrecht, pp 345–381. https://doi.org/10.1007/978-94-011-2546-8_20
Thuresson K, Hoglund P, Hagmar L, Sjodin A, Bergman A, Jakobsson K (2006) Apparent half-lives of hepta- to decabrominated diphenyl ethers in human serum as determined in occupationally exposed workers. Environ Health Perspect 114:176–118
UNEP (2001) Stockholm Convention on Persistent Organic Pollutants (POPs), Text and Annexes. http://www.pops.int
UNEP (2009a) Factsheet “Tetrabromodiphenyl ether and pentabromodiphenyl ether”. http://www.pops.int/TheConvention/ThePOPs/TheNewPOPs/tabid/2511/Default.aspx
UNEP (2009b) Factsheet “Hexabromodiphenyl ether and heptabromodiphenyl ether”. http://www.pops.int/TheConvention/ThePOPs/TheNewPOPs/tabid/2511/Default.aspx
UNEP (2013) Conference of the Parties to the Stockholm Convention on Persistent Organic Pollutants, Sixth meeting, Geneva, 28 April–10 May 2013: Results of the global survey on concentrations in human milk of persistent organic pollutants by the United Nations Environment Programme and the World Health Organization. UNEP/POPS/COP.6/INF/33
UNEP (2015) Guidance on the global monitoring plan for persistent organic pollutants, January 2013. Conference of the parties to the Stockholm Convention on Persistent Organic Pollutants, Seventh meeting, Geneva, 4–15 May 2015. UNEP/POPS/COP.7/INF/39) (168 pages)
UNEP (2017) Second global monitoring report. UNEP/POPS/COP.8/INF/38
UNEP (2019) Guidance on the global monitoring plan for persistent organic pollutants. UNEP/POPS/COP.9/INF/36. http://www.pops.int/TheConvention/ConferenceoftheParties/Meetings/COP9/tabid/7521/Default.aspx
UNEP (2020) All POPs listed in the Stockholm Convention, http://www.pops.int/TheConvention/ThePOPs/AllPOPs/tabid/2509/Default.aspx
UNEP (2022) Monitoring reports. Link to first monitoring reports, second monitoring reports and third monitoring reports of the regional organization groups and the global coordinating group. http://www.pops.int/implementation/globalmonitoringplan/monitoringreports/tabid/525/default.aspx (Stockholm Convention > Implementation > Global Monitoring Plan > Monitoring Reports)
Van den Berg M, Birnbaum L, Denison M, De Vito M, Farland W, Feeley M, Fiedler H, Hakansson H, Hanberg A, Haws L, Rose M, Safe S, Schrenk D, Tohyama C, Tritscher A, Tuomisto J, Tysklind M, Walker N, Peterson E (2006) The 2005 World Health Organization re-evaluation of human and mammalian Toxic Equivalency Factors (TEFs) for dioxins and dioxin-like compounds. Toxicol Sci 93(2):223–241
van den Berg M, Denison MS, Birnbaum LS, DeVito MJ, Fiedler H, Falandysz J, Rose M, Schrenk D, Safe S, Tohyama C, Tritscher A, Tysklind M, Peterson RE (2013) Polybrominated dibenzo-p-dioxins, dibenzofurans, and biphenyls: Inclusion in the Toxicity Equivalency Factor Concept for dioxin-like compounds. Toxicol Sci 133(2):197–208. https://doi.org/10.1093/toxsci/kft070
van den Berg M, Duursen MBM, Tritscher A, Malisch R, Peterson RE (2023) Risk-benefit analysis for the breastfed infant based on the WHO- and UNEP human milk surveys for dioxin-like compounds. In: Malisch R, Fürst P, Šebková K (eds) Persistent organic pollutants in human milk. Springer, Cham (in this volume, Part IV)
Acknowledgments
This publication was developed in the framework of the projects titled “Implementation of the POPs Monitoring Plan in the Asian Region” and “Continuing regional Support for the POPs Global Monitoring Plan under the Stockholm Convention in the Africa, Pacific and Latin-American and Caribbean Region,” funded by the Global Environment Facility and in close collaboration with and support of CVUA Freiburg.
The worldwide implementation of the Global Monitoring Plan for POPs, including that of the UNEP/WHO global human milk studies, is made possible thanks to the generous contributions to the Stockholm Convention Voluntary Trust Fund by the Governments of Japan, Norway, and Sweden and through the European Union’s Global Public Goods and Challenges Programme (GPGC). Further, the substantial contributions made by the Global Environment Facility to support POPs monitoring activities in regions implemented by UNEP, in close collaboration with WHO, particularly for the global human milk surveys, are greatly appreciated.
Data analysis was supported by the RECETOX Research Infrastructure (No LM2018121) and the CETOCOEN EXCELLENCE Teaming Phase 2 project financed by the European Union’s Horizon 2020 (No 857560) and the European Structural and Investment Funds: No CZ.02.1.01/0.0/0.0/17_043/0009632).
The authors express their gratitude to the National Coordinators of the WHO- and UNEP-coordinated exposure studies for their excellent work to collect the human milk samples and to prepare and send the pooled samples to the WHO/UNEP Reference Laboratories, which included great efforts to plan and implement the national studies with the assistance of the health, environment, laboratory, and administrative staff. The continuous exchange of information between the National Coordinators and WHO, UNEP and the Reference Laboratories was an important aspect for the successful organization of these studies on a global level.
Hae Jung Yoon, Seongsoo Park, and Philippe Verger (WHO Department of Food Safety and Zoonoses) are acknowledged for their coordinating support during their time at WHO, and Lawrence Grant (WHO) for the statistical analysis of the sampling protocols.
We thank Katarina Magulova and Ana Witt (Secretariat of the Basel, Rotterdam and Stockholm Conventions) and Jacqueline Alvarez, Haosong Jiao, and Gamini Manuweera (United Nations Environment Programme, Economy Division, Chemicals and Health Branch) for their support and contributions to these surveys, furthermore Heidelore Fiedler for the conception and implementation of the GMP projects during her time at the UNEP Economy Division, Chemicals and Health Branch.
We also thank the team at CVUA Freiburg for the performance of the analyses of the POPs presented in this publication.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Ethics declarations
The authors alone are responsible for the views expressed in this publication, which do not necessarily represent the decisions, policy or views of the World Health Organization and the United Nations Environment Programme.
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2023 The Author(s)
About this chapter

Cite this chapter
Schächtele, A. et al. (2023). WHO- and UNEP-Coordinated Exposure Studies 2000–2019: Findings of Polybrominated Substances (PBDE, HBCDD, PBB 153, PBDD/PBDF). In: Malisch, R., Fürst, P., Šebková, K. (eds) Persistent Organic Pollutants in Human Milk. Springer, Cham. https://doi.org/10.1007/978-3-031-34087-1_9
Download citation
DOI: https://doi.org/10.1007/978-3-031-34087-1_9
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-34085-7
Online ISBN: 978-3-031-34087-1
eBook Packages: Chemistry and Materials ScienceChemistry and Material Science (R0)