
Abstract
The estimation of the absorbed dose is an essential factor for the determination of risks and therapeutic benefit of internal radiation therapies. Optimal dose estimations require time-consuming and sophisticated methods, which are difficult owing to practical purposes mainly related to the patients’ status and physical reasons. Nevertheless, to make patient-specific dosimetry available, we use a special developed dosimetry procedure, which can be used in daily clinical routine.
The so-called Bad Berka Dose Protocol (BBDP) is a hybrid method based on serial planar whole body scans and SPECT/CT acquisitions and represents a compromise between the calculation model and practical conditions. It has ensured dose estimation in daily clinical routine with a reasonable effort and within acceptable time. Our protocol allows each of our patients to undergo dosimetry after therapy using Lu-177-labeled radiopharmaceuticals, especially PRRT or PSMA RLT.
In consequence, dosimetry based on our protocol helps to identify optimal ligands, for PRRT as well as for PSMA RLT. It helps to plan the individual treatment. Additionally, dosimetry is important for the evaluation of the therapy: concerning response, benefit and toxicity. Besides PRRT and PRLT, the BBDP can be used to make dose estimations for all kinds of different tracers. Dosimetry adds a lot of important information to clinical and medical facts in order to find the optimal therapeutic path for each individual patient.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
27.1 Introduction
The story of dosimetry for molecular radiotherapy at the Zentralklinik Bad Berka starts in 2004. At the department of nuclear medicine, Professor Dr. R. P. Baum already performed peptide receptor radionuclide therapy (PRRT) using Y-90 labeled DOTATATE since 1999. In August 2004, the first PRRT using Lu-177 DOTATATE was performed. It was the very first Lu-177 therapy and also the very first dosimetric study.
This first patient was a 41-year old woman, which presented with a sphenoidal meningioma that affected the right optical nerve. The initial diagnosis was in December 2003; after surgery, the MRI still detected residual tumor and she had increasing right-sided defect of field of view. Due to the progressive visual field defect on the right side, the ophthalmologist gave a prognosis of rapidly progressive blindness of the right eye within the next few months. The patient reported increasing visual disturbances and feeling of pressure behind the right eye as well as intermittent headaches.
Before therapy, in order to confirm the SSTR expression of the meningioma, at this time a Tc-99 m EDDA Hynic Toc scintigraphy as well as SPECT was performed. In addition, Ga-68 DOTA-NOC PET/CT was acquired. All imaging studies proved the high SSTR expression of the meningioma (Fig. 27.1).

First Lu-177 PRRT patient in Bad Berka before therapy: (a) Tc-99 m EDDA Hynic Toc scintigraphy; (b) SPECT; (c) Ga-68 DOTANOC MIP
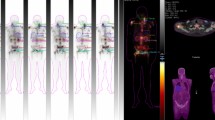
Because of the high SSTR expression, the patient received 5300 MBq of Lu-177 DOTATATE. After the administration, serial planar whole body scans were performed to measure the time-dependent biodistribution of the radiopharmaceutical (Fig. 27.2).

First Lu-177 PRRT patient in Bad Berka: (a) first PRRT anterior whole-body scintigraphy; (b) corresponding time-activity curves
Based on these uptakes, mean absorbed organ and tumor doses were estimated for the first time. The whole body dose was 0.05Gy/GBq, the renal mean absorbed dose was about 1 Gy/GBq, and the dose to the meningioma was approximately 7Gy/GBq or 35Gy. In addition, the effective half-life of the compound in organs and tumor was also calculated, the longest half-life of 78 h was found in the kidneys and a shorter half-life of 38 h for the tumor.
Three months after this first cycle, the patient was treated again. Since then, just restaging was done and until now the patient is doing fine, she is free of any complaints and her visual field has improved over time.
This success story was the starting shot for dosimetry in molecular radiotherapy in Bad Berka.
27.2 Bad Berka Dose Protocol
Dosimetry in Bad Berka was always carried out using an in-house developed dose protocol, the so-called Bad Berka dose protocol (BBDP), which is constantly being further improved.
The BBDP is a so-called hybrid method combining planar and SPECT imaging for dose estimation. The dose estimation requires an accurate determination of the time-dependent activity curve of the organs and tumors to be analyzed. Thus, most important is the correct evaluation of the distribution and the kinetics of the administered radiopharmaceutical [1, 2]. We developed a practically convenient procedure by adapting the calculation model to our particular conditions. The main objective was to create a method which is practicable in daily clinical routine and to make dosimetry available for all patients. The dosimetric approach is based on the MIRD scheme, and mean absorbed doses are estimated using the OLINDA 2.0 software [3,4,5,6]. The workflow of the BBDP is shown in Fig. 27.3.

Workflow Bad Berka Dose Protocol
At least five serial planar whole-body scintigraphies and one regional SPECT/CT were acquired per patient. For planar whole-body (WB) imaging, the following gamma camera settings were implemented: MEDISO spirit DH-V dual-headed gamma camera (Medical Imaging Systems, Budapest, Hungary), MEGP collimator, 15% energy window, peak at 208 keV, scan speed 15 cm/min. WB scintigraphies were acquired at following time points post injection (p.i.): from 0.5 h p.i. (immediately after administration of therapeutic activity and before bladder voiding) up to 68 h p.i.. Additionally, post-therapy imaging using SPECT/CT of kidneys and/or tumor-involving regions of the body was performed at 24, 48, or 72 h p.i. using a Siemens Symbia T camera system (Siemens Healthcare GmbH, Erlangen, Germany) and the following settings: MELP collimator, peak at 113 keV and 208 keV (15% energy windows and 20% upper and lower scatter window), 128×128 matrix, 32 projections with 30 s per step, body contour.
Since the patients were not allowed to empty the bladder before the first scan, the total body counts acquired immediately after the injection were defined to be 100% of the administered activity. Total body counts on the subsequent scans were expressed as fractions of injected activity (%IA). Regions of interest (ROI) were drawn manually over the source regions over the acquired scintigraphy images, which were then analyzed using the software of the HERMES system (Hermes Medical Solutions, Stockholm, Sweden). Source regions were defined as organs and metastases showing significant specific uptake, which could be clearly delineated on each post-therapy scan. ROIs were always drawn by a physicist in collaboration with a nuclear medicine physician, who selected the suitable lesions for dosimetry (i.e., lesions with the highest uptake in the respective organ). The biodistribution and kinetics of whole body and source organs were determined based on this ROI analysis. The SPECT/CT scans were reconstructed and quantified using the HERMES SUV SPECT software (HERMES Medical Solutions, Stockholm, Sweden). After segmentation, the SPECT activity of source regions was used to scale the time-activity curves obtained from planar imaging. In the next step, these time-activity curves were fitted to mono- or bi-exponential functions in order to calculate effective half-lives and the time-integrated activity coefficient. Mean absorbed organ and tumor doses were finally estimated using OLINDA 2.0. The ICRP 89 adult model and the spheres model were used for normal organs and tumor lesions, respectively (both included in OLINDA 2.0). Volumes of normal organs and tumor lesions were obtained by the latest CT of the patient in order to adopt the model to individual organ and tumor volumes. Organs showing tumor involvement were excluded from dosimetric evaluation.
27.3 Dosimetry in Daily Clinical Routine
The BBDP is a hybrid method which is used in daily clinical routine, with some advantages but also disadvantages. Planar dosimetry represents whole body dosimetry including all organs and metastases, but it is limited by organ superimposition and inaccurate attenuation and scatter correction. Hybrid dosimetry on the other side is using 3D imaging with improved accuracy, but the segmentation is challenging and depending on the number of SPECT/CTs or the field of view, hybrid dosimetry cannot characterize whole body biodistribution. Thus, there are some limitations of the dose estimation:
-
Physical/technical:
-
Number of time points.
-
Availability of late scan.
-
Quantification and volumetric analysis.
-
Dose estimation based on models (OLINDA).
-
-
Medical:
-
Patient’s condition.
-
-
Time effort for:
-
Patient.
-
Technologist.
-
Physician.
-
Physicist.
-
Consequently, dosimetry is still a dose estimation, an approximation of the mean absorbed dose. The challenge for the clinical use is to find an optimal practical method to enable individual dosimetry for each patient and each therapy cycle (e.g., in comparison to external radiation therapy). The solution is a compromise between the theoretical model and daily circumstances by adapting the MIRD scheme to the special conditions at the department. The BBDP represents the optimal dosimetry procedure for the clinical routine at the nuclear medicine ward of the Zentralklinik Bad Berka.
Until December 2019, dosimetry was performed using the BBDP for 1180 Lu-177 PRRT cycles, and another 289 for Lu-177 PRLT; in total, dosimetry was analyzed for more than 1500 therapy cycles. Figure 27.4 shows the number of dosimetry studies over time as well as the number of studies using different (commonly used) tracers. In the following, some particular examples for the use of dosimetry and the role of dosimetry results will be given.

Number of dosimetry cycles performed in Bad Berka for PRRT and PRLT
27.4 Dosimetry for PRRT
Already in 2007 we published first results of dosimetry in PRRT. The comparison of Lu-177 DOTATATE and Lu-177 DOTANOC revealed a higher uptake of DOTANOC for whole body and normal tissue as well as a higher tumor uptake for DOTATATE. The resulting mean absorbed kidney and spleen doses were comparable for both ligands, and the mean absorbed tumor doses tended to be higher for DOTATATE. Based on these dosimetry results, we showed that DOTATATE has characteristics which are more favorable for PRRT of patients with neuroendocrine tumors [7].
In another large patient cohort, we compared DOTATATE, HA-DOTATATE and DOTATOC. We found the lowest renal uptake as well as the lowest renal absorbed dose for DOTATOC. These examples emphasize how dosimetry can help to evaluate the therapy and to find the optimal peptide for PRRT (Fig. 27.5).

Comparison of renal dosimetry in PRRT using different peptides: (a) renal uptake; (b) renal mean absorbed dose
A high interpatient variability was found for all dosimetry results. This is not unexpected since heterogeneous groups of patients, having varying receptor densities and tumor burden, were analyzed. In addition, the results showed a high intra-patient variability in the undergoing several cycles of therapy with different peptides. The dosimetry results stored in the database also give the possibility to analyze several therapy cycles of a single patient.
Figure 27.6 shows serial whole body scintigraphies of a patient which presented with a NEN of the pancreas and hepatic, lymph node as well as bone metastases. He received multiple cycles of PRRT over time; the first three cycles were done using DOTATATE followed by four cycles of DOTATOC. Dosimetry results are shown in Fig. 27.7.

Anterior whole body scintigraphy of serial PRRT cycles over a long period of time in the same patient

Intra-patient variability of multiple PRRT cycles in the same patient: (a) whole body and renal uptake; (b) whole body mean absorbed dose; (c) renal mean absorbed dose
The whole body uptake as well as the renal uptake shows some differences between the dosimetry cycles. Also the resulting mean absorbed doses show some variation over time. If the first whole body dose is considered to be 100%, the whole body dose of consecutive therapies varies from −3 to 60%. The same is true for the renal absorbed dose. Interestingly, the renal doses were less from the fourth therapy on. This could be due to the changing tumor burden, or other therapies in between. The patient received DOTATOC in these cases, so these results could also indicate a lower renal dose when DOTATOC is used.
27.5 PRRT Antagonists
Since over two decades, somatostatin receptor (SSTR) agonists are being used for molecular imaging of SSTR-expressing tumors. Clinical studies with SSTR antagonist-based PET/CT have shown a higher tumor detection rate in SSTR expressing tumors than PET/CT applying the SSTR agonist [8,9,10]. Consequently, we used dosimetry in order to compare the kinetics and absorbed doses in patients undergoing peptide receptor radionuclide therapy (PRRT) using the Lu-177 labeled antagonist DOTA-LM3.
Analyzed were biodistribution, effective half-life and mean absorbed organ and tumor doses. Very intense uptake in the tumor lesions as well as significant uptake in the kidneys, spleen and liver was observed in all patients. A rapid clearance of tracer from whole body was also found, whereas the longest effective half-life was obtained for metastases. The dosimetry of Lu-177 antagonists revealed relatively high absorbed tumor and organ doses, where the spleen had the highest absorbed dose of the analyzed normal organs. Additionally, tumor lesions were grouped in bone and liver metastases. A higher uptake, longer effective half-life and higher mean absorbed doses were found for liver metastases compared to bone metastases.
In accordance with imaging studies, we found higher tumor uptake, longer effective half-life and higher mean absorbed organ and tumor doses for the antagonist compared to the agonist DOTATOC (Fig. 27.8).

PRRT dosimetry comparison using DOTATOC versus DOTA-LM3: (a) biodistribution; (b) effective half-life; (c) mean absorbed dose
These first results showed a high accumulation of the antagonist DOTA-LM3 in metastases. Despite the also high mean absorbed organ doses, we concluded that PRRT using DOTA-LM3 appears to be promising, as significantly high tumor doses are achieved.
27.6 Dosimetry for PSMA Radioligand Therapy
Besides dosimetry for PRRT, dosimetry for PSMA radioligand therapy (PRLT) is very valuable. The most frequently applied ligands at our center are PSMA I&T (since April 2013) and PSMA-617 [11, 12].
Of particular interest is the variation of dosimetry parameters in correlation with the serum PSA level, as shown by Fig. 27.9. In this study, 19 patients were included. The percentage differences of the tumor and renal absorbed dose during the second PRLT cycle compared to the first one were analyzed. 63% of the patients showed a decrease of absorbed tumor dose and increased renal dose at the second therapy cycle. Additionally these patients also had a lower PSA level after two PRLT cycles. These results indicate a correlation of tumor response and change in PSA level.

Correlation of dosimetry results and change in PSA
An inter-cycle variation in the absorbed tumor and kidney doses was found, which correlates with the change in PSA after PRLT. A decrease in serum PSA, indicative of therapy response in tumors, is therefore associated with a decrease in the absorbed tumor dose during subsequent PRLT cycle and vice versa. A decrease in tumor burden results in an increase in the absorbed renal dose in the next therapy cycle. We concluded finally that the administration of a higher amount of radioactivity in the first cycle seems to be reasonable, since the tumor doses tend to decrease in the subsequent cycles due to therapy response. The results of this study show the direct influence of dosimetry on clinical decision-making and prove the importance of dosimetry in radionuclide therapy.
27.7 Conclusions
What is the “best dosimetry?” Historically, in radionuclide therapy, a standardized amount of a radionuclide is administered, neglecting patient size, tumor burden, disease progression and intralesional heterogeneity. External beam radiotherapy on the other hand is highly individualized to maximize the dose to target whilst minimizing radiation dose delivered to normal tissues.
Treatment planning is to deliver what is believed to be the dose of radiation to target to attempt to effect local control and to limit the radiation exposure of dose-limiting organs. There might be some limits, for example, imaging modalities, patient conditions, time effort. However, the following compromise situation may succeed: Start a course with a dose based on the experience of physicians and physicists and acquire necessary data to individualize subsequent treatments – even though intraindividual differences between consecutive therapy cycles are well known.
In summary, we hope that the importance of dosimetry could be pointed out. Using protocols like the BBDP makes it practicable in daily clinical routine within acceptable time and affordable effort. Dosimetry helps to identify optimal ligands, for PRRT as well as for PSMA RLT. It helps to plan the individual treatment. Additionally, dosimetry is important for the evaluation of the therapy: concerning response, benefit and toxicity. Beside PRRT and PRLT, the BBDP can be used to do dose estimations for all kinds of different tracer, labelled with Lu-177 or even labelled with other nuclides [13,14,15].
The title of this article is: “Sola Dosis Facit Venenum,” which means that the dose makes the poison. Consequently, if one wants to do therapy in nuclear medicine, dosimetry is mandatory. Dosimetry adds a lot of important information to clinical and medical facts in order to find the optimal therapeutic path for each individual patient. But a nuclear medicine department also needs one important prerequisite: the physician who believes in dosimetry. This cannot be taken for granted; sometimes, it is a challenge to make the physician believe in physics, even in nuclear medicine where physics is the base of “practically everything.”
Professor Dr. R. P. Baum is such a physician, he always believed in dosimetry results and supported the team all the time. He always encouraged to stay tuned, to use the latest methods to provide the important dosimetry results – always with the aim of finding the best possible therapy for the individual patient.
The author wants to thank Prof Baum for this encouragement and steady support during all the years in Bad Berka. It was an eventful time and a great collaboration between medicine and physics.
References
Stabin MG, Siegel JA. Physical models and dose factors for use in internal dose assessment. Health Phys. 2003;85(3):294–310.
Sgouros G. Dosimetry of internal emitters. J Nucl Med. 2005;46(1):18S–27S.
Siegel JA, Thomas SR, Stubbs JB, Stabin MG, Hays MT, Koral KF, et al. MIRD pamphlet no. 16: Techniques for quantitative radiopharmaceutical biodistribution data acquisition and analysis for use in human radiation dose estimates. J Nucl Med. 1999;40(2):37S–61S.
Bolch WE, Eckerman KF, Sgouros G, Thomas SR. MIRD pamphlet No. 21: a generalized schema for radiopharmaceutical dosimetry—standardization of nomenclature. J Nucl Med. 2009;50(3):477–84.
Stabin MG, Sparks RB, Crowe E. OLINDA/EXM: the second-generation personal computer software for internal dose assessment in nuclear medicine. J Nucl Med. 2005;46(6):1023–7.
Stabin MG, Siegel JA. RADAR dose estimate report: a compendium of radiopharmaceutical dose estimates based on OLINDA/EXM version 2.0. J Nucl Med. 2018;59(1):154–60.
Wehrmann C, Senftleben S, Zachert C, Muller D, Baum RP. Results of individual patient dosimetry in peptide receptor radionuclide therapy with 177Lu DOTA-TATE and 177Lu DOTA-NOC. Cancer Biother Radiopharm. 2007;22(3):406–16.
Fani M, Nicolas GP, Wild D. Somatostatin receptor antagonists for imaging and therapy. J Nucl Med. 2017;58(Suppl 2):186783.
Wild D, Fani M, Fischer R, Del Pozzo L, Kaul F, Krebs S, et al. Comparison of somatostatin receptor agonist and antagonist for peptide receptor radionuclide therapy: a pilot study. J Nucl Med. 2014;55(8):1248–52.
Bodei L, Weber WA. Somatostatin receptor imaging of neuroendocrine tumors: from agonists to antagonists. J Nucl Med. 2018;59(6):907–8.
Kulkarni HR, Singh A, Schuchardt C, Niepsch K, Sayeg M, Leshch Y, et al. PSMA-based Radioligand therapy for metastatic castration-resistant prostate cancer: the Bad Berka experience since 2013. J Nucl Med. 2016;57(Suppl 3):170167.
Baum RP, Kulkarni HR, Schuchardt C, Singh A, Wirtz M, Wiessalla S, et al. Lutetium-177 PSMA Radioligand therapy of metastatic castration-resistant prostate cancer: safety and efficacy. J Nucl Med. 2016;21(115):168443.
Baum RP, Prasad V, Muller D, Schuchardt C, Orlova A, Wennborg A, et al. Molecular imaging of HER2-expressing malignant tumors in breast cancer patients using synthetic 111In- or 68Ga-labeled affibody molecules. J Nucl Med. 2010;51(6):892–7.
Baum RP, Kluge A, Gildehaus FJ, Bronzel M, Schmidt K, Schuchardt C, et al. Systemic Endoradiotherapy with carrier-added 4-[(131)I]Iodo-L-phenylalanine: clinical proof-of-principle in refractory glioma. Nucl Med Mol Imaging. 2011;45(4):299–307.
Baum RP, Singh A, Schuchardt C, Kulkarni HR, Klette I, Wiessalla S, et al. (177)Lu-3BP-227 for neurotensin receptor 1-targeted therapy of metastatic pancreatic adenocarcinoma—first clinical results. J Nucl Med. 2017;12(117):193847.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2024 The Author(s)
About this chapter

Cite this chapter
Schuchardt, C. (2024). Sola Dosis Facit Venenum: Dosimetry for Molecular Radiotherapy in Bad Berka. In: Prasad, V. (eds) Beyond Becquerel and Biology to Precision Radiomolecular Oncology: Festschrift in Honor of Richard P. Baum. Springer, Cham. https://doi.org/10.1007/978-3-031-33533-4_27
Download citation
DOI: https://doi.org/10.1007/978-3-031-33533-4_27
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-33532-7
Online ISBN: 978-3-031-33533-4
eBook Packages: MedicineMedicine (R0)