
Abstract
This chapter is primarily about the rationale and decision-making process of including advanced treatments (immuno-oncology therapy, hepatitis B and C medications), tests (next-generation sequencing, NGS) and medical devices in the benefits package of the National Health Insurance.
Because of the high prevalence of hepatic cirrhosis and advancement in treatment, Taiwan aims to expand the coverage of hepatitis B treatment and eradicate hepatitis C by 2025. This chapter documents the history and achievements in the expansion of reimbursed indications. As for NGS, although it is recognized as essential for personalized oncology treatment, it requires regulation support to expand its coverage.
The chapter ends with discussion in detail regarding why and how National Health Insurance Administration (NHIA) expanded its coverage for medical devices as well as strategies used to improve price transparency for out-of-pocket medical devices.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others

Keywords
- Precision medicine
- Immuno-oncology therapy
- Next-generation sequencing
- Real-world data
- Health Technology Assessment
- Balance-billing medical device/material
Introduction
With the development of the medical industry, immunotherapy brings a new dawn for cancer treatment, and personalized precision medicine has been applied in the development of cancer treatment with the advancement of molecular medicine (Fig. 9.1).

National Health Insurance’s policies of precision medicine
Owing to advancements in treatment, Taiwan, with a high prevalence of hepatic cirrhosis, aims to expand the reimbursement indications in hepatitis B and strives to eradicate hepatitis C by 2025.
In addition, as the treatment pattern has changed from traditional surgeries in the past to interventional treatment, endoscopic surgery, and robotic arms, plus the increasing life expectancy of the national people, the clinical and public demand for new medical devices has been growing.
In this chapter, we will discuss the rationale and the decision-making process of combining reimbursement of advanced treatments (immuno-oncology therapy, hepatitis B and C medications), tests (next-generation sequencing, NGS), and medical devices in the benefits package of the National Health Insurance (NHI).
Including Immuno-oncology Therapy in National Health Insurance Benefits
To enable cancer patients to be treated with new drugs as soon as possible, cancer immunotherapy for eight cancer types and 11 indications have been covered by the NHI since 2019, such as the first-line treatments for nonsmall-cell lung cancer and urothelial carcinoma, earlier than other Asian countries. Then, the reimbursed indications were reviewed according to the scientific evidence of the patients’ real-world treatment outcome. Based on the evaluation results, since 2020, the reimbursed course of treatment was determined to extend up to 2 years for patients responsive to the medication. As for the gastric and liver cancer indications, as it shows no significant benefits compared with the existing treatments, for the first time the National Health Insurance Administration (NHIA) decided to suspend applications from new patients because the drug supplier didn’t agree on the risk-sharing scheme, but patients who are already under the treatment can continue until disease progression.
Immunotherapy is a trend in cancer treatment. Since April 2019, the NHI has covered cancer immunotherapy, including pembrolizumab, nivolumab, atezolizumab, and avelumab for the treatment of melanoma, nonsmall-cell lung cancer, classic Hodgkin’s lymphoma, urothelial carcinoma, head and neck squamous cell carcinoma, gastric adenocarcinoma, renal cell carcinoma, hepatocellular carcinoma, Merkel Cell Carcinoma, and other indications. Patients who meet the criteria of PD-L1 expression are fully covered by the NHI.
Because some indications of the cancer immunotherapy have not yet completed phase III clinical trials, the clinical benefits are uncertain. To let the patients who can really benefit use the drug, the registry system for “Pre-Review of Cancer Immunotherapy Case Applications” has been established since the cancer immunotherapy was first listed. This system collects real-world data (RWD) such as the treatment outcomes and significant adverse effects of patients under the treatment, so that the benefits and rationality of the payment for such drugs could be evaluated.
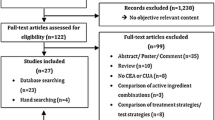
According to the results of real-world evidence (RWE) analysis, the response rate to cancer immunotherapy, including complete/partial response (CR/PR), is only about 20% on average (Fig. 9.2). Although the relative benefits are limited, to let patients responsive to the treatment benefit from the value of the new drugs, the NHIA decided that since April 2020, patients who have been evaluated as having stable disease after treatment can continue the treatment for another 12 weeks, the same as those with CR/PR. In the mean time, the reimbursed course of treatment is extended up to 2 years for patients responsive to the treatment; as for patients with urothelial carcinoma with a relatively good response rate, the reimbursement criteria are also loosened.

Analysis of the outcomes of the latest treatment in patients using cancer immunotherapy. Note: (1) Cases for analysis: 2012 cases that have been approved for renewal. (2) As of 30 September 2020
On the other hand, more than 90% of gastric cancer patients and about 80% of liver cancer patients did not respond to cancer immunotherapy drugs (Fig. 9.3). Although the treatment outcomes differ between patients treated by different physicians, most patients experienced disease progression or expired within about 2 months after the treatment. The treatment outcomes are similar to those of patients treated with chemotherapy or target therapy, but the NHI has to pay several times more. Therefore, after referring to domestic data, international cancer treatment guidelines, and other reimbursement recommendations from the United Kingdom, Australia, and Canada, the National Health Insurance Pharmaceutical Benefit and Reimbursement Scheme Joint Committee, which is composed of professionals, representatives of medical associations, employers, and patient groups, decided to suspend applications from new patients with these two cancers, but patients who are already under treatment can continue the treatment until disease progression.

The latest evaluation of disease status in each indication. Note: (1) Cases for analysis: 2012 cases that have been approved for renewal. (2) As of 30 September 2020
To provide patients with gastric cancer and liver cancer with new treatment options, the NHIA continues to communicate with pharmaceutical firms on diversified reimbursement mechanisms, hoping that pharmaceutical firms can share the drug costs for patients not responsive to the treatment, and ask pharmaceutical firms to develop precise pretreatment testing methods to find out patients suitable for treatments and ensure the safe use of medications. At the same time, the NHIA also speeds up the relaxation of the reimbursement regulations for other treatments used for gastric and liver cancer, such as expanded coverage of Herceptin and Lonsurf for gastric cancer treatment and the listing of the targeted therapy for liver cancer, Lenvima, hoping to provide patients with more beneficial treatment options.
Since the listing of cancer immunotherapy in 2019, more than 3200 patients have applied to use the medication, reflecting the medical needs of patients. The NHIA also continues to collect patients’ responses to the medication as suggested by cancer patient groups, hoping to use RWD to evaluate and review the reimbursement regulations of cancer immunotherapy. To ensure cancer immunotherapy use in patients who can benefit from the medication, the NHI has also covered four types of PD-L1 kits for pretreatment testing since April 2020. This helps to identify patients who are likely responsive to cancer immunotherapy and enhances reimbursement efficiency.
Owing to the accelerated market approval process of new cancer drugs in many countries, the clinical benefits of cancer immunotherapy become highly uncertain, resulting in most public insurance schemes facing the risk of financial impact. Despite limited resources, Taiwan’s NHI covers cancer immunotherapy by adopting risk-sharing mechanisms and uses the RWE collected from the registry for evaluation, which can serve as references for decision-making and revising reimbursement regulations. This helps to enhance the efficiency of reimbursement. This reimbursement model can be applied to the listing of more new cancer drugs in the future. It enhances patient access to new drugs and allows pharmaceutical firms to share the risk of financial impact, which helps to ensure the sustainability of the NHI.
Inclusion of Next-Generation Sequencing in National Health Insurance Benefits
In the past, cancer drug treatment followed empirical therapy based on the accumulated clinical data from patients. Patients with the same type of cancer and cancer staging were given the same treatment, and doctors tried to control tumors with various drugs. They first gave drug A for treatment and then changed to drug B if the efficacy of drug A was low. With the advancement of molecular medicine, personalized precision medicine has been applied in the development of cancer treatment, enabling each patient’s specific biomarkers to be considered when determining the corresponding treatment. For example, only lung adenocarcinoma patients with epidermal growth factor receptor (EGFR) mutations would be given EGFR-targeted drugs to provide patients with a more effective and personalized treatment. Besides relieving the patients from suffering illness caused by traditional trial treatments, personalized medicine would reduce unnecessary examinations, tests, and consultation for the NHI.
Individual Genetic Testing
Currently, the genetic testing items covered by the NHI are single-gene tests carried out one after another according to the incidence of genetic mutations. Taking lung cancer as an example, EGFR and anaplastic lymphoma kinase (ALK) mutations, two common mutations in lung cancer patients, which account for 50% of the mutations, are tested first, and then the remaining specimen will be tested for other possible genes. However, the sequential test method may cause the risk of an unsatisfactory specimen, resulting in repeated specimen collection and delays in the timing of treatment.
According to statistics of the nine genetic testing items covered by the NHI (Table 9.1), leukemia, breast cancer, and lung cancer testing contribute to the majority of the testing costs, reaching 1.48 billion to 1.69 billion relative value units (RVUs) from 2019 to 2020 (excluding out-of-pocket costs and manufacturer’s repayments). The ALK in vitro diagnostics testing, an immunohistochemistry method for lung cancer, and All-RAS (rat sarcoma) mutation testing for colorectal cancer have been approved by the “National Health Insurance Fee Schedule and Reference List for Medical Services Joint Committee” in 2020. After agreements with pharmaceutical companies are signed, revising the fee schedule for these genetic tests and corresponding targeted therapy will be concurrently effective.
Future Direction: Next-Generation Sequencing
Next-generation sequencing, also known as second-generation sequencing, refers to methods different from the low throughput, high-cost, and time-consuming Sanger sequencing. Because NGS could process a larger number of nucleic acids simultaneously, its advantages, such as low cost of single-base sequencing, high throughput, and high speed, break the limitation of gene size or number for gene sequencing.
In response to the trend toward personalized precision medicine, the NHIA has begun to compile the list of targeted therapies that have been reimbursed by NHI or that will become covered shortly and their corresponding genetic testing. Questions and challenges regarding covering NGS as a treatment item are under discussion as well. For example, what is included in the list of genes that need to be sequenced for clinical practice? The cost calculation and test report format for NGS are also waiting to be determined.
Biotechnology industry laboratories are currently performing most NGS. However, according to Article 27, Paragraph 1 of the “Regulations Governing Contracting and Management of National Health Insurance Medical Care Institutions” and Note 33 of the “Report Format and Filling Instructions of Outpatient Medical Expenses of Contracted Medical Service Institutions,” hospitals can only entrust NHI-contracted medical institutions with performing medical examinations. Therefore, the NHI must review the feasibility of contracted hospitals entrusting external laboratories with the Laboratory Developed Test without violating current medical regulations and start drafting the expansion of the coverage and revising the fee schedule for the Laboratory Developed Test.
Expansion of the Coverage of Medications to Eradicate Hepatitis B and C
The World Health Organization (WHO) has proposed the goal of eliminating viral hepatitis by 2030, including a 90% reduction of new cases of chronic viral hepatitis B and C infections, 65% reduction of viral hepatitis B and C deaths, and treating 80% of eligible patients with chronic hepatitis B and C virus infection, aiming to stop the transmission of viral hepatitis. Therefore, the NHI plays an important role in providing patients with affordable and effective treatment.
Why Is the Treatment of Viral Hepatitis So Important?
Hepatitis B and C are important factors leading to liver cirrhosis and liver cancer. 15–20% of hepatitis B carriers with chronic hepatitis will develop liver cirrhosis, and cirrhosis will increase the incidence of liver cancer. More than half of hepatitis C infected patients will develop chronic hepatitis, and about 20% of them will develop liver cirrhosis, and every year about 3–5% of patients with liver cirrhosis will get liver cancer.
According to the analysis of the top 10 causes of death in Taiwan in 2019, chronic liver disease and liver cirrhosis are the tenth cause of death, and liver cancer is the second cause of cancer death. According to the claims data of the NHI, the number of hepatitis B patients has increased from nearly 168,000 in 2003 to 549,000 in 2019, and the RVUs of hepatitis B have also increased from 1.72 billion to 19.98 billion, which is an increase of nearly 12-fold in 17 years (Fig. 9.4). The expenditure on hepatitis B oral antiviral agents was 3.18 billion RVUs, which accounts for only 16%, and the remaining direct or indirect medical expenses account for 84%. As for hepatitis C , the number of patients has increased from nearly 74,000 in 2003 to 205,000 in 2019, and the RVUs of hepatitis C have also increased from 1.38 billion to 17.39 billion, which is an increase of nearly 13-fold in 17 years (Fig. 9.5). In the year before the new direct-acting antiviral agents for hepatitis C were covered, expenditure on antiviral medications used for the treatment of hepatitis C only accounted for 8.4%, and expenditure on other direct or indirect treatment accounted for 91.6%.

Statistics on hepatitis B patients over the years. Note: The data include outpatient and inpatient cases with hepatitis B-related diagnoses in the claimed primary and secondary diagnosis codes

Statistics on hepatitis C patients over the years. Note: The data include outpatient and inpatient cases with hepatitis C-related diagnoses in the claimed primary and secondary diagnosis codes
From the above data, we can understand that if hepatitis is not well controlled, liver cirrhosis and liver cancer will increase. If hepatitis patients can receive antiviral medication and be controlled properly, the NHI resources used to treat liver cirrhosis and liver cancer can also be saved for the treatment of other diseases. Based on this principle, the reimbursement indications for hepatitis B and hepatitis C medications in the NHI have also been gradually expanding along with the latest clinical developments.
Treatment of Hepatitis B Medication Under National Health Insurance
Taiwan began to promote the viral hepatitis treatment plan in 2003, and about 3000 people were treated with hepatitis B medication in the same year. Along with the progress in research, the NHI has gradually expanded the coverage according to the treatment guidelines for hepatitis B. From 2003 to 2019, the number of patients who have received hepatitis B medication was approximately 211,000 (Fig. 9.6). If 545,000 hepatitis B patients require treatment, the coverage rate of hepatitis B patients receiving treatment is 38.7% (211,000 ÷ 545,000).

The number of patients treated with National Health Insurance-covered hepatitis B antiviral medications
As for the reimbursed medications for hepatitis B medication, it has been gradually expanding over the years. The key points are summarized below.
-
1.
November 2009: the treatment course covered by the NHI was extended from at most 18 months to 36 months (for those with hepatitis B e-antigen (HBeAg) test turning negative during the treatment course, they can be paid for another 12 months).
-
2.
July 2010:
-
(a)
Long-term coverage of liver cirrhosis.
-
(b)
The reimbursed treatment course extends from 2 years to 3 years for those who develop resistance to the first-line treatment. If they relapse after medication withdrawal, patients can be treated with the combination therapy once, and the course of treatment is 3 years.
-
(a)
-
3.
January 2017
-
(a)
HBeAg positive before treatment: treatment until HBeAg turns negative and then another 12 months of coverage.
-
(b)
HBeAg negative before treatment: at least 2 years of the treatment course, and HBV DNA is tested every 6 months during the treatment for a total of three times. Withdraw the medication if the HBeAg tests are all negative, and the maximum reimbursement period is 36 months each time.
-
(c)
To cancel the limit (used to be twice per patient) on the number of treatments.
-
(a)
-
4.
February 2018: highly infectious pregnant women with hepatitis B are covered from the 28th week of pregnancy to 4 weeks after delivery, further reducing the risk of vertical infection.
-
5.
March 2021: the NHIA invited gastroenterologists to discuss the revision of the reimbursement regulations for hepatitis B medication, and there are five major points as follows:
-
(a)
Revise the reimbursement criteria for initiating therapy in patients with the signs of virus replication and active hepatitis.
-
(b)
Revise the reimbursement criteria for long-term treatment of liver cirrhosis.
-
(c)
Revise the reimbursement criteria for pre-exposure prophylaxis in nonliver transplant recipients.
-
(d)
Revise the reimbursement criteria for initiating therapy in patients of liver cancer who can receive eradicative treatment.
-
(e)
Newly added reimbursement criteria for treatment and prevention of hepatitis B in patients receiving immunosuppressant treatment.
-
(a)
Treatment of Hepatitis C Under the National Health Insurance
In the past, treatment for hepatitis C involved using pegylated interferon once a week combined with daily oral ribavirin, and the treatment took 6 months to 1 year. However, because interferon has to be injected frequently and the side effects are obvious, patients are discouraged from receiving the treatment, which results in a low treatment rate for hepatitis C. By the end of 2017, there were about 95,000 hepatitis C patients receiving interferon treatment, which is still lower than the number of people infected in Taiwan. Since 2014, direct-acting antiviral agents with a high cure rate have been successively launched around the world. The new direct-acting antiviral agents only need to be taken for 2–4 months, reducing side effects, and the cure rate is more than 90%.
In response to the trend toward hepatitis C patients receiving new drug treatments, the budget allocation and priority of the treatment population have become an important issue. The NHIA held the “Public Hearings of Hepatitis C Treatment in Taiwan” on 14 September 2016, and representatives of the industry, government, professionals, physicians, pharmacists, patients, and legislators were invited to join the meeting. The opinions and advice from all sectors were collected to build strategies for preventing and treating hepatitis C.
By the time the new direct-acting antiviral agents for hepatitis C were launched in Taiwan, their prices were high, at more than New Taiwan dollars (NTD) 1 million for each treatment course. Therefore, the NHIA made every effort to negotiate with pharmaceutical firms for a price reduction. Meanwhile, the NHIA invited experts, scholars, and representatives of the medical providers, pharmaceutical firms, and patient groups to join a public hearing and then negotiated the budget in the National Health Insurance Committee (NHIC). Finally, the Ministry of Health and Welfare (MOHW) approved a 2017 budget of NTD 3.101 billion for the medications used for hepatitis C on 2 November 2016. Furthermore, the NHIA established a registry system for new, direct-acting antiviral agents for hepatitis C. The NHIA formally announced the “Implementation Plan of the Payment for New Direct-Acting Antiviral Agents for Hepatitis C in the National Health Insurance” and began to pay for the new direct-acting antiviral agents for hepatitis C on 24 January 2017.
As the MOHW is expecting that Taiwan could be a role model in the World Health Organization (WHO) and the World Health Assembly, the MOHW further proposed that Taiwan could achieve the WHO goal of eliminating hepatitis C by 2025. Therefore, the NHIA continues to receive higher budgets for hepatitis C medication in the NHIC and expands the reimbursement indications for the disease. Since 2019, patients infected with hepatitis C virus can be reimbursed for new direct-acting antiviral agents for hepatitis C without the limitation of being diagnosed with liver fibrosis.
According to National Hepatitis C Program Office estimates, there are about 405,000 hepatitis C patients in Taiwan. In the past, nearly 80,000 people have been successfully treated with interferon. To achieve the goal of eliminating hepatitis C, 250,000 people must receive new drug treatment. From 24 January 2017, to 31 December 2020, a total of 111,000 people have been treated with new drugs, and the treatment coverage rate is about 47.2%. We are almost halfway done in accomplishing the goal of eliminating hepatitis C in Taiwan by 2025.
Currently, we already have effective treatment for hepatitis B and C. The problem that we are facing in the future is to find people who don’t know they are infected with hepatitis B and C. The MOHW has expanded the eligible age for subsidized adult preventive care service for hepatitis B and C screening, which is 45–79 years old, and the data can help the NHIA find patients.
Medical Device Reform Under National Health Insurance
Since the NHI first started operating 27 years ago, many efforts have been made to protect the health of all citizens. However, owing to the rapid development of new medical devices and the increasingly sophisticated functions and designs, the prices of devices are also rising. According to the statistics data, self-paid medical devices have increased annually to about 2750 items in 2020, and the total medical cost of self-paid medical devices is five times higher in 2020 than it was in 2014. People often question why the NHI does not cover new medical devices, and the other question is how to make the decision between NHI medical devices or self-paid ones.
As medical devices are highly professional products, the NHIA proactively cooperates with clinical professionals, takes clinical need as the main consideration, and promotes the reform of NHI medical devices to ensure the rights and interests of the public. After thoughtful and attentive discussion, there are three main problems:
-
1.
The functions and types of self-paid medical devices are complicated, but which one is indispensable in the clinic?
-
2.
How is coverage for new devices gradually expedited within the limited global budget?
-
3.
Insufficient knowledge and information of medical devices leaves the public with limited choice.
Adding New Functional Categories of Medical Devices Based on Clinical Needs
Most people think that the items of the medical services and medicines paid for by the NHI should meet most people’s “basic” medical needs. The NHI cannot cover all medical services, such as expensive new medical devices. If people want to use them, it is reasonable for them to pay for them themselves. Some people compare the NHI medical devices and special materials to domestic-made cars, people should pay more if they want to drive a Mercedes. However, this is not the way the NHI medical devices and special materials are classified. Different vehicles, such as sedans or SUVs, have different fuel tank sizes, equipment, and other settings. Choices have to be made according to the “function categories” and people’s financial capabilities. Therefore, the medical devices under coverage of the NHI are based on the clinical needs of people. The “basic” medical needs are evolving with the times. Medical materials will be chosen for NHI coverage and classified based on the suggestions of medical associations and medical professionals. For the “clinical results” of the NHI medical devices, special materials, and self-paid medical devices, the comparison should be made on the basis of similar functional categories. In other words, it is more logical to compare medical materials with the same design purpose and similar clinical utilities, for example, comparing the nonlocking bone plate system and locking bone plate system used for fracture fixation.
Claims for Self-Paid Medical Devices Are Increasing
The NHIA has noticed that self-paid medical devices have gradually become the mainstream by analyzing the NHI claims data, while people continue to ask why does this belong to self-paid medical devices and why is that uncovered? Does this mean that the NHI medical devices and special materials have not met the basic clinical needs? Therefore, the NHIA checked all self-paid medical devices and found that nearly 60% are used for bone and neurological surgery and treatment. There are some self-paid medical devices that have similar functions to the NHI medical devices and special materials, but more than half of the claims are out-of-pockets, such as the locking plate system for fixing fractures (around 83%), intramedullary nails (around 58%), suture anchors for fixing soft tissues (around 60%), and artificial knee articular surface for treating degeneration (around 54%). It is even necessary for some of the self-paid medical devices to be covered, such as bone cement for spinal surgery, artificial cervical intervertebral discs that can maintain mobility for nonfusion surgery, and transcatheter replacement aortic valve sets required for new heart valve treatment techniques. Therefore, for these clinical indispensable devices with no similar NHI covering items provided, the NHIA, as the insurer of the NHI, has the responsibility to proactively strive for budget and cover medical devices to meet medical needs.
The NHIA faces these problems pragmatically and is promoting reforms progressively. We understand that medical devices are professional products, and clinicians are the frontline staff who understand the needs of patients the best. Therefore, we invite clinical experts from the medical associations, hospital representatives, and medical device license holders for communication and collect professional opinions on the clinical demand and how to set reasonable prices. At the same time, the NHIA has commissioned the Center for Drug Evaluation to establish a “value appraisal for progressing medical devices” to objectively evaluate the “clinical results” of the new medical devices, by collecting the evaluation results from clinical experts on the improvement in the treatment effect, patients’ quality of life, medical cost efficacy, convenience in clinical operation, decrease in the adverse effects, and with the HTA report as a reference to the special medical materials expert consultation meeting. Then, the medical professionals will provide suggestions on whether to include the items in the NHI coverage or not.
Take transcatheter aortic valve implantation (TAVI), for example. It is a device for treating patients with severe aortic valve stenosis who cannot undergo surgery or for whom surgery is high risk. The NHIA used a value appraisal scheme to evaluate the new medical device, because it is a “new medical device with new medical technology” with no similar functional NHI medical devices and special materials. The NHIA has held three meetings to discuss with the cardiology-related specialty associations regarding this clinical “gap.” Based on HTA reports and clinical professional recommendations, the proposal was discussed within the National Health Insurance Pharmaceutical Benefit and Reimbursement Scheme (PBRS) Joint Committee in November 2020, and was finally agreed to be covered by the NHI with full coverage from 1 February 2021. In addition, for artificial cervical intervertebral discs used in nonfusion spine surgery, the NHIA has also held seven meetings successively to communicate with relevant medical associations such as neurosurgery and orthopedics and will discuss reasonable payment as soon as possible. To increase clinical medical device choices for physicians, one HTA after another has been launched for self-paid medical devices, which are gradually replacing the NHI medical devices and special materials as the foundation of follow-up clinical professional discussions. The NHIA respects the professional opinions of the medical associations and works with the medical community to make decisions on incorporating new medical devices that truly meet clinical needs into NHI payments.
To increase the functional categories for new NHI medical devices, the NHIA has increased the budget for new medical devices annually, with NTD 522 million in 2017, NTD 610 million in 2018, NTD 585 million in 2019, NTD 400 million in 2020, and NTD 650 million in 2021. With collaboration with the medical community, NHIA hopes to gradually close the gap between clinical need and NHI medical device coverage.
Management of Balance-Billing of Medical Devices/Materials
As the medical industry develops and the population ages, the clinical demands for new medical devices increase. Building a sustainable NHI system under the limited NHI resources has always been the most important challenge for the NHIA. For this reason, second-generation NHI collects expensive medical devices that are more effective than the fully covered medical devices and special materials, and with unclear cost-effectiveness, as balance-billing materials. The NHI payment will cover part of the cost, whereas the rest will be paid by the patients. As a result, more new medical devices will be covered by the NHI payment, which increases the accessibility of new medical devices to patients.
In the past, the NHIA determined the payment of balance-billing medical devices based on the payment price of the most similar functional category item. However, it is difficult to find proper reference items owing to the rapid technology progressing or the balance-billing medical devices are too expensive to achieve the benefits of balance-billing. With the rapid development of the industry, most of the new medical devices have a short life cycle and clinical trials are not conducted before marketing. The industries often claim that the functional effect of the expensive devices is different from that of the NHI medical devices and special materials because of the patented design. However, the devices lack clinical evidence for the NHIA to determine reasonable payment. Therefore, the NHIA has promoted pragmatic reforms to incorporate the spirit of the “co-payment” into the payment method for NHI medical devices and special materials. To implement clinical evidence-based evaluation, the NHIA collects the true benefits of self-paid medical devices in clinical use and evaluates the difference between them and the NHI medical devices. The NHIA discusses the appropriate function/material classification with clinical professionals, and gradually includes clinically necessary self-paid medical devices into the NHI payments and pays reasonably based on clinical evidence. As a result, the NHI can take both finance and the richness of the NHI medical devices into consideration and implement the spirit of user charge at the same time.
To increase the types of the new medical devices for clinical application, the NHI strives to cooperate with the specialist medical associations to collect the items and pay at a reasonable balance-billing price. In the future, the NHIA will continue to follow the data on safety and efficacy to review the payment ratio, hoping to increase the clinical use of new medical devices, and clarify whether the self-paid medical devices are as effective as those claimed for by the public.
Information Transparency Enhances Shared Decision-Making Between Physicians and Patients
To help the public understand and search for the charging status of balance-billing medical devices in medical institutions and in order to increase information transparency, the NHIA established the “Price Comparison Platform of Medical Devices” in June 2014. . This platform is for NHI-contracted institutions to autonomously upload medical device charging information to facilitate accessibility to the public, and provides the public with a reference for choosing medical devices after comparison. The data are uploaded and self-checked by the contracted institutions. To improve the accessibility of the information, the NHIA carried out the following strategies:
-
1.
Upgraded the app and Web function of the Price Comparison Platform of Medical Devices
-
(a)
To help the public inquiring about information, the NHIA gradually improved the function of the Price Comparison Platform of Medical Devices. The searching steps are as follows: Go to the Price Comparison Platform of Medical Devices, select the “Balance-Billing Item Charging Situation” tab, select “medical device” and “function/material classification,” and then click the “Query” button to find out how the medical devices are charged in various NHI-contracted institutions. Advanced queries, such as specific counties and cities where the contracted institutions are located, contracted categories. and specific institutions, can also be searched in the query column; you can also search for the highest and lowest fees for each medical device item in the NHI-contracted institution (Fig. 9.7).
-
(b)
The Price Comparison Platform of Medical Devices can also be queried in the National Health Insurance Mobile Easy Access mobile application (NHI Express app). The search steps are as follows: open the app and go to the page of the Price Comparison Platform of Medical Devices. After reading the description page of the Balance-billing Medical Device , click “Go to Inquiry.” Select “medical device” and “function/material classification” and click the “query” button to find out the charging information for the medical device in contracted institutions (Fig. 9.8).
-
(a)
-
2.
Open data for the public
The NHIA also published the Price Comparison Platform of Medical Devices data on the NHI Open Data website (https://data.nhi.gov.tw/Index.aspx) and structured the classification of functions and materials of the various balance-billing medical devices to facilitate accessibility to the user by direct application. In the future, the NHIA will continue to evolve the search function of the Price Comparison Platform of Medical Devices and optimize the website with the goal of being easier to “use,” “search,” and “compare” to improve the transparency and accessibility of information and enhance the communication between physicians and patients to achieve shared decision-making.

Steps for usage of the Price Comparison Platform of Medical Devices web page

Steps for usage of the Price Comparison Platform of Medical Devices app
Conclusion
With the development of medical technology, personalized precision medicines have become mainstream cancer treatments. In response to accomplishing the goal of eliminating viral hepatitis by 2030 from the WHO, the coverage for hepatitis B and hepatitis C medications in the NHI has also been gradually expanding along with the latest clinical development. The NHIA makes efforts to safeguard the medical benefits and rights of the patients. Despite the rapid development of various medical technologies, medical expenses have also risen greatly, causing financial burdens on the NHI. The NHIA shoulders its responsibility and continues to work with the medical providers on good communication and focuses on seeking the balance between financial and clinical needs.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2022 The Author(s)
About this chapter

Cite this chapter
(Mary) Tai, HY., Chang, YP. (2022). Coverage of Advanced Treatments and Medical Devices. In: Lee, PC., Wang, J.TH., Chen, TY., Peng, Ch. (eds) Digital Health Care in Taiwan. Springer, Cham. https://doi.org/10.1007/978-3-031-05160-9_9
Download citation
DOI: https://doi.org/10.1007/978-3-031-05160-9_9
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-05159-3
Online ISBN: 978-3-031-05160-9
eBook Packages: MedicineMedicine (R0)