
Abstract
This chapter summarizes the current state of research on social status, social relations, and health. The focus is on two questions: (1) Is there evidence of an explanatory contribution of social relationships on the association of social status and health (mediating effect of social relationships), and (2) do associations of social relations and health vary in different social status groups (moderating effect of social status)? There is evidence that social relationships can help explain health inequalities. The current state of research on the moderating effect is less clear. Although there are indications of a moderating effect, the results for both questions vary greatly regarding indicators used for social relationships or health. Research on these questions has so far neglected a more complex measurement of social relations, such as in social networks. Complex assessments of social relations might help in finding more detailed insights.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


-
The differential exposure hypothesis assumes that the link between social status and health also exists, because lower status groups have fewer social contacts and less social support.
-
The hypothesis of differential vulnerability assumes that it is precisely in lower social status groups that a lack of social relationships has a greater impact on health.
-
The majority of study results to date can confirm the hypothesis of differential exposure (mediator effect of social relationships).
-
The state of research on the hypothesis of differential vulnerability is rather inconsistent; there is little evidence of a moderating effect of social status on the relation between social relationships and health.
1 Introduction
This chapter aims to provide an overview of research on the links between social relationships, social status, and health. Social relations can be understood as an overarching concept that encompasses various aspects of social relations. Comprehensive indicators of social networks can hardly be identified in any study (see chapter “Network Analysis and Health Inequalities: A Methodological Introduction”). In studies on this topic, the indicators used range from quantitative aspects such as social integration and the number of social contacts to qualitative aspects of social relations such as social support and social capital, measured on a small scale. In accordance with this diversity, social relations are used as an overarching category.
In the context of this chapter, the state of research is presented in relation to two central questions:
-
Mediator effect of social relationships: Are there studies that have found a contribution of social relations to explain the links between social status and health?
-
Moderator effect of social status: Is there evidence that social status moderates the relationship between social relationships and health, and does the relationship between social relationships and health vary in different status groups?
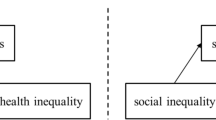
The first question aims to show that social status has an impact on health, precisely because different status groups have different social relationships (see Fig. 1). The so-called differential exposure hypothesis assumes that the relationship between social status and health can be explained by lower status groups having fewer social contacts and less social support. Therefore, health risks of low social status groups are more pronounced (Krause, 2001). Social relations could thus contribute to an explanation of health inequalities, since they act as a mediator between social status and health.

Explanatory contribution of social relations regarding the link between social relations and health (c–c′) (thesis of status-specific exposure). Source: Own illustration
The second question assumes that the links between social relationships and health vary according to status groups (see Fig. 2). According to this assumption, lower status groups in particular have a higher health vulnerability, precisely due to insufficient social contacts and social support. This assumption is reflected in the differential vulnerability hypothesis (Krause, 2001). Hence, a stronger connection between social relations and health can be found especially in lower status groups, and social status moderates the connection accordingly.

Moderating effect of social status (a) on the associations between social relations and health (b) (thesis of status-specific vulnerability). Source: Own illustration
2 State of Research
2.1 Mediator Effect of Social Relations
In the so-called path model by Berkman and Krishna (see Fig. 3), various aspects of social relationships can act as mediators for the relation between socioeconomic status and health. The model shows possible paths of socioeconomic factors on different aspects of social relationships and on health. The mediator function of social relationships, that is, the question of the extent to which social relationships can explain the links between social status and health, has already been explored in various studies.

The path model of the connection between social relations and health according to Berkman and Krishna. Source: Berkman and Krishna (2014)
Cohen and colleagues studied the links between social support, social status, and subjective health (Cohen et al., 1999). After showing that social support is positively associated with both higher social status and perceived health, the explanatory contribution of social support was explored. The explanatory contribution of social relationships was most pronounced in the lower status groups (Cohen et al., 1999).
Gorman and Sivaganesan (2007) found no evidence of a complete mediator effect of social relationships. However, their subgroup analyses showed that the links between individual status indicators and subjective health decreased after controlling for social relations. Particularly unemployed persons seemed to benefit from social integration in terms of their subjective health, since the negative effect on health could be significantly mitigated by social integration (Gorman & Sivaganesan, 2007).
In their analyses based on cross-sectional, representative data from Norway, Dahl and Malmberg-Heimonen (2010) found no mediator effect on social relations regarding the relationship between socioeconomic status and health. Social relationships were determined especially at the level of social capital, using both emotional and instrumental support, as well as the number of personal contacts, as indicators. However, none of the indicators used contributed to a significant reduction in the relation between social status and health. The health indicators used in the study were subjective health and information on chronic diseases (Dahl & Malmberg-Heimonen, 2010).
Knesebeck and Geyer (2007) also examined the extent to which social support may help explain the links between social status, measured by education, and subjective health. They limited their analysis to emotional support. Based on analyses of the European Social Survey of 2003, the authors found little evidence that emotional support can help explain health inequalities. The country-specific analysis only showed explanatory contributions of emotional support for few countries. There was no evidence that emotional support leads to different explanatory contributions of health inequalities between men and women.
Kroll and Lampert (2011) found an effect of social support on the association of unemployment and health impairments. They found that those unemployed who reported sufficient social support were more likely to have less health impairments than those who had little social support. These results were based on a cross-sectional, representative telephone survey in Germany.
Huurre et al. (2007) found no evidence in their study that social support can help explain the link between socioeconomic status and depression in young adults, based on data from a Finnish cohort study.
Aida et al. (2011) provided a further indication that social relationships can possibly buffer the relation between social status and health, especially for older people. Using their analysis based on ross-sectional data from an ongoing Japanese cohort study, the authors were able to show that for the population under study, social capital at the community level, such as the number of club memberships and general trust in the community, contributed to a reduction in the correlation between social status and subjective health. However, no contributions were found to explain indicators of social capital at the individual level.
In analyses regarding the links between social inequality, social cohesion, and mental health, Fone et al. (2007) showed that not only socioeconomic status influenced the probability of weaker mental health, but that the interaction between low status and weak social cohesion within the neighborhood significantly increased the probability of poor mental health.
Overall, there are different indications of the explanatory contribution of social relationships on health inequalities. Depending on the health indicators used or aspects of social relationships, the explanatory contributions vary significantly. In addition, the selection of the target population plays an important role as research on social relations in old age shows. In a review regarding the extent to which material, psychosocial, or behavioral aspects make a greater contribution to explaining health inequalities, Moor et al. (2017), after analyzing the literature, conclude that material aspects in particular contribute to the explanation. However, the authors stress that the effects of material aspects also have an indirect effect on health inequalities via psychosocial and behavioral aspects.
2.2 Moderator Effect of Socioeconomic Status
Evidence that socioeconomic status moderates the links between social relationships and health is found in a French cross-sectional study (Heritage et al., 2008). The authors were able to show that the associations between weak social relationships and poor subjective health are strongest particularly in lower status groups, while the correlations were less clear in upper status groups.
Gorman and Sivaganesan (2007) found clear differences in the relation between hypertension and social integration—measured by the number of contacts with family and friends in the last 2 weeks before the survey—between different status groups. It was found that people without a high school degree also showed higher risks of hypertension with increasing social integration. However, this picture changed completely when the results of the study were monitored for higher education groups: Here the probability of developing high blood pressure decreased with increasing social integration (Gorman & Sivaganesan, 2007). It was found that, especially in higher status groups, the probability of good subjective health rose with increasing social contacts. However, these analyses were based on cross-sectional analyses.
An analysis based on data from the French GAZEL cohort study provided evidence that socioeconomic status moderates the relationship between social relations and health (Melchior et al., 2003). However, different results were found for women and men. In particular, men in higher occupational positions showed the strongest associations between social relations and subjective health: a low level of social support led to a significantly higher risk of poor subjective health than in the other occupational groups that were studied. For women, very similar associations were found across different occupational groups, so a moderating effect of social status cannot be seen (Melchior et al., 2003).
A Finnish cohort study on young people and adolescents found evidence that the strength of the relation between social relationships and health varied according to social status (Huurre et al., 2007). Depression was used as a health outcome. Social relationships were measured by information on social support and the size of the personal network. Results showed that, especially in families where the principal earner worked in manual labor, the relationship between depression and indicators of social relations was stronger than in families where the principal earner was not employed in manual labor (Huurre et al., 2007).
3 Discussion and Significance of Social Networks
3.1 Mediator
The explanatory share of social integration refers to the social environment and social space in which interactions take place. The social space also refers to the different structures in which these actions happen and also the contexts in which they take place. Actions that are intended to change the interaction of individuals in a particular area or community in a positive way also represent a change of context. The importance of contexts for health and health inequalities shifts the focus of attention away from individual factors to social structure (Frohlich et al., 2001). One contribution of social integration to mitigating negative health effects of low social status refers to circumstances that are not necessarily linked to individuals, but rather to the social environment. According to Frohlich et al. (2001): “Consequently, material/structural factors in health inequalities research are frequently studied as proxies for social structure and each variable is not understood in terms of its relation to other elements in the system, nor in terms of how it is manifested in and reinforced by social practices” (Frohlich et al., 2001, p. 781). The reference to social practices suggests that the importance of social relations in explaining health inequalities points to more than the mere existence of individual risk factors. Structures within societies, which certainly include social environment, can also influence individual behavior. The context of individual actions results from the interaction of restrictions and possibilities; thus, individual actions can be explained on a structural level. However, the context is also changed and reinterpreted by individual actions. In the authors’ view, these mechanisms of recursiveness between context and individual demonstrate that individualizing concepts such as “lifestyles” cannot fully contribute to an explanation of collective social practices (Frohlich et al., 2001). The above mentioned findings suggest that social relationships, especially social integration, can contribute to an explanation of the links between social status and subjective health, pointing towards the role of mediating factors (“agency”). These are possibly associated with the development and sustainability of certain social practices within limited social spaces.
Approaches to interventions on social relationships have also been discussed in order to reduce health inequalities. These range from adaptating the living environment (Eriksson & Emmelin, 2013) to influencing health-related behavior and thus increasing social control (Conklin et al., 2014). When health can benefit from the effect of social relations, then the quality of the immediate living environments in which social interactions take place plays an important role. Kawachi and Berkman have shown in their review that social integration and a high degree of social interaction are more likely to contribute to health-promoting behavior and the development of health-promoting norms. It can also be assumed that within well-organized neighborhoods and communities, access to health care and also to health-related knowledge is easier (Kawachi & Berkman, 2001). As previously mentioned, qualitative characteristics of housing and living conditions, which can promote or hinder integration and interaction, are closely linked to socioeconomic resources, particularly income. These structural differences in living conditions also affect the utilization of protective factors in housing conditions. Not everyone has the opportunity to benefit from favorable housing conditions. Unfavorable housing conditions within socioeconomically disadvantaged neighborhoods and communities have a negative impact on health, as some studies have already shown (Dragano et al., 2007, 2008; Mujahid et al., 2008).
Especially against the background of more complex measurements of social relations and the resulting different explanatory contributions of indicators of the social network or the qualitative aspects of social relations, different possibilities of interventions arise. While a higher explanatory contribution of social support points clearly to more resources within social relationships, a stronger mediating effect of social network indicators points more strongly to the possible improvement of social interactions in the populations studied. In their cross-sectional study, Salonna et al. (2012) showed that not all aspects of social relationships per se can contribute to an explanation of health inequalities. They suggest that future research on this topic should take a more omplex approach on social relationships. In addition, further research should examine other facets of social relations in addition to the quantitative and qualitative aspects of social relations—permanent conflicts, the range of social networks, and also the increasing importance of virtual social networks.
Social relationships cannot be considered positive per se (see chapter “Negative Ties and Inequalities in Health”). Not every form of social support or social contact can help mitigate the negative health effects of low social status. For the results presented here, this means that a future detailed consideration of negative aspects, such as social isolation or conflicts within social relationships, could have an influence on the identified explanatory contribution of social relations on health inequalities. It is possible that particularly individuals and groups with lower status may have less access to resources within communities due to exclusion processes and thus may ultimately be more vulnerable to health inequalities (Portes, 1998; Abel & Frohlich, 2012; Uphoff et al., 2013). Social processes that promote the exclusion of lower status groups and thus impede their access to social capital within communities often have corresponding health consequences (Subramanian et al., 2002; Uphoff et al., 2013). From this perspective, it therefore seems important that future research projects include negative aspects of social relations in their analyses. Even the feeling of being overwhelmed by social networks can have negative health consequences. People who are particularly active in social relationships might feel overwhelmed, as there may not be enough time to fulfill corresponding social roles within these networks to a satisfactory extent (Macinko & Starfield, 2001; Mansyur et al., 2008; Gorman & Sivaganesan, 2007).
3.2 Moderator
Overall, the results of studies to date regarding a moderating effect of social status on the links between social relations and health are largely inconsistent. The studies found on this topic varied considerably with regard to status and relationship indicators used, and the results also varied depending on the health indicators used. In a review Uphoff et al. (2013) present an overview of studies that examine the moderating effect of social status on the relation between social capital and health. Some of the studies included in the review conclude that especially people from lower status groups benefit from the effects of social capital in terms of health. In studies that confirm these findings, there are significantly stronger associations between social capital and health in lower status groups compared to upper status groups. However, the results of some of the studies cannot be generalized due to the chosen populations and the selected health outcomes.
On the basis of his comments on the various forms of capital, Bourdieu also discussed the mutual conditionality of the three main forms of capital (Bourdieu, 1986). Accordingly, social relations and the social capital they contain can only be properly used and applied when economic and cultural capital is also available, which in turn enables access to social contacts and their continuation. Conversely, this would mean that people from lower status groups have less social capital and therefore use it less effectively for their health; that is, they are not able to benefit from the possible positive effects (Uphoff et al., 2013). This does not necessarily have to be in contrast to previous research findings: People in lower status groups may particularly benefit from bonding social capital, but they lack bridging social capital. Bonding social capital refers to ties between similar network members, mostly within a given social network. It reflects the social cohesion of social groups. Bridging social capital “bridges” across different social groups and does not necessarily connect similar others. It can be linked to solidarity or social justice within a society as a whole. A further assumption regarding the connection between social relations and health is that within social communities with sufficient social capital there are also people who do not benefit from it. If social capital is available especially to those with higher social status, it can accelerate exclusion processes and lead to permanent exclusion of others. This holds particularly true for contextual social capital, which is social capital that is available within social communities but is not equally accessible to everyone within the community. In this respect, such a process can also contribute to an increase in health inequalities, as permanent exclusion can also have negative effects on health (Uphoff et al., 2013).
Moreover, it was shown that a moderating effect of social status does not occur equally for all aspects of social relations. A differentiation should be made between quantitative and qualitative aspects, since these can be associated with health in different ways, even against the background of social status.
4 Summary and Conclusion
There is a wide variety of studies on the different links between social status, social relations, and health. However, this diversity, especially due to the indicators used, does not allow for a comparability of results. This is especially true for the different indicators of social relations, but also for health indicators and, with certain limitations, status indicators. For both research questions, the study situation is rather heterogeneous; overall, there is less evidence for a moderating effect of social status than for an explanatory contribution of social relationships to health inequalities. There is stronger evidence for the latter on the basis of longitudinal analyses. However, in most cases the explanatory contribution remains rather small and, compared to other explanatory approaches, tends to lag behind. There is still a need for further research on the question of how the individual explanatory approaches to health inequalities are mutually dependent and how they are related to one another (see Moor et al., 2017).
A more complex and multidimensional assessment of social networks, which covers different aspects of social relations, could lead to a better comparability of results across different network and relational indicators. In addition, by looking at smaller social networks, statements can be made about the social environment that go beyond the previous standard of ego-based surveys. What is the relation between network members, how exactly are resources distributed within the networks, and what influence do such aspects have on health? These questions could be answered more concretely when referring to the socioeconomic status of both the respondents and the network members. It remains to be seen whether these questions will actually lead to better answers to the two central research questions in this area. With increasing technical possibilities, improved survey instruments, and more complex analysis methods, it would be desirable to reach a more detailed perspective on the links between social status, social networks, and health in the future.
Reading Recommendations
-
Berkman, L. F., & Krishna, A. (2014). Social network epidemiology. In L. F. Berkman & I. Kawachi (Eds.), Social Epidemiology (pp. 234–289). Oxford University Press. Detailed and systematic overview of the relationship between social networks and health.
-
Uphoff, E. P., Pickett, K. E., Cabieses, B., Small, N., & Wright, J. (2013). A systematic review of the relationships between social capital and socioeconomic inequalities in health: a contribution to understanding the psychosocial pathway of health inequalities. International Journal for Equity in Health, 12(54). One of the very few systematic reviews in the field that considers aspects of social relationships, social status, and health.
-
Moor, I., Spallek, R., & Richter, M. (2017) Explaining socioeconomic inequalities in self-rated health: a systematic review of the relative contribution of material, psychosocial and behavioural factors. Journal of Epidemiology & Community Health, 71, 565–575. A recent review of how health inequalities can be explained and which aspects in particular contribute to an explanation.
References
Abel, T., & Frohlich, K. L. (2012). Capitals and capabilities: Linking structure and agency to reduce health inequalities. Social Science and Medicine, 74(2), 236–244.
Aida, J., Kondo, K., Kondo, N., Watt, R. G., Sheiham, A., & Tsakos, G. (2011). Income inequality, social capital and self-rated health and dental status in older Japanese. Social Science and Medicine (1982), 73(10), 1561–1568.
Berkman, L. F., & Krishna, A. (2014). Social network epidemiology. In L. F. Berkman & I. Kawachi (Eds.), Social epidemiology (pp. 234–289). Oxford University Press.
Bourdieu, P. (1986). The forms of capital. In J. Richardson (Ed.), Handbook of theory and research for the sociology of education (pp. 241–258). Greenwood.
Cohen, S., Kaplan, G. A., & Salonen, J. T. (1999). The role of psychological characteristics in the relationship between socioeconomic status and perceived health. Journal of Applied Social Psychology, 29(3), 445–468.
Conklin, A. I., Forouhi, N. G., Surtees, P., Khaw, K. T., Wareham, N. J., & Monsivais, P. (2014). Social relationships and healthful dietary behaviour: Evidence from over-50s in the EPIC cohort, UK. Social Science and Medicine (1982), 100(100), 167–175.
Dahl, E., & Malmberg-Heimonen, I. (2010). Social inequality and health: The role of social capital. Sociology of Health and Illness, 32(7), 1102–1119.
Dragano, N., Bobak, M., Wege, N., Peasey, A., Verde, P. E., Kubinova, R., Weyers, S., Moebus, S., Möhlenkamp, S., Stang, A., Erbel, R., Jöckel, K.-H., Siegrist, J., & Pikhart, H. (2007). Neighbourhood socioeconomic status and cardiovascular risk factors: A multilevel analysis of nine cities in the Czech Republic and Germany. BMC Public Health, 7(1), 255–267.
Dragano, N., Hoffmann, B., Stang, A., Moebus, S., Verde, P. E., Weyers, S., Möhlenkamp, S., Schmermund, A., Mann, K., Jöckel, K.-H., Erbel, R., & Siegrist, J. (2008). Subclinical coronary atherosclerosis and neighbourhood deprivation in an urban region. European Journal of Epidemiology, 24(1), 25–35.
Eriksson, M., & Emmelin, M. (2013). What constitutes a health-enabling neighborhood? A grounded theory situational analysis addressing the significance of social capital and gender. Social Science and Medicine, 97, 112–123.
Fone, D., Dunstan, F., Lloyd, K., Williams, G., Watkins, J., & Palmer, S. (2007). Does social cohesion modify the association between area income deprivation and mental health? A multilevel analysis. International Journal of Epidemiology, 36(2), 338–345.
Frohlich, K. L., Corin, E., & Potvin, L. (2001). A theoretical proposal for the relationship between context and disease. Sociology of Health and Illness, 23(6), 776–797.
Gorman, B. K., & Sivaganesan, A. (2007). The role of social support and integration for understanding socioeconomic disparities in self-rated health and hypertension. Social Science and Medicine, 65(5), 958–975.
Heritage, Z., Wilkinson, R. G., Grimaud, O., & Pickett, K. E. (2008). Impact of social ties on self reported health in France: Is everyone affected equally? BMC Public Health, 8, 243.
Huurre, T., Eerola, M., Rahkonen, O., & Aro, H. (2007). Does social support affect the relationship between socioeconomic status and depression? A longitudinal study from adolescence to adulthood. Journal of Affective Disorders, 100(1-3), 55–64.
Kawachi, I., & Berkman, L. (2001). Social cohesion, social capital, and health. In L. F. Berkman & I. Kawachi (Eds.), Social epidemiology (pp. 174–190). Oxford University Press.
Knesebeck, O. V. D., & Geyer, S. (2007). Emotional support, education and self-rated health in 22 European countries. BMC Public Health, 7, 272.
Krause, N. (2001). Social Support. In R. H. Binstock & L. K. George (Eds.), Handbook of aging and the social sciences (pp. 273–294). Academic Press.
Kroll, L. E., & Lampert, T. (2011). Unemployment, social support and health problems: Results of the GEDA study in Germany, 2009. Deutsches Ärzteblatt International, 108(4), 47–52.
Macinko, J., & Starfield, B. (2001). The utility of social capital in research on health determinants. Milbank Quarterly, 79(3), 387–427.
Mansyur, C., Amick, B. C., Harrist, R. B., & Franzini, L. (2008). Social capital, income inequality, and self-rated health in 45 countries. Social Science and Medicine, 66(1), 43–56.
Melchior, M., Berkman, L. F., Niedhammer, I., Chea, M., & Goldberg, M. (2003). Social relations and self-reported health: A prospective analysis of the French Gazel cohort. Social Science and Medicine, 56(8), 1817–1830.
Moor, I., Spallek, R., & Richter, M. (2017). Explaining socioeconomic inequalities in self-rated health: A systematic review of the relative contribution of material, psychosocial and behavioural factors. Journal of Epidemiology and Community Health (JECH), 71, 565–575.
Mujahid, M. S., Diez Roux, A. V., Morenoff, J. D., Raghunathan, T. E., Cooper, R. S., Ni, H., & Shea, S. (2008). Neighborhood characteristics and hypertension. Epidemiology (Cambridge, Mass.), 19(4), 590–598.
Portes, A. (1998). Social capital: Its origins and applications in modern sociology. Annual Review of Sociology, 24, 1–24.
Salonna, F., Geckova, A. M., Zezula, I., Sleskova, M., Groothoff, J. W., Reijneveld, S. A., & van Dijk, J. P. (2012). Does social support mediate or moderate socioeconomic differences in self-rated health among adolescents? International Journal of Public Health, 57(3), 609–617.
Subramanian, S. V., Kim, D. J., & Kawachi, I. (2002). Social trust and self-rated health in US communities: A multilevel analysis. Journal of Urban Health: Bulletin of the New York Academy of Medicine, 79(4 Suppl 1), S21–S34.
Uphoff, E. P., Pickett, K. E., Cabieses, B., Small, N., & Wright, J. (2013). A systematic review of the relationships between social capital and socioeconomic inequalities in health: A contribution to understanding the psychosocial pathway of health inequalities. International Journal for Equity in Health, 12, 54.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2022 The Author(s)
About this chapter

Cite this chapter
Vonneilich, N. (2022). Social Status, Social Relations, and Health. In: Klärner, A., Gamper, M., Keim-Klärner, S., Moor, I., von der Lippe, H., Vonneilich, N. (eds) Social Networks and Health Inequalities. Springer, Cham. https://doi.org/10.1007/978-3-030-97722-1_11
Download citation
DOI: https://doi.org/10.1007/978-3-030-97722-1_11
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-97721-4
Online ISBN: 978-3-030-97722-1
eBook Packages: Social SciencesSocial Sciences (R0)