
Abstract
Activities of Daily Living (ADLs) refers to the fundamental skills required to care for one-self and live independently and includes dressing, feeding, personal hygiene, continence and transferring. Assessing ADLs is therefore essential, especially for vulnerable population who may need assistance in performing these activities. As current validated scales to measure ADLs capacity are often dependent of an informant or a caregiver and are mainly performed in the controlled settings of the hospital, using technology-enabled tools could benefit individual’s health in terms of disease prevention and treatment but would also enhance individual’s quality of life and independence. This chapter presents 4 standard validated scales for ADLs and the current research activities on the use of technologies to assess one’s ability to perform ADLs, mainly indoor-outdoor mobility and nutrition. A nutrition assessment use case through a conversational agent is presented in the second part of the chapter. Future opportunities for technology-enabled ADL assessment are discussed.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
Developed countries are facing the challenge of ageing societies, lack of infrastructure for healthcare and high cost of care. Researchers have been attempting to answer these problems by using innovative technology to promote healthy ageing [1]. Rather than the absence of disease, “healthy ageing” is defined as a process that enables older people to continue to do the things that are important for them such as performing activity of daily living, maintaining social contact and conserving dignity [2,3,4].
Activities of Daily Living (ADLs) include individual’s basic physical needs such as dressing, feeding, personal hygiene, continence and transferring [5]. To assess individual’s level of independence, researchers and clinicians often measure the ability to perform ADLs’ tasks through different approaches such as self-report and performance-based measures [6]. However, these methods which are commonly completed by caregivers are not completely free of bias and are sometimes subject to under or overestimation of the individual’s true functioning [7].
Besides, the Quantified Self (QS) movement is gaining more and more attention. It is an emerging trend, which allows individuals to self-monitor or self-track their daily life activities, to analyze and self-reflect on their behaviors, and to bring potential change in their daily habits [8, 9]. Furthermore, with the recent development of monitoring technologies and artificial intelligence techniques, the possibilities to automatically distinguish between different ADLs and detect unexpected events such as falls, have become an interesting, important and potentially impactful topic [10]. How efficient these tools are, to assess and improve ADLs, needs further investigations.
This chapter will present the standard validated scales for ADLs and the current researches on the use of technologies to assess one’s ability to perform ADLs, mainly indoor-outdoor mobility and nutrition. To expand our overview on the topic, the focus will be on elderly as well as on younger and healthier individuals. We then follow with a nutrition use case assessment based on a conversational agent called “MiranaBot”.
Conclusive remarks will emphasize the necessity to consider behavioral science along with cultural and environmental context to elaborate personalized monitoring and intervention strategies, which will be translated to innovative solutions to promote independence at home.
State of the Art
Activities of Daily Living (ADLs)
Created by Sidney Katz in 1950 [11, 12], the term “Activities of Daily Living” refers to the fundamental skills required to care for one-self and live independently. ADLs include dressing, feeding, personal hygiene, continence and transferring [5]. ADL dependence is often associated with lower quality of life, higher healthcare costs, higher risk of mortality and institutionalization [13,14,15]. Assessing individual’s ADLs is therefore essential, especially for vulnerable population who may need assistance in performing these activities. In this chapter, the focus will be on indoor/outdoor mobility and nutrition.
Mobility is defined as the ability to move oneself from one point (or state) to another inside and outside the home environment to maintain a certain level of independence [16, 17]. As activity restriction is associated with various physical deconditioning effects and decreased rates of social involvement, mobility is closely linked to health status and quality of life. Researchers has been attempting to propose a mobility model based on multiple factors such as cognitive, social, physical, environmental, financial as well as gender, culture and age, which all may influence individual’s mobility in different way [16]. As people age, decreased mobility is often predictor of falls and physical disabilities [18]. Consequently, there is a growing interest in measuring mobility and determining the factors that influence mobility to strengthen the physical and functional capacities of older adults.
Nutrition capacity or the ability to eat is a part of the essential ADLs to maintain an independent life [5]. Food intake plays a crucial role in individual’s life and momentary, as well as long-term health and quality of life. Research on nutrition science, human nutrition, preventive nutrition, clinical nutrition and public health nutrition has been specifically on the rise the past years [19], to treat and prevent medical conditions such as diabetes [20] or sarcopenia [21] and ensure a better quality of life [22]. Reliably measuring not only the quantity but also the quality and the frequency of food intake is therefore very important to picture one’s nutritional habits and to be able to recommend adapted and personalized advice or treatment to the person.
Validated Scales for ADLs
Several methods, such as self-report, caregiver report, or direct observation, have been used to measure the degree of independence in ADLs. Self-reporting is easy to perform and are often used when direct observation is not possible, or if the person presents no cognitive deficiency. Nevertheless, the self-reports may be biased and less valid when ones have difficulties to evaluate their functional capacity [23, 24]. Performance-based assessments imply in-lab assessment of the individual’s ability and skills for self-care using mock settings, role play and simulation of real-world environment. They may provide accurate information about the ability to execute the ADLs but typically require more qualified assessor to be performed, compared to self-reporting or informant reports. Table 2.1 presents four main validated scales widely used to measure ADLs in older adults or patients with cognitive or mobility impairment as well as their benefits and drawbacks.
Although these scales are validated and standardized, they are, first, often dependent of an informant or a caregiver, which may include biases and, second, mainly performed in the control settings of the hospital. Being able to automatically assess ADLs at the home environment would benefit individual’s health in terms of disease prevention and treatment but would also enhance individual’s quality of life and independence. In the following section, we will review the current researches on the use of technologies to assess one’s ability to perform ADLs, mainly indoor-outdoor mobility and nutrition.
Technology-Enabled Tools to Assess Indoor-Outdoor Mobility
Over the last few years, Global Positioning System (GPS) technology, embedded in personal smartphone, has become the leading solution for outdoor positioning, and new technologies for indoor positioning and navigation exponentially expanded. Smart devices with embedded inertial sensors, radio beacons and image processing are just few examples of the systems deployed to assess indoor mobility. As most of the times, choosing one solution for any type of mobility assessment scenario is proven to be not possible, ongoing developments tend to combine different technologies to find the best balance between precision, cost, robustness, scalability and energy consumption [31]. With respect to the ADLs, such solutions enable assessment of the indoor-outdoor mobility. Some of them may enable recognition of activities such as transfer, use of stairs, dressing, meal preparation or use of rooms (bathroom, toilet and kitchen). Privacy concerns and environmental context recognition are often discussed in the research when choosing one or more systems for assessing mobility. In this section, we will review the current research on systems for mobility measurement by emphasizing two main categories: activity recognition and wireless indoor-outdoor positioning systems.
Activity Recognition
Activity recognition is focusing on distinguishing a person’s activities (sedentary: sleeping, sitting /active: walking, using stairs, cooking, etc.) in a given space is now currently performed using two types of technologies: vision-based systems and sensor-based systems [32, 33].
The vision-based recognition focuses on the processing and evaluation of video data from cameras or low-cost integrated depth sensor. Cameras installed in fixed positions can be fitted to the environment. In this case, the goal is to locate a moving target in images that are taken by one or more cameras [31]. Commons examples include video-based exercise program which allow user, caregiver or family to track daily exercise. Ayase et al. [34] investigated a “multimedia fitness exercise progress notes” which forwarded the video recording of elderly exercise movements to a research center, which were used to identify the duration, the distances and the angle of the movement . Another study [35] tried to analyze sit-to-stand motion from monocular videos by comparing the images received with the motion of a human body model. Li et al. [36] proposed a system that could extract gait features by using images from two orthogonal viewing cameras. Although optical systems show better accuracy nowadays [37], they remain intrusive, costly and are often limited to specific environments in which variable lighting and other disturbances can be controlled. However, attentions are now given to mobile and low-cost solutions based on camera embedded in mobile phone [38, 39]. Kahlert and Ehrhardt [40] used a photo-based ambulatory assessment to measure out-of-home mobility and social participation of older adults. The use of video and image may however be recognized as potentially privacy-threatening.
Sensor-based recognition includes the use of pressure sensors, accelerometers, magnetic sensors and gyroscopes embedded within an environment, where the individual is active (or not). On one hand, smart floors and smart furniture are based on pressure sensitive sensors installed on or under the corresponding materials and focus either on load cell systems or pixelated surfaces. Load cell systems use separated sensors embedded on tiles and try to compute user location by sensing vertical force applied to the tiles [41, 42]. Pixelated surfaces on the contrary embed many sensors working as binary switches when someone is standing or moving on the surfaces [43,44,45]. Other furniture such as chairs and beds can also be embedded with pressure sensors to assess user mobility. Merilampi et al. [46] tested an exergame coupled with a smart chair where users were asked to stand up and sit to play the game. On the other hand, the emergence and progress of wearables technologies have opened a door to develop different tools to assess individual’s mobility. Non-invasive off-the-shelf sensors such as wearables, smart clothes or smartphones have gained more and more attention for their potential to recognize indoor and outdoor activities while being continuously embedded on/around the user. Several reviews [47,48,49] discuss the potential of physical activity monitoring using accelerometry techniques to enable activity measurement of individuals in a free-living environment. Steps and activity intensity are often measured through an off-the-shelf sensors or a smartphone and used to estimate energy expenditure following a physical activity. Furthermore, Berglind et al. [50] showed in their study that smartphone apps can be as efficient as supervised exercise sessions (assessing the activities of the user) to improve body composition and cardiorespiratory fitness.
Wireless Indoor-Outdoor Positioning Systems
Through the past few years, several wireless technologies and techniques have been used and researched to assess indoor-outdoor positioning and navigation. Infrared, Ultrasound, Wi-Fi (Wireless Fidelity), RFID (Radio Frequency Identification), Bluetooth are mainly used indoor [31] while GPS (Global Positioning System) often represent outdoor solution [51].
All of them present advantages and drawbacks, which have to be considered while choosing the right solution. Infrared transmits infrared signals and compute the distance between the emitter and the receiver to locate the user. The main advantages are the absence of radio electromagnetic interference and an adjustable power of transmission. However, it can be costly to implement, less accurate and often requires a line of sight between transmitter and receiver to function properly [52]. Ultrasound systems use similar techniques by transmitting ultrasonic waves to assess the distance between fixed receivers and a mobile target. Synchronization of multiple receivers is then necessary. This system is relatively low-cost and could bypass indoors obstruction, but large-scale implementation remains complex and temperature variation could influence the speed of the sound [53]. Wi-Fi-based and Bluetooth-based systems are also known for being low-cost as it can localize every Wi-Fi compatible device without any extra installation, but it has lower accuracy and could induce large power consumption for smartphone [54, 55]. RFID system works without direct line of sight. Nevertheless, the intensity of the signal depends on the density of the obstacles in the building, and therefore precision is always reduced. However, RFID technology has more benefit such as better data rate, high security and compactness [56]. GPS-based applications are now widely used to track outdoor mobility. GPS-based navigation services are also often investigated in the context of facilitating visually impaired people mobility [57]. When combined with other devices such as accelerometers, the GPS system shows better accuracy in identifying the type of activity [58]. Weber and Porter [59] examined the feasibility of using GPS watch and accelerometers to monitor walking and community mobility in older adults and found promising results for monitoring community mobility patterns.
Technology-Enabled Tools to Assess Nutrition
Regarding techniques and technologies to assess nutrition which is important when assessing the meal preparation and feeding abilities of an individual, we also distinguish between vision-based systems, sensor-based systems and self-assessment via mobile applications.
Ghali et al. [60] designed a system using cameras to provide real-time feedback to stroke patients while performing daily activities such as making a cup of coffee. They used histogram-based recognition methods to compare the recorded movement to a target task model and identify key events. P-W Lo et al. [61] investigated a vision-based dietary assessment approach to estimate food volume by using mobile phone 3D camera, deep learning and deep sensing techniques. They concluded an efficiency in portion size estimation even under view occlusion (food items scanned only from the front view). Pettitt et al. [62] combined micro-camera images with food diaries and improved the accuracy of dietary assessment. Their system also provided valuable information on macronutrient intake and eating rate. Gemming and al [63]. used a wearable camera to capture and categorize the environmental and social context of self-identified eating episodes and found that these contexts could be assessed objectively by using wearable cameras. Most of the eating episodes were at home and indoors, seated at tables or sofas but also standing or at a desk.
Sensor-based systems include the uses of furniture embedded sensors such as smart fork, smart table or smart plate. Zhou et al. [64] developed an unobtrusive smart table surface and were able to distinguish between different eating actions, such as cutting, scooping and poking. They could also indicate the type of food taken and the way the meal is consumed. Qualitative study [65] evaluating smart fork to decrease eating has been conducted and demonstrated user awareness of eating rate. However, the incapacity of the fork to consider meal characteristics, were less appreciated. Huang et al. [66] prototyped a smart utensil which analyzes light spectra reflected by foods that differ for every food ingredient. They could recognize up to 20 types of aliments with 93% accuracy. Mertes et al. [67] proposed a novel plate system that can detect weight and location of individual bites during meals. They used a compartmented plate were filled with different type of food and initially weighed. Depending on the weight variation, they could detect the category of food eaten by the user.
The most common techniques to assess nutrition are through self-assessment via an application or a platform. Todays’ systems are not only trying to measure food intake but based on nutrition habits, recommends healthy diet. Food recommender systems have received increasing attention to help people adopt healthier eating behavior. These systems focus on suggesting appropriate food items based on individuals’ preferences and health conditions [68, 69]. Nevertheless, despite the extensive research and the large number of existing nutrition applications, food recommender systems are still facing many challenges in terms of nutrition habits tracking and delivery of the proper recommendations [70, 71]. People find it often difficult and time consuming to enter manually their food every day in the system. Many studies are also facing the uncertainty of the information given by the users as they may not know or tend to forget what they have eaten which makes it more challenging for the system to recommend the correct food item. Additionally, many studies have shown that the recommendation is not necessarily followed by a change in the behavior [72]. There is still a lack of understanding in how to incorporate efficiently behavior change techniques into a food recommender system.
Use Case: Nutrition Assessment
With the recent development in natural language understanding, conversational agents defined as a dialog system that supports human-like conversational interaction, have gained popularity over the past three years. In the nutrition domain, they allow to collect user data in an easy and user-friendly manner. Researchers have developed a Web-based prototype of a speech-controlled nutrition-logging system, which converts the entry spoken by the users into calories intake [73]. Others researched a chatbot that help people reduce their meat and increase fruits and vegetables consumption [74]. Users were able to set nutrition goals themselves and had a follow-up with the system every day. Although, only 11% could reach their objectives, more than half of the participants showed positive changes in their nutrition habits.
We developed a conversational agent called “MiranaBot” that helps the user to assess their nutritional patterns and to be aware of their eating habits in terms of variety and regularity.
Interviews, observations and focus groups, presented in the methodology below, were conducted to collect the requirements from users and caregivers for an efficient nutritional conversational agent.
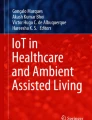
Rather than focusing on food quantity and nutritional value, the system targets the variety of the individuals’ diet. From a regular description of the individual’s meals during a certain period, “MiranaBot” is able to assess the quality of their nutrition, identify the foods they need to consume less, and explain why and how to replace them. The system proposes personalized solutions tailored to the older adults’ needs and context (Fig. 2.1).

Graphical User Interface—MiranaBot—Speech interface
Methodology
We conducted a qualitative study with 10 obese and diabetic patients, 2 nutritionists and 1 physician with a specific expertise on therapeutic education of chronically-ill patients from University of Geneva hospital in Switzerland. Nutrition and overall self-management with respect to nutrition, usually implying the need for nutritional behavior change, plays a vital role in the self-management of disease for these patients; their future health state depends on the daily nutrition patterns. Observation sessions, focus group and semi-structured interviews were performed to get insights from the different participants. The prototype was developed through an iterative process, following the agile development principles [75]. A first prototype was developed within 4 weeks and changes were quickly implemented according to the participants feedback and in collaboration with them.
To understand patient’s current self-management with respect to nutrition, and identify barriers for adopting a healthy nutrition, we first observed 4 consultation sessions led by a physician at the therapeutic education center. In addition, we followed a group of 10 patients for one-week period, while they came to the center for a workshop to learn about their disease. To inquire about their needs and their issues, we conducted a focus group with the patients, while presenting them the first prototype of the application. We conducted a semi-structured interview with one physician and two nutritionists, who helped us to understand the real issues faced by the patients as well as the complexity of nutritional behavior change. The nutritionists participated in creating the nutritional database, we later used in the application.
We then selected the corresponding Behavior Change Techniques (BCTs) from the literature aiming at and answering and fulfilling the needs and requirements identified for the MiranaBot. These BCTs are then converted into a set of functionalities that we incorporated in MiranaBot.
Factors Influencing Nutrition Self-Management
Our observation followed by the discussion with the patients and the health professionals gave us insights on the barriers for patients to adopt a healthy nutrition as well as their needs and requirements for a successful behavior change. N1, N2 and P are used to refer to the nutritionists (N) and the physician (P). Patients are addressed as P1 to P10.
Barriers to Healthy Nutrition
Lack of regularity, lack of variety, false belief and hunger unawareness were identified as the main barriers to healthy nutrition.
Lack of Regularity
Nutritionists identified the lack of regularity in eating as the first issue commonly faced by their patients. N1 said “Most of our patients are not eating three times a day. They are not taking breakfast, neither a lunch, which make them starve for a big quantity of food later during the day or at night.” P6 mentioned “I don’t really have time because of my job, so I’m just grabbing some food that I can easily find when I finish my round. It’s easier like that for me.” P3 added “I don’t eat breakfast, I’m used to that. At lunch, I just grab some sandwiches, but I come back home, I think I deserve a big dinner. I’m usually very hungry at night.”
Lack of Variety
Health professionals also mentioned the lack of food variety as a recurring issue observed in chronically-ill patients. N1 stated “We often share the optimal plate during our workshop because most of our patients have difficulty to bring variety to their food. They are often eating the same aliment every day”. P4 said “I have to admit that I’m always eating pasta and pizza, because I like them, and you know, it’s not expensive.” P9 added “I’m always buying the same thing when I do my groceries. I don’t allow a lot of surprise about my food. I already have my personal habits.”
False Belief
Following a consultation with a patient, the physician shared with us that one of the most difficult issue they face as health professionals is patients’ false beliefs. P said, “As one of my patients heard that olive oil was good for the heart, he started to put a big quantity of olive oil in everything he eats.” During the session with her doctor, P2 shared “You know doctor, I only eat fresh cheese every day. Whatever is the menu, I always have my fresh cheese. It is fresh, so for me that’s healthy.”
Hunger Unawareness
Nutritionists and physician both mentioned the complexity of nutritional behavior change due to the different external and internal factors influencing people to eat. P shared with us “Most of the time, when patients comes here, it is not only about food. It’s about how they face the loss of their loved ones or the family problem they have. It’s much more than a food addiction.” N2 stated “It often happen that the patients do not eat because they feel hungry but rather to fill a void inside them.” P7 added “You know, I just eat automatically because there is food there, I don’t think too much about why.” P4 stated “I’m not always feeling good after eating, that’s how I somehow realize maybe that was too much.”
Needs and Requirements
Monitoring, education, empowerment and practicality were identified as the main needs and requirements and facilitators for nutrition behavior change approach.
Monitoring
Patients and health professionals both shared the need for a monitoring tool to raise self-awareness on patients’ nutritional habits. P5 said “It’s true that I don’t always remember the food I ate. So, I don’t really realize how I eat. If a tool can help me know that, why not?” P7 added “The nutritionist asked me to describe what I ate on a diary, so that she can know how to help me. I guess it’s important to monitor what we eat but it is not always easy.” N2 stated “Just being aware of what and how they eat would already represents a big advancement because a lot of my patients do not even think of how much and why they eat. That’s the real issue. It is essential for them to monitor their eating habits.”
Education
The plethora of nutritional advice and beliefs accessible on the web make it often difficult for patients to identify trustworthy information. Patients appreciated the one-week workshop organized by the hospital as it taught them trustworthy and practical tips to change their habits. P6 said “You know before coming here, I thought drinking smoothie should be fine as it is just fruits. I did not know that fruits also contain sugar and drinking a lot of smoothie is really not healthy.” N1 mentioned “During our session here, we teach our patients to always eat proteins, carbs and vegetable. We share simple tricks to measure portion. Our patients need that.”
Empowerment
From the perspective of the health professionals, there is no “one size fit all” solution for everyone. Their role remains to give the necessary education. It is then up to the patients to build their own strategy and apply it for changing their behavior. P4 effectively confirmed “I won’t like it if you tell me what I have to eat. I should be free to choose what I like as long as I follow your general recommendation.”
Practicality
Most of our participants expressed the need for a practical and simple solution. P8 shared “I used a nutrition application before to record my food, but it was too time consuming, so I gave up.” N2 mentioned “Specifying the quantity of your pasta and beef is not so obvious. Patients need a hands-on tool that would motivate them and make their life easy.”
Summary
Lack of regularity, lack of variety, false belief and hunger unawareness were identified as the main barriers to healthy nutrition; whereas monitoring, education, empowerment and practicality were identified as the main needs and requirements for nutrition behavior change. Considering these findings, we selected appropriate BCTs to include inside our systems, as described in the next sections.
MiranaBot: Behavior Change Theory and Techniques in Action
Multiple researches have been conducted to identify motivational strategies for behavior change, especially in the nutrition and physical activity domain [76, 77]. Studies grounded in behavior theory appeared to show a positive impact on patient health behavior. Sawesi et al. [78] demonstrated a significant relationship between theory-based health behavior change intervention and patient engagement. Various systematic reviews and meta-analysis [79,80,81] showed that efficacy of dietary intervention is associated with well-defined behavior change techniques like: social support, increased contact frequency with the therapeutic team, goal setting, just-in-time feedback on behavior, review of goal progress and self-monitoring.
There are many models and theories on behavior change, some focusing on parts of the behavior change process [82], while others are more holistic, aiming to include all factors that can influence behavior change [83]. “MiranaBot” is based on the Self-regulation theory [84] and the COM-B (Capability, Opportunity, Motivation, Behavior) model [82]. Self-monitoring, personalized visual feedback, goal setting, self-awareness and personalized education were the behavior change techniques incorporated in the tool. Table 2.2 summarizes the mapping of the different requirements, barriers with the proposed BCTs (Fig. 2.2).

Behavior change theories and techniques operationalized within MiranaBot
Self-Monitoring
“MiranaBot” allows the users to track their nutrition easily by asking them to briefly describe what they ate after each meal in terms of portions. The system will assess the portion size and initially train the users on the portion size to help them describe their meals as best as possible.
Personalized Visual Feedback
“MiranaBot” provides visual feedback every day regarding nutrition variety and regularity. Food variety is illustrated on a plate showing the ratio of proteins, carbohydrates and vegetables consumed by the user versus the optimal plate suggested by the Swiss Society of Nutrition [85]. A visual watch resuming the individual’s eating times is intended to encourage self-reflection on their nutrition regularity.
Goal Setting
Following a training period analyzing the eating habits of the users, “MiranaBot” allows them to set personal goals, such as “eating three meals a day” or reducing “bread” and to define a timeline to reach their goals. Prompt reminders and useful information are provided to the users to help them reaching their goal.
Self-Awareness
Research has demonstrated that the reason to eat for most patients with chronic conditions are rather linked to psychological issues (emotions, stress, anxiety) or automatic behavior, than hunger itself [86, 87]. “MiranaBot” raises awareness of real physical hunger by asking users how they are feeling before and after each meal.
Personalized Education
“MiranaBot” is developed to be continuously available to answer users’ questions during the process of change. Advice on food item alternatives, benefits of healthy nutrition behavior and promptly reminders towards their personal goals are frequently delivered.
MiranaBot: Components and Functionalities
“Mirana” refers to the overall system, providing “MiranaBot” service, as one of the components. Figure 2.3 illustrates the process and the different technical modules of the conversational agent. “Mirana” is composed of four main components: the speech to text module, the text analysis module, the natural conversation module and the graphical user interface. We denote as “nuggets” the results of “Mirana” analysis after a certain period of data collection from the individual; focusing on types of foods that may need to be replaced by others, to achieve healthier nutritional outcomes. For example, a nugget could be “bread”, then the recommendation through the natural conversation module or the Graphic User Interface Module would be “let’s reduce bread consumption by ¼ for a week. Here is what you can eat instead of bread”.

Process and components of Mirana, including MiranaBot
Speech to Text Module
Users can easily describe, vocally , what they have eaten after each meal. This voice description is then converted in real time into text using DialogFlow, Google’s human–computer interaction technologies based on natural language conversations.Footnote 1 Data are stored in the secure server of the researcher’s institution in Switzerland. MiranaBot is now available in three languages, namely French, English and Danish.
Text Analysis Module
MiranaBot analyses users’ every day food data to provide them with daily and weekly visual feedbacks. MiranaBot also detects frequencies, varieties, and quantities (in terms of portions) of a specific food (or category of food). With the help of nutritionists and dieticians, we were able to build a database of food classified by categories. We have set rules for each category, which are then used by our algorithm to identify recurring patterns (e.g., eat too much bread = more than the normal consumption defined by the rules).
Natural Conversation Module
One important functionality of “Mirana” is its ability to discuss, have a conversation and answer the questions from the user. As mentioned previously , the conversational module is built upon DialogFlow developed by Google. Their module uses machine learning for small talk conversations to recognize user basic questions. In addition, we developed specific intents (or functions) related to our case to give “Mirana” the ability to answer questions about nutrition.
Graphical User Interface
To maximize the output provided to the user, MiranaBot uses the screen of the host device (phone, tablet, computer) to display graphical feedback in addition to the vocal answers. The regularity of the nutrition and the variety of the food eaten by the users are displayed on the screen to induce better self-reflection. While describing their food, the user can also check, in real time, if what they said was transcribed correctly. In case of error, they have the possibility to edit the entry through the graphical user interface. The user interface is also used to share articles, tips or to send useful notifications to the user.
Conclusions
This chapter reviews existing validated scales to measure ADLs and different technology-enabled tools, methodologies and strategies currently used to assess the ability to perform ADLs, namely mobility and nutrition. Although different scales and techniques exist, we found that there is no one-size-fit-all solution to assess ADLs. Depending on the individual’s conditions and environmental context, researchers and designers may choose one technology or even combine several of them to reach better accuracy. Each of the solutions has their own limitations. Despite the plethora of research in this area, most of the studies were conducted in controlled environment or in short time period. Further investigations are needed, in this promising area of Quality of Life Technologies (QoLT), specifically to assess ADLs.
In this chapter, we also described the development of a conversational agent to promote healthy nutrition for chronically-ill patients. We conducted a qualitative study with 13 patients and health professionals who helped us identify the main barriers as well as the needs and requirements for adopting a healthy nutrition behavior. Lack of regularity, lack of variety, false belief and hunger unawareness were identified as the main barriers to healthy nutrition; whereas monitoring, education, empowerment and practicality were identified as the main needs and requirements for nutrition behavior change. These findings allowed us to suggest the appropriate behavior change techniques to be leveraged in our systems, which are self-monitoring, personalized visual feedback, goal setting, self-awareness and personalized education. Finally, these were translated into a set of functionalities that build up to construct our final solution: MiranaBot. We envision that solutions similar to MiranaBot will be leveraged in the near future to enable easy to use and highly engaging assessment and potential improvement of the Activities of Daily Life and behaviors, leading to better life quality of individuals at all ages.
The QoLT we proposed here falls under the definition given by Wac [88], as a system for assessing or improving the individual’s QoL relying on a hardware and software technology via a visual and an auditory interface. The primary aim of our QoLT here was mainly to assess nutritional habits. However, it also holds the potential to enhance individual’s nutrition. As an extension, QoLT can also potentially be tools using prediction from current behavior to prevent undesired future behavior.
References
World Health Organization. Tracking universal health coverage: first global monitoring report. 2015. ISBN 978 92 4 156497 7.
World Health Organization. 10 facts on ageing and health. 2017. https://www.who.int/features/factfiles/ageing/en/ Accessed 01 June 2020.
Wiles JL, Leibing A, Guberman N, Reeve J, Allen RE. The meaning of “aging in place” to older people. Gerontologist. 2012;52(3):357–66. https://doi.org/10.1093/geront/gnr098.
Bacsu JR, Jeffery B, Johnson S, Martz D, Novik N, Abonyi S. Healthy aging in place: supporting rural seniors’ health needs. Online J Rural Nurs Health Care. 2012;12(2):77–87. https://doi.org/10.14574/ojrnhc.v12i2.52.
Mlinac ME, Feng MC. Assessment of activities of daily living, self-care, and Independence. Arch Clin Neuropsychol. 2016;31(6):506–16. https://doi.org/10.1093/arclin/acw049.
Bravell ME, Zarit SH, Johansson B. Self-reported activities of daily living and performance-based functional ability: a study of congruence among the oldest old. Eur J Ageing. 2011;8(3):199–209. https://doi.org/10.1007/s10433-011-0192-6.
Miller LS, Brown CL, Mitchell MB, Williamson GM. Activities of daily living are associated with older adult cognitive status caregiver versus self-reports. J Appl Gerontol. 2013;32(1):3–30. https://doi.org/10.1177/0733464811405495.
Choe EK, Lee NB, Lee B, Pratt W, Kientz JA. Understanding quantified-selfers’ practices in collecting and exploring personal data. In: Proceedings of the SIGCHI Conference on Human Factors in Computing Systems (CHI ‘14); 2014. p. 1143–52. https://doi.org/10.1145/2556288.2557372.
Wac K. From quantified self to quality of life. In: Rivas H, Wac K, editors. Digital health. Health informatics. Cham: Springer; 2018. https://doi.org/10.1007/978-3-319-61446-5_7.
De Falco I, De Pietro G, Sannino G. Evaluation of artificial intelligence techniques for the classification of different activities of daily living and falls. Neural Comput & Applic. 2020;32:747–58. https://doi.org/10.1007/s00521-018-03973-1.
Katz S. Assessing self-maintenance: activities of daily living, mobility, and instrumental activities of daily living. J Am Geriatr Soc. 1983;31(12):721–7. https://doi.org/10.1111/j.1532-5415.1983.tb03391.x.
Bieńkiewicz MM, Brandi ML, Goldenberg G, Hughes CM, Hermsdörfer J. The tool in the brain: apraxia in ADL. Behavioral and neurological correlates of apraxia in daily living. Front Psychol. 2014;5(353) https://doi.org/10.3389/fpsyg.2014.00353.
Millán-Calenti JC, Tubío J, Pita-Fernández S, González-Abraldes I, Lorenzo T, Fernández-Arruty T, et al. Prevalence of functional disability in activities of daily living (ADL), instrumental activities of daily living (IADL) and associated factors, as predictors of morbidity and mortality. Arch Gerontol Geriatr. 2010;50(3):306–10. https://doi.org/10.1016/j.archger.2009.04.017.
Gaugler JE, Duval S, Anderson KA, Kane RL. Predicting nursing home admission in the US: a meta-analysis. BMC Geriatr. 2007;7(1):13–26. https://doi.org/10.1186/1471-2318-7-13.
Ramos LR, Simoes EJ, Albert MS. Dependence in activities of daily living and cognitive impairment strongly predicted mortality in older urban residents in Brazil: a 2-year follow-up. J Am Geriatr Soc. 2001;49(9):1168–75. https://doi.org/10.1046/j.1532-5415.2001.49233.x.
Webber SC, Porter & M. M, Menec, V.H. Mobility in older adults: a comprehensive framework. The Gerontologist. 2010;50(4):443–50. https://doi.org/10.1093/geront/gnq013.
Patla AE, Shumway-Cook A. Dimensions of mobility: defining the complexity and difficulty associated with community mobility. J Aging Phys Activity. 1999;7(1):7–19. https://doi.org/10.1123/japa.7.1.7.
Tromp AM, Pluijm SMF, Smit JH, Deeg DJH, Bouter LM, Lips P. Fall-risk screening test: a prospective study on predictors for falls in community-dwelling elderly. J Clin Epidemiol. 2001;54(8):837–44. https://doi.org/10.1016/S0895-4356(01)00349-3.
Cederholm T, Barazzoni R, Austin P, Ballmer P, Biolo G, Bischoff SC, et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin Nutr. 2017;36(1):49–64. https://doi.org/10.1016/j.clnu.2016.09.004.
Franz MJ, Bantle JP, Beebe CA, Brunzell JD, Chiasson J-L, Garg A, et al. Evidence-based nutrition principles and recommendations for the treatment and prevention of diabetes and related complications. Diabetes Care. 2002;25(1):148–98. https://10.2337/diacare.25.1.148
Beaudart C, Dawson A, Shaw SC, et al. Nutrition and physical activity in the prevention and treatment of sarcopenia: systematic review. Osteoporos Int. 2017;28:1817–33. https://doi.org/10.1007/s00198-017-3980-9.
Lindqvist C, Slinde F, Majeed A, Bottai M, Wahlin S. Nutrition impact symptoms are related to malnutrition and quality of life–a cross-sectional study of patients with chronic liver disease. Clin Nutr. 2020;39(6):1840–8. https://doi.org/10.1016/j.clnu.2019.07.024.
Jekel K, Damian M, Wattmo C, et al. Mild cognitive impairment and deficits in instrumental activities of daily living: a systematic review. Alz Res Therapy. 2015;7:17. https://doi.org/10.1186/s13195-015-0099-0.
Desai AK, Grossberg GT, Sheth DN. Activities of daily living in patients with dementia: clinical relevance, methods of assessment and effects of treatment. CNS Drugs. 2004;18(13):853–75. https://doi.org/10.2165/00023210-200418130-00003.
Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged: the index of ADL: a standardized measure of biological and psychosocial function. JAMA. 1963;185(12):914–9. https://doi.org/10.1001/jama.1963.03060120024016.
George & Fillenbaum. Validity and reliability of OARS multidimensional functional assessment questionnaire in Iranian elderly. Iran Rehabil J. 1985;16 https://doi.org/10.32598/irj.16.2.169.
Ferrucci L, Koh C, Bandinelli S, Guralnik JM. Disability, functional status, and activities of daily living. In: Encyclopedia of gerontology (Second Edition). Elsevier; 2007. p. 427–36. https://doi.org/10.1016/B0-12-370870-2/00075-5.
Roedl J, Wilson LS, Fine J. A systematic review and comparison of functional assessments of community-dwelling elderly patients. J Am Assoc Nurse Pract. 2016;28(3):160–9. https://doi.org/10.1002/2327-6924.12273.
Adachi T. Advantages and disadvantages of the functional Independence measure for home care. In: Chino N, Melvin JL, editors. Functional evaluation of stroke patients. Tokyo: Springer; 1996. https://doi.org/10.1007/978-4-431-68461-9_10.
Grey N, Kennedy P. The functional Independence measure: a comparative study of clinician and self ratings. Paraplegia. 1993;31(7):457–61. https://doi.org/10.1038/sc.1993.74.
Mainetti L, Patrono L, Sergi I. A survey on indoor positioning systems. In: 22nd International Conference on Software, Telecommunications and Computer Networks (SoftCOM); 2014. p. 111–20. https://doi.org/10.1109/SOFTCOM.2014.7039067.
Heinz EA, Kunze KS, Gruber M, Bannach D. Using wearable sensors for real time recognition tasks in games of martial arts–an initial experiment. In: In Proceedings of the IEEE Symposium on Computational Intelligence and Games; 2006. p. 98–102. https://doi.org/10.1109/CIG.2006.311687.
Wang LK. Recognition of human activities using continuous autoencoders with wearable sensors. Sensors. 2016;16:189. https://doi.org/10.3390/s16020189.
Ayase R, Higashi T, Takayama S, Sagawa S, Ashida N. A method for supporting at-home fitness exercise guidance and at-home nursing Care for the Elders, video-based simple measurement system. In: In Proceedings of IEEE 10th International Conference on e-health Networking, Applications and Services (HealthCom); 2008. p. 182–6. https://doi.org/10.1109/HEALTH.2008.4600133.
Goffredo M, Schmid M, Conforto S, Carli M, Neri A, D’Alessio T. Markerless human motion analysis in gauss-Laguerre transform domain: an application to sit-to-stand in young and elderly people. IEEE Trans Inf Technol Biomed. 2009;13:207–16. https://doi.org/10.1109/TITB.2008.2007960.
Li Y, Miaou S, Hung CK, Sese JT. A gait analysis system using two cameras with orthogonal view. In: Proceedings of IEEE International Conference on Multimedia Technology (ICMT); 2011. p. 2841–4. https://doi.org/10.1109/ICMT.2011.6002046.
Mautz R, Tilch S. Survey of optical indoor positioning systems. In: International Conference Indoor Positioning Indoor Navigation (IPIN); 2011. p. 1–7. https://doi.org/10.1109/IPIN.2011.6071925.
Ausmeier B, Campbell T, Berman S. Indoor navigation using a Mobile phone. In: African Conf. Sofware Engineering and Applied Computing (ACSEAC); 2012. p. 109–15. https://doi.org/10.1109/ACSEAC.2012.26.
Elloumi W, et al. Indoor navigation assistance with a smartphone camera based on vanishing points. In: International Conference Indoor Positioning and Indoor Navigation (IPIN); 2013. p. 1–9. https://doi.org/10.1109/IPIN.2013.6817911.
Kahlert D, Ehrhardt N. Out-of-home mobility and social participation of older people: a photo-based ambulatory assessment study. Population Ageing. 2020; https://doi.org/10.1007/s12062-020-09278-3.
Addlesee MD, Jones A, Livesey F, Samaria F. The ORL active floor [sensor system]. IEEE Pers Commun. 1997;4(5):35–41. https://doi.org/10.1109/98.626980.
Schmidt A, Strohbach M, van Laerhoven K, Friday A, Gellersen HW. Context acquisition based on load sensing. In: Borriello G, Holmquist LE, editors. UbiComp 2002: ubiquitous computing. Lecture notes in computer science, vol. 2498; 2002. https://doi.org/10.1007/3-540-45809-3_26.
Middleton L, Buss AA, Bazin A, Nixon MS. A floor sensor system for gait recognition. In: Proceedings of the fourth IEEE workshop on automatic identification advanced technologies (AUTOID ‘05). IEEE Computer Society; 2005. p. 171–6. https://doi.org/10.1109/AUTOID.2005.2.
Paradiso J, Abler C, Hsiao K, Reynolds M. The magic carpet: physical sensing for immersive environments. In: CHI '97 extended abstracts on human factors in computing systems; 1997. https://doi.org/10.1145/1120212.1120391.
Richardson B, Leydon K, Fernström M, Paradiso J. Z-tiles: building blocks for modular, pressure-sensing floorspaces. Proceedings of CHI. 2004;1529-1532 https://doi.org/10.1145/985921.986107.
Merilampi, S., Mulholland, K., Ihanakangas, V., Ojala, J., Valo P. & Virkki, J. (2019). A smart chair physiotherapy Exergame for fall prevention–user experience study. IEEE 7th International Conference on Serious Games and Applications for Health (SeGAH), pp. 1–5, doi:https://doi.org/10.1109/SeGAH.2019.8882482.
Allet L, Knols RH, Shirato K, Bruin ED. Wearable Systems for Monitoring Mobility-Related Activities in chronic disease: a systematic review. Sensors. 2010;2010(10):9026–52. https://doi.org/10.3390/s101009026.
De Bruin ED, Hartmann A, Uebelhart D, Murer K, Zijlstra W. Wearable systems for monitoring mobility-related activities in older people: a systematic review. Clin Rehabil. 2008;22(10–11):878–95. https://doi.org/10.1177/0269215508090675.
Yang C-C, Hsu Y-L. A review of Accelerometry-based wearable motion detectors for physical activity monitoring. Sensors. 2010;2010(10):7772–88. https://doi.org/10.3390/s100807772.
Berglind D, Yacaman-Mendez D, Lavebratt C, Forsell Y. The effect of smartphone apps versus supervised exercise on physical activity, cardiorespiratory fitness, and body composition among individuals with mild-to-moderate mobility disability: randomized controlled trial. JMIR Mhealth Uhealth. 2020;8(2):e14615. https://doi.org/10.2196/14615.
Fillekes MP, Kim EK, Trumpf R, Zijlstra W, Giannouli E, Weibel R. Assessing older adults’ daily mobility: a comparison of GPS-derived and self-reported mobility indicators. Sensors (Basel, Switzerland). 2019;19(20):4551. https://doi.org/10.3390/s19204551.
Elgala H, Mesleh R, Haas H. Indoor optical wireless communication: potential and state-of-the-art. IEEE Commun Mag. 2011;49(9):56–62. https://doi.org/10.1109/MCOM.2011.6011734.
Medina C, Segura JC, De la Torre Á. Ultrasound indoor positioning system based on a low-power wireless sensor network providing sub-centimeter accuracy. Sensors. 2013;2013(13):3501–26. https://doi.org/10.3390/s130303501.
Chen L, Wu E, Chen G. Intelligent fusion of Wi-fi and inertial sensor-based positioning Systems for Indoor Pedestrian Navigation. IEEE Sensors J. 2014;no. 99 https://doi.org/10.1109/JSEN.2014.2330573.
Faragher R, Harle R. Location fingerprinting with Bluetooth low energy beacons. IEEE Journal on Selected Areas in Communications. 2015;33(11):2418–28. https://doi.org/10.1109/JSAC.2015.2430281.
Di Giampaolo E. A passive-RFID based indoor navigation system for visually impaired people. In: 3rd International Symposium on Applied Sciences in Biomedical and Communication Technologies (ISABEL 2010); 2010. p. 1–5. https://doi.org/10.1109/ISABEL.2010.5702800.
Zeng L. A survey: outdoor mobility experiences by the visually impaired. In: Weisbecker A, Burmester M, Schmidt A, editors. Mensch und Computer 2015; 2015. p. S. 391–7.
Allahbakhshi H, Conrow L, Naimi B, Weibel R. Using accelerometer and GPS data for real-life physical activity type detection. Sensors. 2020;2020(20):588. https://doi.org/10.3390/s20030588.
Webber SC, Porter MM. Monitoring mobility in older adults using global positioning system (GPS) watches and accelerometers: a feasibility study. J Aging Phys Act. 2009;17(4):455–67. https://doi.org/10.1123/japa.17.4.455.
Ghali A, Cunningham AS, Pridmore TP. Object and event recognition for stroke rehabilitation. In: In Proceedings of Visual Communications and Image processing; 2003. p. 980–9. https://doi.org/10.1117/12.503470.
Lo FP, Sun Y, Qiu J, Lo BPL. Point2Volume: a vision-based dietary assessment approach using view synthesis. IEEE Transactions on Industrial Informatics. 2020;16(1):577–86. https://doi.org/10.1109/TII.2019.2942831.
Pettitt C, Liu J, Kwasnicki R, Yang G, Preston T, Frost G. A pilot study to determine whether using a lightweight, wearable micro-camera improves dietary assessment accuracy and offers information on macronutrients and eating rate. Br J Nutr. 2016;115(1):160–7. https://doi.org/10.1017/S0007114515004262.
Gemming L, Doherty A, Utter J, Shields E, Mhurchu CN. The use of a wearable camera to capture and categorise the environmental and social context of self-identified eating episodes. Appetite. 2015;92:118–25. https://doi.org/10.1016/j.appet.2015.05.019.
Zhou B, et al. Smart table surface: a novel approach to pervasive dining monitoring. In: 2015 IEEE International Conference on Pervasive Computing and communications (PerCom); 2015. p. 155–62. https://doi.org/10.1109/PERCOM.2015.7146522.
Hermsen S, Frost JH, Robinson E, Higgs S, Mars M, Hermans RCJ. Evaluation of a smart fork to decelerate eating rate. J Acad Nutr Diet. 2016; https://doi.org/10.1016/j.jand.2015.11.004.
Huang Q, Yang Z, Zhang Q. Smart-U: smart utensils know what you eat. In: IEEE INFOCOM 2018–IEEE Conference on Computer Communications; 2018. p. 1439–47. https://doi.org/10.1109/INFOCOM.2018.8486266.
Mertes G, Christiaensen G, Hallez H, Verslype S, Chen W, Vanrumste B. Measuring weight and location of individual bites using a sensor augmented smart plate. In: 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC); 2018. p. 5558–61. https://doi.org/10.1109/EMBC.2018.8513547.
Burke R, Felfernig A, Göker MH. Recommender systems: an overview. AI Mag. 2011;32(3):13–8. https://doi.org/10.1609/aimag.v32i3.2361.
Shah K, Salunke A, Dongare S, Antala K. Recommender systems: an overview of different approaches to recommendations. In: International Conference on Innovations in Information, Embedded and Communication Systems (ICIIECS); 2017. p. 1–4. https://doi.org/10.1109/ICIIECS.2017.8276172.
Mika S. Challenges for nutrition recommender systems. In: Proceedings of the 2nd Workshop on Context Awareness in Retrieval and recommendation; 2011. p. 786.
Tran TN, Atas M, Felfernig A, Stettinger M. An overview of recommender systems in the healthy food domain. J Intell Inf Syst. 2017;50:501–26. https://doi.org/10.1007/s10844-017-0469-0.
Konstan JA, Riedl J. Recommender systems: from algorithms to user experience. User Model User-Adap Inter. 2012;22(1–2):101–23. https://doi.org/10.1007/s11257-011-9112-x.
Korpusik M, Glass J. Spoken language understanding for a nutrition dialogue system. IEEE Trans Audio Speech Lang Process. 2017;25:1450–61. https://doi.org/10.1109/TASLP.2017.2694699.
Casas J, Mugellini E, Khaled OA. Food diary coaching Chatbot. In: In Proceedings of the 2018 ACM International Joint Conference and 2018 International Symposium on Pervasive and Ubiquitous Computing and Wearable Computers (UbiComp '18); 2018. p. 1676–80. https://doi.org/10.1145/3267305.3274191.
Meso P, Jain R. Agile software development: adaptive systems principles and best practices. Inf Syst Manag. 2006;23(3):19–30. https://doi.org/10.1201/1078.10580530/46108.23.3.20060601/93704.3.
Duff O, Walsh D, Furlong B, O’Connor N, Moran K, Woods C. Behavior change techniques in physical activity eHealth interventions for people with cardiovascular disease: systematic review. J Med Internet Res. 2017;19(8):e281. https://doi.org/10.2196/jmir.7782.
Schembre S, Liao Y, Robertson M, Dunton G, Kerr J, Haffey M, et al. Just-in-time feedback in diet and physical activity interventions: systematic review and practical design framework. J Med Internet Res. 2018;20(3):e106. https://doi.org/10.2196/jmir.8701.
Sawesi S, Rashrash M, Phalakornkule K, Carpenter JS, Jones JF. The impact of information technology on patient engagement and health behavior change: a systematic review of the literature. JMIR Med Inform. 2016;4(1):e1. https://doi.org/10.2196/medinform.4514.
Greaves CJ, Sheppard KE, Abraham C, Hardemann W, Rode M, Evans PH, et al. Systematic review of reviews of intervention components associated with increased effectiveness in dietary and physical activity interventions. BMC Public Health. 2011;11:119. https://doi.org/10.1186/1471-2458-11-119.
Michie S, Abraham C, Whittington C, McAteer J, Gupta S. Effective techniques in healthy eating and physical activity interventions: a meta-regression. Health Psychol. 2009;28(6):690–701. https://doi.org/10.1037/a0016136.
Lara J, Evans EH, O'Brien N, Moynihan PJ, Meyer TD, Adamson AJ, et al. Association of behaviour change techniques with effectiveness of dietary interventions among adults of retirement age: a systematic review and meta-analysis of randomised controlled trials. BMC Med. 2014;12:177. https://doi.org/10.1186/s12916-014-0177-3.
Prochaska J, Velicer W. The Transtheoretical model of health behavior change. Am J Health Promot. 1997;12:38–48. https://doi.org/10.4278/0890-1171-12.1.38.
Klein M, Mogles N, van Wissen A. Why Won’t you do What’s good for you? Using intelligent support for behavior change. In: Salah AA, Lepri B, editors. Human behavior understanding. HBU 2011. Lecture notes in computer science, vol. 7065; 2011. https://doi.org/10.1007/978-3-642-25446-8_12.
Karoly P. Mechanisms of self-regulation: a systems view. Annu Rev Psychol. 1993;44(1):23–52. https://doi.org/10.1146/annurev.psych.44.1.23.
Swiss Society of Nutrition. Balanced Diet-Optimum Plate. http://www.sge-ssn.ch/fr/toi-et-moi/boire-et-manger/equilibre-alimentaire/assiette-optimale/. Accessed on 01 June 2020.
Cohen D, Farley TA. Eating as an automatic behavior. Prev Chronic Dis. 2008;5(1):A23.
Yau YH, Potenza MN. Stress and eating behaviors. Minerva Endocrinol. 2013;38(3):255–67.
Wac K. Quality of life technologies. In: Gellman M, editor. Encyclopedia of behavioral medicine. New York, NY: Springer; 2020. https://doi.org/10.1007/978-1-4614-6439-6_102013-1.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2022 The Author(s)
About this chapter

Cite this chapter
Randriambelonoro, M. (2022). Assessing Activity of Daily Living through Technology-Enabled Tools: Mobility and Nutrition Assessment: MiranaBot: A Nutrition Assessment Use Case. In: Wac, K., Wulfovich, S. (eds) Quantifying Quality of Life. Health Informatics. Springer, Cham. https://doi.org/10.1007/978-3-030-94212-0_2
Download citation
DOI: https://doi.org/10.1007/978-3-030-94212-0_2
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-94211-3
Online ISBN: 978-3-030-94212-0
eBook Packages: MedicineMedicine (R0)