
Abstract
The design of medical devices is challenging, due to strict geometry specifications and criteria belonging to several disciplines. The aim of this paper is to provide a design methodology which seems to lack in the literature of design of biomedical devices. In particular, the case study proposed in this paper concerns with the design of Bone-Biopsy (BB) needle devices. Following the design process of Pahl and Beitz, a functional analysis is carried out, to point out the interfaces between parts of existing BB needles. A morphology matrix is used to generate alternatives for the cannula holder, the core part of the product. Generated alternatives have been ranked and scored by means of the Pugh’s Controlled Convergence method according to the decision makers' opinions. In this work, the design peculiarities related to the BB needles which have been pointed out could be extended for guiding the design of other biomedical devices.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others


Keywords
- Bone-Biopsy needle
- Multicriteria decision making
- Design of biomedical devices
- Conceptual design
- Pugh’s Controlled Convergence
1 Introduction
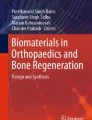
The design of bone biopsy needles is challenging, due to several criteria which need to be considered concurrently, as well as strict geometry specifications requested. Hence, design methods should be adopted in order to satisfy constraints and select most suitable alternatives, considering all the multiple criteria and actors involved. The case study of this paper concerns the design of bone biopsy (BB) needle devices. Bone biopsy is a diagnostic procedure consisting in taking a sample of bone tissue to be analysed in the laboratory, by means of a device with a hollow cannula surrounding a stylet (Fig. 1). The cannula and stylet are coaxially assembled and are used to penetrate through the outer layer of the bone, (cortex), which is harder than the trabecular bone layer and the marrow. Reliable devices are characterized by optimized shapes of the handle, needle and cannula.

Bone-Biopsy needles (Jamshidi type) and relative components
In the literature, papers related to the design of biopsy needles are mostly aimed at enhancing the biopsy efficiency in relation to the geometry of the cannula and needle. This is for enhancing the sample geometry [1,2,3], or the efficiency in taking it from the bone [4,5,6]. More in general, the use of MCDM methods in the design of medical devices has been proposed in the literature, as in [7,8,9]. At the authors’ best knowledge, no works regard the application of design methods for generating and selecting new conceptual designs. Hence, this work is aimed at describing the requirements related to the design of bone biopsy needles, as well as the steps required for the generation and selection of concepts. This is to enhance the state of the art on the design of medical devices, and guide designers in the assessment of design of novel medical devices, by providing a design methodology which seems to lack in the design of biomedical devices.
2 Method
The engineering design process adopted for the generation and selection of biomedical devices is based on the systematic approach proposed by Pahl and Beitz [10]. In Fig. 2, the method followed is schematically depicted. Product specifications are identified within the involved disciplines, (medicine, engineering design, and manufacturing). In the planning phase, a functional analysis is carried out, to identify interfaces between product parts, and analyze them in terms of response to product requirements. To this aim, a benchmark of the existing needles has been performed first, in order to find out the common features among the existing BB-needles. Hence, a functional analysis is carried out, for evaluating the core components of the needle assembly. Related concept designs are generated considering the functions performed by each part of the device. The parts have been collected within a morphology table, screened and scored by means of the Pugh’s Controlled Convergence (PuCC) method, which is included in multicriteria decision making (MCDM) methods as described in [11]. PuCC method is used to classify and rank design alternatives candidate solutions, considering the judgments of the decision makers belonging to different technical backgrounds.

Design process for a biomedical device
3 Results
The functional analysis of the BB-needle is schematically reported in (Fig. 3). The handle 1 is made of components A1 (cap) and B1 (handle body) and is the interface with the operator. In the handle, the interface between parts A1 and B1 requires for a reliable tightening and ease of connection. Existing devices use locks as the bayonet lock, snap fits, and cam-clamping. The interface between B1 and 2 is fundamental, as the central body is used to couple handle and cannula. The “2-to-3” interface regards the connection of the cannula in the central body. The “3-to-4” interface between the cannula and the needle requires strict coaxial tolerances, hence the dimensions of these parts are constrained by regulations. The “5-to-patient” interface is fundamental as it limits the depth penetration of the needle. The height is regulated by means of a thread (“5 to 2” interface), to guarantee the sliding of the regulator. The interface between B1 and the cannula 3 is the cannula holder 6, which is the core of the product, as it holds the cannula 3 during its penetration into the bone. This is also responsible for the stresses and forces on the operator and patient during biopsy operations. Hence, the generation and selection of novel design are dedicated to the cannula holder component 6. Functions related to the cannula holder are connection with the syringe (6-1), connection with the handle body (6-2), and connection with the depth regulator 5 (6-3). Conceptual designs for the cannula holder are generated by means of a morphology table, taking into account the interfaces with the coupled components as in the functional analysis (Fig. 4).

Functional scheme of a bone biopsy needle (1 – Handle. (cover A1 – body B1); 2 – central body; 3 – cannula; 4 – needle (stylet); 5 – depth regulator (guard), 6 – cannula holder: functions 6-1, 6-2, 6-3).
In particular: the connection with a syringe is via a Luer Lock thread (1A) or one contour thread (1B). The tightening on the handle is carried out by means of snap fits of different geometries (2A, 2B and 2C, Fig. 4). The lower side clamping with the regulator (3A, 3B and 3C in Fig. 4) is based on snap-fits. To avoid pairwise comparing and analyzing all 18 generated combinations, a modified PuCC method is used. In particular, concepts are screened according to the functions covered, namely function 1: connection to the syringe (concepts 1A, 1B); function 2: connection to the handle body (concepts 2A, 2B, 2C); function 3: connection to the depth regulator (concepts 3A, 3B, 3C). Concept designs are screened by means of the PuCC method, (Table 1) according to four criteria, namely: ease of manufacturing, easy geometry (presence of undercuts), easy connection with the coupled component, reliable connection with the coupled component. The reference product is the component 6 of Fig. 3. The judgments given to the alternatives in the PuCC matrix derive from a former discussion among the decision makers, namely the designer, the manufacturer, the surgeon and the business manager of a SME in the northern of Italy, which is specialized in biopsy needles. They provided judgments for each design alternative, depending on the specific function (1, 2, 3) and criterion that each part of the device must perform. According to the PuCC method, the most suitable combination for the cannula holder geometry seems to be the 1B-2C-3C Fig. 5. Unlike the AHP method, the PuCC method does not involve analytic calculations for ranking the alternatives. Nevertheless, it maintains the objectivity of the judgments by means of a discussion among the decision makers [11].

Morphologic table for the inner connection device

The selected design for the cannula holder (left) and the layout of the entire Bone biopsy needle (right).
4 Discussion and Conclusions
The conceptual design of medical devices is challenging, due to strict regulations and criteria to be satisfied. In this paper, the systematic method of Pahl and Beitz [10] is used for the functional analysis of the components in the assembly. Hence a modified PuCC method [11] is adopted for screening and scoring the alternatives for the cannula holder in a BB-needle. The proposed cannula holder seems to provide a better connection to the coupled components, with respect to existing products. This work is aimed at enhancing the state of the art on the design of medical devices, guiding designers in the design of novel medical devices.
References
Keulers, A., Cunha-Cruz, V.C., Bruners, P., Penzkofer, T., Braunschweig, T., Schmitz-Rode, T., Mahnken, A.: Bone biopsy needles: mehanical properties, needle design and specimen quality [Knochen-biopsiesysteme: Mechanische eigenschaften, nadeldesign und probenqualität]. RoFo Fortschritte auf dem Gebiet der Rontgenstrahlen und der Bildgebenden Verfahren 183(3), 274–281 (2011)
Misiewicz, J., Nguyen, B., Poudyal, A., Wachrathit, K., Chen, Y., Vossoughi, J.: A fiber optic enhanced bone biopsy needle. In: 2012 38th Annual Northeast Bioengineering Conference, NEBEC 2012, pp. 382–383. (2012) Art. no. 6207124
Giovannini, M., Ren, H., Cao, J., Ehmann, K.: Study on design and cutting parameters of rotating needles for core biopsy. J. Mech. Behav. Biomed. Mater. 86, 43–54 (2018)
Roberts, C.C., Morrison, W.B., Leslie, K.O., Carrino, J.A., Lozevski, J.L., Liu, P.T.: Assessment of bone biopsy needles for sample size, specimen quality and ease of use. Skeletal Radiol. 34(6), 329–335 (2005)
Uhl, M., Theves, C., Geiger, J., Kersten, A., Strohm, P.C.: The percutaneous bone biopsy: in vitro study for comparison of bone biopsy needles [Die perkutane Knochenbiopsie: Experimentelle Studie zum Vergleich von Knochenbiopsiesystemen]. Zeitschrift für Orthopädie und Unfallchirurgie 147(3), 327–333 (2009)
Islam, A.: Bone marrow solid core biopsy needle: a critical assessment of the utility, benefits and limitations of the instruments employed in current day haematology and oncology. J. Clin. Pathol. 71(6), 475–482 (2018)
Aitchison, G.A., Hukins, D.W.L., Parry, J.J., Shepherd, D.E.T., Trotman, S.G.: A review of the design process for implantable orthopedic medical devices. Open Biomed. Eng. J. 3, 21 (2009)
Ivlev, I., Vacek, J., Kneppo, P.: Multi-criteria decision analysis for supporting the selection of medical devices under uncertainty. Eur. J. Oper. Res. 247(1), 216–228 (2015)
Rogalewicz, V., Jurickova, I.: Multiple-criteria decision making: application to medical devices. In: IWBBIO. pp. 1359–1372 (2014)
Pahl, G., Beitz, W.: Engineering Design: A Systematic Approach, 2nd edn. Springer, London (1996)
Renzi, C., Leali, F., Pellicciari, M., Andrisano, A.O., Berselli, G.: Selecting alternatives in the conceptual design phase: an application of Fuzzy-AHP and Pugh’s Controlled Convergence. Int. J. Interact. Des. Manuf. 9(1), 1–17 (2013)
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2021 The Author(s)
About this paper

Cite this paper
Renzi, C., Leali, F. (2021). Multicriteria Decision Making Methods in Engineering Design: An Application on Medical Devices. In: Roucoules, L., Paredes, M., Eynard, B., Morer Camo, P., Rizzi, C. (eds) Advances on Mechanics, Design Engineering and Manufacturing III. JCM 2020. Lecture Notes in Mechanical Engineering. Springer, Cham. https://doi.org/10.1007/978-3-030-70566-4_64
Download citation
DOI: https://doi.org/10.1007/978-3-030-70566-4_64
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-70565-7
Online ISBN: 978-3-030-70566-4
eBook Packages: EngineeringEngineering (R0)