
Abstract
Photovoice, as a Community-Based Participatory Action Research (CBPAR) approach, aims to combine research with advocacy and action for achieving change. This project aimed to use photovoice to assess and increase awareness on public health problems faced by young refugees in Turkey, as well as involve young people in health promotion research and have their voices heard by policy makers. The qualitative study was conducted with young people experiencing forced migration and with local youth aged 18 to 30 years in Turkey. The methodology involved representing problems through photographs taken by participants and conducting discussions among both refugee and local youth groups, followed by dissemination and advocacy activities such as producing publications and organizing photo exhibitions that brought together policy makers, health service providers, civil society organizations, refugees, and host communities to achieve positive change through joint action. Through the photovoice process, we found that although health care services were widely available for registered refugees, many faced language, financial, cultural, and educational barriers—as well as gender and stigma-related barriers—to accessing health information, health services, and healthy environments. Using photovoice, as a CBPAR approach, had numerous advantages, such as the creation of visual findings that were more impactful than written material, the opportunity to work with vulnerable/disadvantaged groups throughout the research process, and increasing interaction between different stakeholders. This chapter demonstrates how photovoice can be used as a tool for research and advocacy to promote health and decrease inequalities in forced migration settings.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Forced migration is one of the most significant consequences of man-made and natural disasters throughout history. Today, millions of people are forced from their homes by war, persecution, and poverty, driving a global migration crisis (UN 2018). Factors such as poverty, unhealthy living conditions, and lack of nutritious food—in addition to poor access to health care, social care, education, and employment opportunities—cause forced migrants (e.g., refugees and asylum seekers) to be among the most vulnerable groups with respect to health (Karadag Caman and Altintas 2010).
The United Nations Convention Relating to the Status of Refugees (1951) defines a refugee as “a person who owing to a well-founded fear of being persecuted for reasons of race, religion, nationality, membership of a particular social group or political opinion, is outside the country of his nationality and is unable or, owing to such fear, is unwilling to avail himself of the protection of that country; or who, not having a nationality and being outside the country of his former habitual residence as a result of such events, is unable or, owing to such fear, is unwilling to return to it” (UNHCR 1951). The United Nations High Commission for Refugees (UNHCR) has called the Syrian emergency “the biggest humanitarian and refugee crisis of our time.” Since the start of the conflict in Syria, an estimated 6.6 million persons have been displaced inside the country and an additional 5.6 million persons have fled to other countries. More than 90% of people fleeing Syria have sought asylum in three countries: Turkey, Lebanon, and Jordan (UNHCR 2019). According to the World Migration Report (2018) of the International Organization for Migration (IOM), Turkey has the highest number of refugees in the world (3.6 million), with the majority being Syrian. Latest national statistics indicate that over 95% of the refugees live in urban areas, and young people constitute the majority of the refugee population in Turkey, where more than 70% of the refugees are below 30 years old (Turkish Ministry of Interior 2019).
Young refugees are among the most vulnerable population groups with respect to physical, mental, and social health problems; sexual and gender-based violence; trafficking; and early and forced marriage (Karadag Caman and Bahar Ozvaris 2010; Women’s Refugee Commission 2016). Refugee youth also face numerous challenges including barriers to accessing quality learning, education, and employment opportunities, as well as youth-friendly health care and social care (Norwegian Refugee Council 2018; UNHCR 2017). In Turkey, although health care is freely available for registered refugees, use of health services—especially the uptake of preventive services—remains low due to factors such as health literacy problems, lack of awareness about available services, language problems, and cultural barriers including gender inequalities (Karadag Caman 2015; Kaya and Kiraç 2016). However, little research to date has examined how to bridge this gap. Qualitative research may be useful in this regard, as it is known to be effective in learning more about different values, perspectives, attitudes, behaviors, and social contexts of specific population groups. Using qualitative methods can sometimes be more helpful than quantitative research when working with vulnerable and/or disadvantaged groups because these methods encourage learning about a given phenomenon from individuals themselves, rather than driven solely by researchers’ framing of the issue. As a result, qualitative research can help both researchers and policy makers to better understand the complex reality of a given context and can also complement quantitative research (Mack et al. 2005). One qualitative approach is Community-Based Participatory Action Research (CBPAR), which has been recognized as a unique approach to conducting research with—rather than on—communities. CBPAR involves researchers, community members, and decision makers and aims to combine research with advocacy and action for achieving change (Holkup et al. 2004). CBPAR differs from traditional research in many ways. Instead of creating knowledge for the advancement of a field or for knowledge’s sake, CBPAR is an iterative process, integrating research, reflection, and action in a cyclical process (Holkup et al. 2004).
In the early 1990s, Dr. Caroline Wang, a professor and researcher with the University of Michigan, developed photovoice, a creative approach to participatory action research. According to Wang, photovoice has three main goals: (1) to enable people to record and reflect their community’s strengths and concerns, (2) to promote critical dialogue and knowledge about important issues through group discussion of photographs, and (3) to reach decision makers to change policies and programs (Wang and Burris 1997). Among CBPAR methods, photovoice is designed to empower members of vulnerable or disadvantaged groups by giving them an opportunity to tell their own stories and have their voices heard (Budig et al. (2018). Photovoice enables researchers, community members, and policy/decision makers to work in a collaborative manner to achieve social change through photography. By documenting their own worlds and critically discussing with policy makers the images they produce, communities can initiate social change (Wang et al. 2004). Using cameras, participants may focus on a wide range of individual, family, and community assets and needs. By sharing and talking about their photographs, participants may also use the power of visual images to communicate their life experiences, expertise, and knowledge (Wang et al. 1998). Therefore, photovoice can be used more widely in health promotion research, especially among more vulnerable/disadvantaged groups such as refugees and youth, as an empowerment and advocacy tool and as a social bridge. Within this framework, the project described in this chapter aimed to involve young people in health promotion research and advocacy through the use of photovoice to assess and increase awareness on the most pressing public health problems they faced.
2 The Photovoice Process
2.1 Setting
The present study was conducted with young refugee and local youth aged 18 to 30 years in Hatay, which is one of the provinces with the highest per capita concentration of refugees in Turkey. The study was conducted as part of a larger project between December 2015 and April 2016 with the collaboration of a national NGO (Community Volunteers Foundation), United Nations Population Fund (UNFPA) Country Office, and Hacettepe University in Turkey.
Photovoice was selected as part of a mixed-methods study to complement quantitative data collection in the field. The quantitative needs assessment study was conducted with 251 young refugees (aged 18–30 years). The quantitative data collection aimed to assess the current situation of young refugees in order to plan evidence-based interventions with respect to health, education, employment, and gender issues. The main motivation to complement this quantitative survey with a photovoice approach was to select a research method that enables active participation of young refugees in identifying their own problems and finding solutions, as well as to increase social cohesion and mutual understanding between refugee and local youth. Creation of visual materials that could attract more attention of stakeholders than written materials was another strong motive in choosing this specific photography-based approach.
2.2 Participants
Young people experiencing forced migration were recruited during the quantitative survey portion of the larger project in Hatay, in which the survey participants were asked about their willingness to participate in another study that used photography and group discussions. After the quantitative data collection was completed, the young people who had volunteered to take part in the photovoice study were contacted via e-mail or mobile phone and were invited to an introductory meeting with the research team (principal investigator, OC, and two local facilitators). In addition, local youth within the same age group were contacted by local NGOs using snowball sampling and were invited to take part in the same study. The study was conducted with a group of 12 young people (nine refugee and three local youth) who gathered in meetings before, during, and after data collection in the field. The country of origin for refugee youth was Syria and they had “temporary protection status,” which is a legal status giving forced migrants access to certain services and employment opportunities in Turkey. The main goals in bringing together refugee and local youth were to increase interaction and to improve mutual understanding between the two groups of young people, who were living in the same urban area in physical terms but in mostly different environments in social terms.
2.3 Study Timeline and Steps
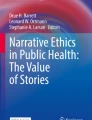
Taking into consideration the proposed stages of photovoice by Dr. Wang et al. (1998), the following study steps were taken as shown in Fig. 10.1.

Photovoice study steps of the present project. (Reproduced with permission from the author. Copyright © 2021 Ozge Karadag Caman. All rights reserved)
The methodology involved an introductory half-day meeting with the participants to: (1) introduce the photovoice approach with its participatory nature; (2) discuss, get input, and agree on the overall aim of the study; (3) receive written informed consent of participants; (4) introduce specific features of the distributed cameras; (5) discuss data collection procedures; and (6) discuss ethical issues regarding taking photos in the field.
This first meeting lasted around three and a half hours in total (two sessions with a half-hour coffee break in between). The meeting was mainly led by two local and bilingual facilitators, who were trained by the principal investigator on the study methodology. The local facilitators were members of local NGOs and were leading several other projects in the study area. Therefore, they were already knowledgeable about the local context and had previous contact with some of the study participants, which made it easier for young people to participate and devote time to this photovoice project on a voluntary basis. After the introduction to the project, there was a general discussion about the major individual and environmental health concerns for young refugees, as well as the potential barriers that they may face in accessing health care. Thereafter, the main aim of the study was discussed and agreed upon with the participants—namely, that the study should aim to reflect the main challenges that young refugees face with respect to healthy living conditions and access to health care services in Turkey. The facilitators delivered information about the photo-taking process, including important features of the distributed digital cameras and how and where to use the cameras. During this time, several ethical issues were also discussed in the group, such as the importance of getting permission when taking photos of other people and the rules for taking photos of minors. Finally, potential participants provided written consent to participate, and the group agreed to meet in the same place two weeks later.
The first part of the data collection process lasted two weeks and involved reflection of refugees’ individual- and environmental-level health issues/problems through photographs taken by both refugee and local youth. After the two-week data collection period was over, all participants were invited to meet again for a general group discussion and reflection on their experience in this photovoice study.
The second meeting with the same participants was a two-hour focus group meeting in which all photographs taken by the participants were discussed. This group meeting was led by the principal investigator and included one facilitator helping in Arabic-Turkish translation and facilitating discussion while the other facilitator took written notes about the discussion. The discussion was guided by the following series of questions adapted from the SHOWeD guide (Wang 1999):
General discussion with the group:
-
1.
In your opinion, what kind of factors affect the health of young people experiencing forced migration?
-
2.
In your opinion, what kind of barriers do young people experiencing forced migration face when trying to access health care services in Turkey?
Individual reflections for each photo taken:
-
3.
What would you like to share with the group about this photo?
-
4.
What was the main reason why you took this photo?
-
5.
What kind of barriers does this photo show regarding young people’s health promotion and/or accessing health care?
-
6.
Do you have any recommendations to solve this problem or to overcome this barrier?
General discussion with the group:
-
7.
Do you have any other opinions or recommendation to promote the health of young people experiencing forced migration?
-
8.
How can young people’s access to health services be improved?
Upon participants’ request to continue taking photos for two more weeks, the same cycle of data collection and group discussion was repeated once more. All group discussions were voice-recorded (after obtaining written consent of participants) and were then transcribed and translated verbatim. The qualitative data from the study were analyzed using thematic content analysis. The initial analysis was performed by the principal investigator with input from the two facilitators; the initial set of themes were shared with youth for their feedback, which was incorporated in an iterative process continuously throughout project discussions.
3 Project Findings and Impact
The photos and the group discussions about those photos demonstrated that although health care services in the public sector were widely available for registered refugees , social determinants of young refugees’ health at the individual and environmental levels were mostly unfavorable. Refugees faced language, financial, social, cultural, and educational barriers, as well as gender and stigma-related barriers, to accessing health care services and healthy environments in urban areas. Some of the main themes that emerged during data analysis included: (1) unhealthy living conditions (crowded households, rental costs, unsafe buildings, and problems with access to clean water and heating; see Fig. 10.2a); (2) nutrition and hygiene problems (vitamin and mineral deficiencies, lack of access to healthy food and cooking facilities, and hygiene-related problems—especially by female participants, who were traditionally more involved with this topic; see Fig. 10.2b); (3) barriers to accessing education (financial and language problems, the need to work and earn money to sustain living conditions, inability to find a secure job, low-paying jobs, occupational hazards, and the need for vocational trainings); (4) child labor (unhealthy working conditions, unregistered employment, and lack of access to primary education for children, especially for those living out of camps; see Fig. 10.2c); (5) early marriage and adolescent pregnancies (polygamy, unregistered marriages, unregistered children, human trafficking issues, gender inequalities, low health literacy, language and cultural barriers to accessing health care, lack of awareness on available health services, problems in access to reliable health information, and low uptake of preventive services); and (6) high mobility and uncertainty (unregistered refugees, dreams to return to home country or to move to another country, adaptation problems, problems arising with moving from one city to another including limited access to services without an updated registration, continuous uncertainty in life, acceptance problems including stigma and discrimination toward refugees, and mental health problems; see Fig. 10.2d).




(a–d) Example photos taken by youth and used in analysis, reporting, and dissemination of research findings. (Reproduced with permission from the author. Copyright © 2016 Ozge Karadag Caman. All rights reserved)
The findings above were the main themes that emerged—with mutual agreement among the study participants—during the two group discussion meetings. Several other issues were also brought up by some of the participants; however, after discussing those issues in the larger group, they were found to be very rare, individual-level experiences that were not shared or experienced by most of the participants, and hence were not included among the major themes that emerged. There were also several ethical concerns that arose during the group discussions and during selection of the photos for wider dissemination in the photo exhibitions and publications. Although all photos were either taken with permission or did not show people’s faces for privacy reasons, there were still some concerns about potential identification of some people, including some minors. Therefore, photos that were not found suitable for wider dissemination were extracted from the database and were not shared in any electronic or printed medium.
3.1 Advocacy Through Dissemination
In the study, data analysis with feedback and contribution of participants was followed by the production of short reports, conference papers, and other publications for disseminating findings to different stakeholders, such as academics, civil society members, and policy makers at the national and international level. These written documents for dissemination were written by the primary investigator with input from the youth throughout the process. The youth also selected which photos would be used in the dissemination efforts and co-wrote the quotes to use with the photos. The publications were coupled with advocacy activities, such as photo exhibitions that brought together policy makers, health service providers, civil society organizations, host communities, and young people to achieve positive change through joint action. The photo exhibition—which was organized on World Refugee Day (June 20, 2016) with the joint efforts of the Community Volunteers Foundation, UNFPA, and a municipality in Ankara—attracted a large number of visitors from different sectors and resulted in high media coverage of the different young refugee stories. In the exhibitions, each photo was displayed with the name of the participant, the name of the photographer, and a short excerpt from the participant’s own words, hence combining photos with voices. Youth participants also attended the photo exhibitions and interacted with policy makers and other stakeholders, and some of them were interviewed by journalists, later appearing in newspapers with their photos and stories. Although the project team did not use a specific evaluation method for these exhibits, verbal reflections of the exhibition participants indicated that both the photos and the young people’s physical presence in the exhibitions were the major contributors to raising awareness and increasing observers’ perception of the reality of problems faced by young people.
4 Discussion
The present qualitative study aimed to use a CBPAR approach to assess public health problems faced by young refugees in Turkey. The study also aimed to advocate for their health rights, as well as to involve young refugees in health promotion research and have their voices heard by policy makers. The findings of this photovoice study indicated that refugees living in urban areas faced serious problems regarding shelter, education, employment, income, and access to health services, in addition to language barriers, cultural differences, stigma, and discrimination. There was a significant gender-based difference between the challenges faced by young refugees, indicating a need to tailor unique approaches based on gender.
The overall experience of young people with the photovoice approach was found to be very positive. This particular approach enabled the researchers to involve participants actively throughout the research process, while helping the research team to compare their experience with different research methods and question their own roles and limitations in the research processes. The team agreed that active involvement of study participants contributed to the research process in many different ways and increased the validity of findings and the quality of research in general. These positive outcomes can mainly be attributed to the continuous feedback that was received from the participants. In traditional research, there is usually a one-way flow of data, where all data are analyzed and then interpreted by the researchers. On the other hand, when properly facilitated, participatory approaches like photovoice enrich the data analysis and interpretation process by enabling the flow of data, information, ideas, and suggestions in two directions throughout the whole process (from participants to researchers and vice versa).
Community involvement is usually described as the involvement of communities in the planning, implementation, and evaluation of policies and practices. In disaster or humanitarian settings, many programs implemented by governments and non-governmental organizations have been found to be successful during the initial phase of responses but to effect decreasing success as time passes. There can be many reasons for this phenomenon; however, lack of participation and capacity building of the affected communities remains a major factor in inadequate sustainability (Rajeev 2014). Literature shows that in the past, important decisions were made by higher authorities based on their perception of the communities’ needs, where the affected communities served as passive receivers of aid. This approach was typically ineffective because it failed to meet the real needs of communities (Pandey and Okazaki 2012). Previous experience indicated that community members need to be involved from the initial phase of responses and should continue to be involved in later stages, including long-term development efforts. Equitable partnerships require sharing power, resources, credit, results, knowledge, and skills at each stage of the research project, including problem definition, research design, data collection, data analysis, results interpretation, and determination of how the results should be used for action (Minkler and Wallerstein 2008). Unless people are involved in research-related decisions—and, therefore, included as research partners, or (co-)researchers—it is not participatory research, but rather an example of pseudo-participation (Bergold and Thomas 2012). In truly participatory research, community members have control (shared leadership) over the research, and they are more likely to accept the legitimacy of the research and pay attention to its findings if they know it was conducted by people like themselves. Participatory research also trains citizen researchers, who can turn their skills to other community-level problems. Skills learned by researchers in the course of participatory research are also carried over into other areas of researchers’ lives (University of Kansas 2018). However, when working with youth, we found that several adaptations to a traditional CBPAR approach were necessary to achieve project goals within study constraints.
First, due to organizational and financial reasons, the preparation stage of our photovoice study was comparatively less participatory than later stages; however, the data collection, analysis, and dissemination stages were very dynamic with continuous communication between all project stakeholders. In an ideal participatory research setting, the preparation stage should be as participatory as the following stages, but this was not an option in our study. Despite the initial phase, our overall experience showed that when compared to other research approaches, participatory action research was more effective in developing concrete plans for disseminating findings and driving advocacy to create a change. In our own experience, the high motivation of the research team and the participants was kept alive throughout the process due to the collaborative and iterative nature of the study. This approach provided an opportunity to discuss study findings, revisit data for further analysis, and prepare dissemination and advocacy materials with the continuous contribution of the participants. The photovoice approach also helped to improve social cohesion and social ties between refugee and local youth, in addition to building partnerships among different stakeholders for more comprehensive youth health promotion efforts—covering potential changes at the individual, social, and environmental levels. Overall, research-related costs were not high, and outputs (visual findings and stories) were more attractive for, and easy to grasp by, the target audience.
Second, the language barrier between the principal investigator and the refugees might have affected some of the group interactions as well as the interpretation of some of the findings, although this limitation was thought to be minimal since the facilitators that translated all group discussions and the local participants that contributed to the translation process during group discussions were bilingual. In contrast to studies using qualitative interviews, photovoice studies are less affected by language barriers, since photos, which are taken by the participants, either complement or speak more strongly than words. In addition to these issues, it was challenging to build and sustain collaboration and to share decision-making between all partners, especially when the partners are youth who have important lived experiences but are typically less experienced in political and financial processes to make sustained change. Considering these challenges, this study aimed to bring together youth who has local wisdom with stakeholders who have expertise in research, advocacy, and policy making for all partners to learn from each other and to plan more concrete actions for social change.
Although this qualitative study was conducted with a rather small sample size in one city, the findings still point to an urgent need for developing multidimensional and multi-sectoral interventions on health, education, employment, and gender issues regarding young refugees in Turkey. Within this framework, potential interventions that were brought up during group discussions were: (1) increasing health literacy and awareness on available health care services; (2) improving social determinants of health, including the promotion of healthy living and working conditions; (3) increasing awareness of policy makers and service providers on gender inequities and how to tackle them; (4) decreasing refugee-related stigma among local communities; and (5) empowering young refugees and promoting their social and mental health. In this regard, it was agreed that community involvement should be an integral part of these interventions in order for the health promotion responses to be successful and linked to sustainable development efforts in the long term, because effective participation and capacity building of the affected communities are critical factors for sustainability.
In the present study, social cohesion of refugee and host communities—as well as increased motivation of local young people (host communities) to think about problems faced by their refugee peers—were additional gains, since working in mixed groups can strengthen social ties and values to build a shared environment between refugee and local youth. Thus, while photovoice can be a strong “tool” for health promotion research and advocacy, our experience demonstrates that the photovoice approach has a strong potential to act as a “bridge” to create synergy (See Chaps. 1 and 21, this volume for further background on these concepts). In the context of our study, photovoice methodology created social bridges in many different ways. First, photovoice was often a language bridge for young people, who experienced forced migration from a neighboring country with a different language and a different alphabet. Depending upon their experiences getting to and living in the host country, photovoice might also have helped to create a channel for young people to talk about their migration-related traumas or challenges. This participatory methodology and the mixed nature of the study group created a bridge between refugee and local youth, building connections and feelings of belonging and mutual understanding. Photovoice also acted as a bridge to policy makers and other stakeholders, who had the power to create system-level changes. By seeing the photos and reading the quotations, they might have felt something viscerally that moved them, through empathy, to change certain policies and/or practices.
5 Conclusion
The number of studies using CBPAR methodology with refugees/migrants is still scarce. Therefore, despite some of its limitations, the project described in this chapter may potentially motivate health promotion researchers and professionals to involve vulnerable or disadvantaged populations in future health promotion research and practice. In particular, photovoice might be very helpful in understanding real-life problems of minority populations, as well as in supporting them with tools and bridges to identify and advocate for their own solutions. This experience indicated that photovoice, as one of the CBPAR approaches, can be used more widely with vulnerable or disadvantaged groups to promote health and decrease inequalities. In forced migration settings, photovoice can also facilitate social cohesion of refugee and local individuals, and photography can be a strong tool to engage refugees in health promotion work.
In conclusion, participation of refugees in refugee-related research, policy, and practice in host countries—as well as in the promotion of their own health—is essential for efficiently using available resources and planning culturally appropriate interventions in the short term, and for supporting sustainable development efforts of host countries in the long term.
References
Bergold, J., & Thomas, S. (2012). Participatory research methods: A methodological approach in motion. Historical Social Research, 37(4), 191–222. https://doi.org/10.12759/hsr.37.2012.4.191-222.
Budig, K., Diez, J., Conde, P., Sastre, M., Hernán, M., & Franco, M. (2018). Photovoice and empowerment: Evaluating the transformative potential of a participatory action research project. BMC Public Health, 18(1), 432. https://doi.org/10.1186/s12889-018-5335-7.
Center for Community Health and Development, University of Kansas. Community tool box, Section 2. Community-based participatory research. https://ctb.ku.edu/en/table-of-contents/evaluate/evaluation/intervention-research/main. Accessed 24 Nov 2018.
Department General of Migration Management, Turkish Ministry of Interior. (2019). Migration statistics: June, 2019. https://www.goc.gov.tr/icerik6/gecici-koruma_363_378_4713_icerik. Accessed 14 June 2019.
Holkup, P. A., Tripp-Reimer, T., Salois, E. M., & Weinert, C. (2004). Community-based participatory research: An approach to intervention research with a native American community. Advances in Nursing Science, 27(3), 162–175.
International Organization for Migration (IOM). (2018). World migration report. https://www.iom.int/wmr/world-migration-report-2018. Accessed 26 Nov 2018.
Karadag Caman, O. (2015). Needs assessment study among young Syrian refugees on health, education, employment and gender issues in Turkey: Final report. Ankara: Community Volunteers Foundation, Yuva Association, UNFPA.
Karadag Caman, O., & Altintas, K. H. (2010). Refugees and health. TAF Prev Med Bull, 9(1), 55–62.
Karadag Caman, O., & Bahar Ozvaris, S. (2010). International migration and women’s health. Health and Society, 20(4), 3–14.
Kaya, A., & Kiraç, A. (2016). Vulnerability assessment of Syrian refugees in Istanbul. Support to Life.
Mack, N., Woodsong, C., Macqueen, K., Guest, G., & Namey, E. (2005). Qualitative research methods: A data collector’s field guide. USAID/Family Health International.
Minkler, M., & Wallerstein, N. (Eds.). (2008). Community-based participatory research for health: From process to outcomes (2nd ed.). San Francisco: Jossey-Bass.
Norwegian Refugee Council. (2018). 10 challenges of refugee youth. https://www.nrc.no/news/2018/august/10-challenges-of-refugee-youth/. Accessed 18 Nov 2018.
Pandey, B., & Okazaki, K. (2012). Community-based disaster management: Empowering communities to cope with disaster risks. United Nations Centre for Regional Development, Japan.
Rajeev, M. M. (2014). Sustainability and community empowerment in disaster management. International Journal of Social Work and Human Services Practice, 2(6), 207–212.
UNHCR. (1951). UN Convention relating to the status of refugees. http://www.unhcr.org.tr/MEP/FTPRoot/HTMLEditor/File/anasayfa/sozles me.pdf. Accessed 10 Dec 2018.
UNHCR. (2017). 3RP progress report: regional refugee & resilience plan 2017–2018. https://data2.unhcr.org/en/documents/download/60340. Accessed 28 Nov 2018.
UNHCR. (2019). Syria emergency. http://www.unhcr.org/en-us/syria-emergency.html. Accessed 12 June 2019.
United Nations. (2018). Refugees. http://www.un.org/en/sections/issues-depth/refugees/. Accessed 12 Nov 2018.
Wang, C. (1999). Photovoice: A participatory action research strategy applied to women’s health. Journal of Women’s Health, 8, 185–192.
Wang, C., & Burris, M. A. (1997). Photovoice: Concept, methodology, and use for participatory needs assessment. Health Education & Behavior, 24(3), 369–387.
Wang, C. C., Yi, W. K., Tao, Z. W., & Carovano, K. (1998). Photovoice as a participatory health promotion strategy. Health Promotion International, 13(1), 75–86. https://doi.org/10.1093/heapro/13.1.75.
Wang, C. C., Morrel-Samuels, S., Hutchison, P. M., Bell, L., & Pestronk, R. M. (2004). Flint photovoice: Community building among youths, adults, and policymakers. American Journal of Public Health, 94(6), 911–913.
Women’s Refugee Commission, United Nations Refugee Agency, United Nations Population Fund. (2016). Initial assessment report: protection risks for women and girls in the European refugee and migrant crisis. https://www.unhcr.org/en-us/protection/operations/569f8f419/initial-assessment-report-protection-risks-women-girls-european-refugee.html
Acknowledgements
The author is thankful to all the participants and facilitators of the photovoice study and acknowledges with appreciation the invaluable support provided by the Community Volunteers Foundation, the Yuva Association, and the UNFPA Country Office in Turkey during data collection and organization of the photo exhibition.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License (http://creativecommons.org/licenses/by-nc-nd/4.0/), which permits any noncommercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if you modified the licensed material. You do not have permission under this license to share adapted material derived from this chapter or parts of it.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2021 The Author(s)
About this chapter

Cite this chapter
Karadag Caman, O. (2021). Photovoice for Health Promotion Research, Empowerment, and Advocacy: Young Refugee Stories from Turkey. In: Corbin, J.H., Sanmartino, M., Hennessy, E.A., Urke, H.B. (eds) Arts and Health Promotion. Springer, Cham. https://doi.org/10.1007/978-3-030-56417-9_10
Download citation
DOI: https://doi.org/10.1007/978-3-030-56417-9_10
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-56416-2
Online ISBN: 978-3-030-56417-9
eBook Packages: MedicineMedicine (R0)