
Abstract
Positron emission tomography (PET) using different radiotracers evaluating different metabolic patterns is able to early detect pathophysiological changes in oncological patients, including those with brain tumours. These functional changes usually occur before the development of morphological changes detected by conventional radiological imaging techniques such as computed tomography (CT) and magnetic resonance imaging (MRI) [1]. MRI is the standard neuroimaging method used for diagnosis of brain tumours, for performing stereotactic biopsy and surgical planning in neuro-oncology [2]. Currently, hybrid imaging techniques as PET/CT and PET/MRI, providing a combination of both functional and morphological information, may be useful methods for early diagnosis of brain tumours [1, 2].
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others

1 Background
Positron emission tomography (PET) using different radiotracers evaluating different metabolic patterns is able to early detect pathophysiological changes in oncological patients, including those with brain tumours. These functional changes usually occur before the development of morphological changes detected by conventional radiological imaging techniques such as computed tomography (CT) and magnetic resonance imaging (MRI) [1]. MRI is the standard neuroimaging method used for diagnosis of brain tumours, for performing stereotactic biopsy and surgical planning in neuro-oncology [2]. Currently, hybrid imaging techniques as PET/CT and PET/MRI, providing a combination of both functional and morphological information, may be useful methods for early diagnosis of brain tumours [1, 2].
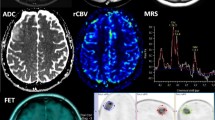
Different PET radiotracers have been used to evaluate brain tumours including fluorine-18 fluorodeoxyglucose (18F-FDG), carbon-11 methionine (11C-methionine), fluorine-18 fluoroethyltyrosine (18F-FET), fluorine-18 fluorodihydroxyphenylalanine (18F-FDOPA), fluorine-18 fluorothymidine (18F-FLT) and radiolabelled choline (11C-choline or 18F-choline).
Enough literature data already exist about the diagnostic performance and prognostic value of PET with different tracers in brain tumours. In particular, 24 meta-analyses on the use of PET or PET/CT with different tracers in brain tumours, published from 2012, were selected through a comprehensive computer literature search [3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26]. The findings of the selected meta-analyses on the diagnostic performance are presented in Table 3.1. Here below we have summarized the main findings of meta-analytic studies based on the different clinical indications of PET or PET/CT.
2 Evaluation of Suspicious Primary Brain Tumour
Four meta-analyses have assessed the diagnostic performance of PET or PET/CT with different tracers in patients for whom primary brain tumours are suspected [3, 20, 23, 26].
2.1 18F-FDG
A meta-analysis including patients with suspicious primary brain tumours showed that 18F-FDG PET or PET/CT has a moderate sensitivity and specificity for differentiating brain tumours from non-tumour lesions. False-positive findings were often due to inflammatory lesions or other non-tumour tissues; on the other hand, reduced 18F-FDG uptake in brain tumours is usually influenced by the high physiological glucose metabolism in surrounding normal brain tissue, leading to a decreased sensitivity [23]. Another meta-analysis also demonstrated that 18F-FDG PET or PET/CT has a moderate diagnostic performance in distinguishing between tumour and non-tumour lesions in the brain, lower than amino acid PET [20].
2.2 11C-Methionine
A meta-analysis by Zhao et al. demonstrated a good diagnostic performance of 11C-methionine PET or PET/CT in detecting brain tumours (pooled sensitivity and specificity were of 95% and 83%, respectively) with higher diagnostic accuracy values compared to 18F-FDG PET or PET/CT, likely due to the higher 11C-methionine uptake in brain tumours and lower accumulation in normal brain tissue [23].
2.3 18F-FET
For initial assessment of patients with a newly diagnosed brain lesion, 18F-FET PET or PET/CT demonstrated a good performance in the diagnosis of a brain tumour with a pooled sensitivity and specificity of 82% and 76%, respectively. A mean tumour-to-background uptake ratio (TBR) threshold of at least 1.6 and a maximum TBR of at least 2.1 had the best diagnostic value for differentiating brain tumours from non-tumour brain lesions. For the diagnosis of glioma versus non-glioma brain lesions, 18F-FET PET or PET/CT demonstrated a good sensitivity (84%) but a not adequate specificity (62%) [26]. In a head-to-head comparative meta-analysis, the diagnostic performance of 18F-FET PET or PET/CT in distinguishing between tumour and non-tumour lesions in the brain was found significantly higher compared to that of 18F-FDG PET or PET/CT performed in the same patients [20].
2.4 18F-FDOPA
18F-FDOPA PET or PET/CT revealed a moderate sensitivity (71%) and a good specificity (86%) in detecting newly diagnosed gliomas [3].
3 Glioma Grading
Gliomas are the most frequent primary brain tumours. High-grade gliomas like glioblastomas are the most common gliomas in adults, with a poor prognosis with any current therapy. Conversely, low-grade gliomas, the second most common type of gliomas, are potentially curable with appropriate treatment. Several meta-analyses have evaluated the role of PET or PET/CT with different tracers in differentiating between high-grade and low-grade gliomas [3, 6, 14, 20].
3.1 18F-FDG
18F-FDG uptake is significantly higher in high-grade gliomas compared with low-grade gliomas. According to the meta-analysis of Dunet et al., a mean TBR of at least 1.4 and a maximum TBR of at least 1.8 at 18F-FDG PET had the best value to distinguish between low- and high-grade gliomas, with a sensitivity, specificity and accuracy of 60%, 91% and 74%, respectively, for mean TBR and 72%, 73% and 72%, respectively, for maximum TBR [20]. A recent meta-analysis demonstrated a lower sensitivity of 18F-FDG PET or PET/CT in differentiating between high-grade and low-grade gliomas compared to radiolabelled amino acid PET (11C-methionine and 18F-FET) but with higher specificity [6].
3.2 11C-Methionine
11C-methionine PET or PET/CT had a moderate diagnostic accuracy in differentiating between high-grade and low-grade gliomas, according to data provided by a recent meta-analysis (pooled sensitivity and specificity of 80% and 72%, respectively) [14]. Another meta-analysis demonstrated that 11C-methionine PET or PET/CT has a higher sensitivity compared to 18F-FDG PET or PET/CT in differentiating between high-grade and low-grade gliomas but with lower specificity; diagnostic performance values were similar to those of 18F-FET PET or PET/CT in this setting [6].
3.3 18F-FET
18F-FET uptake is significantly higher in high-grade gliomas compared with low-grade gliomas. Dunet et al. reported that a mean TBR of at least 2.0 and a maximum TBR of at least 3.0 at 18F-FET PET reached a sensitivity, specificity and accuracy of 88%, 73% and 81%, respectively, for mean TBR, and 80%, 82% and 81%, respectively, for maximum TBR [20]. A recent meta-analysis demonstrated that 18F-FET PET or PET/CT has a higher sensitivity compared to 18F-FDG PET or PET/CT in differentiating between high-grade and low-grade gliomas but with lower specificity; diagnostic performance values were similar to those of 11C-methionine PET or PET/CT in this setting [6].
3.4 18F-FDOPA
For differentiating high-grade from low-grade gliomas, 18F-FDOPA PET or PET/CT showed a pooled sensitivity of 88% and a pooled specificity of 73% [3].
4 Delineation of Gliomas
For surgical and radiation therapy planning in patients with glioma, a correct delineation of the target volume is needed. A recent evidence-based article suggested that radiolabelled amino acid PET may ameliorate the delineation of high-grade gliomas compared to standard MRI [16].
5 Diagnosis of Recurrent Brain Tumours
Distinguishing recurrent brain tumours from non-tumour lesions after radiation therapy and/or chemotherapy is a crucial clinical issue, because the different diagnosis will lead to divergent treatments. Several meta-analyses have assessed the diagnostic performance of PET with different tracers in this setting [3, 4, 7, 9, 11, 13, 21,22,23,24,25].
5.1 18F-FDG
A meta-analysis of Zhao et al. demonstrated a moderate diagnostic accuracy of 18F-FDG PET or PET/CT in detecting brain tumour recurrence [23]. This finding was confirmed by another meta-analysis which showed a pooled sensitivity and specificity of 78% and 77%, respectively [21]. Furuse et al. showed that the diagnostic performance of 18F-FDG PET or PET/CT in detecting recurrent brain tumours was lower compared to that of radiolabelled amino acid PET or PET/CT [7]. Nihashi et al. showed that, when considering both low- and high-grade gliomas, pooled sensitivity and specificity of 18F-FDG PET or PET/CT in detecting glioma recurrence were 77% and 78%, respectively. In subgroup analyses limited to high-grade gliomas, pooled sensitivity and specificity were 79% and 70%, respectively [25]. Wang et al. reported a moderate sensitivity (70%) but a good specificity (88%) of 18F-FDG PET or PET/CT in detecting recurrent glioma; however, the diagnostic accuracy was lower compared to that of 11C-methionine PET or PET/CT and magnetic resonance spectroscopy in this setting [22]. Another meta-analysis demonstrated that the diagnostic performance of 18F-FDG PET or PET/CT in detecting recurrent glioma is not optimal, in particular if compared with other available neuroimaging methods [7].
5.2 11C-Methionine
11C-methionine PET or PET/CT demonstrated good diagnostic performance in detecting brain tumour recurrence (pooled sensitivity and specificity of 92% and 87%, respectively), with higher values compared to 18F-FDG PET or PET/CT [23]. For high-grade gliomas, pooled sensitivity and specificity of 11C-methionine PET or PET/CT in detecting glioma recurrence were 70% and 93%, respectively [25]. Compared to dynamic susceptibility contrast-enhanced MRI, 11C-methionine PET or PET/CT demonstrated comparable pooled sensitivity and specificity in detecting glioma recurrence, with pooled values of 87% and 81.3%, respectively [24]. Similar values of sensitivity and specificity (85% and 83%, respectively) were described by Wang et al., which demonstrated that the diagnostic performance of 11C-methionine PET or PET/CT in detecting glioma recurrence was similar to that of magnetic resonance spectroscopy [22]. A large meta-analysis including 29 studies confirmed the good diagnostic performance of 11C-methionine PET or PET/CT in this setting with a pooled sensitivity and specificity of 88% and 85%, respectively [13].
5.3 18F-FET
A recent meta-analysis demonstrated that 18F-FET PET or PET/CT has a good diagnostic accuracy in differentiating between brain tumour recurrence and radiation necrosis after treatment, with pooled sensitivity and specificity values of 82% and 80%, respectively. In the subgroup of patients with suspicious glioma recurrence, sensitivity and specificity of 18F-FET PET or PET/CT were 83% and 81%, respectively [11]. The good diagnostic performance of 18F-FET PET or PET/CT in this setting was also confirmed by Furuse et al. who reported increased diagnostic performance of 18F-FET PET or PET/CT compared to 18F-FDG and 11C-methionine PET or PET/CT [7]. Kim et al. found that amino acid PET or PET/CT, including 18F-FET PET, has a good diagnostic performance in differentiating residual or recurrent brain tumour from treatment-related changes (pseudoprogression) in patients with high-grade gliomas [4].
5.4 18F-FDOPA
A recent meta-analysis indicated that 18F-FDOPA PET or PET/CT has a good diagnostic accuracy in differentiating between brain tumour recurrence and radiation necrosis after treatment, with pooled sensitivity and specificity values of 85% and 77%, respectively. In the subgroup of patients with suspicious glioma recurrence, sensitivity and specificity of 18F-FDOPA PET or PET/CT were 94% and 89%, respectively [11]. Xiao et al. reported a good sensitivity of 18F-FDOPA PET and PET/CT in detecting recurrent glioma (92%) and a moderate specificity (76%) [3].
5.5 18F-FLT
18F-FLT PET or PET/CT demonstrated a similar diagnostic performance in detecting brain tumour recurrence compared to 18F-FDG PET or PET/CT with pooled sensitivity and specificity of 82% and 76%, respectively [21].
5.6 18C-Choline
A recent meta-analysis indicated that 11C-choline PET or PET/CT has a good diagnostic accuracy for differentiating glioma recurrence from radiation induced necrosis after treatment, with a pooled sensitivity and specificity of 87% and 82%, respectively [9].
6 Diagnosis of Brain Metastases
The reliability of PET or PET/CT with different tracers in detecting brain metastases has been evaluated to a less extent compared to primary brain tumours. A meta-analysis demonstrated that the pooled sensitivity and specificity of 18F-FDG PET or PET/CT in detecting brain metastases in patients with lung cancer were 21% and 100%, respectively. In particular, the sensitivity of this method is lower compared to that of contrast-enhanced MRI [19].
7 Diagnosis of Recurrent Brain Metastases
The meta-analysis of Li et al., focused on the use of PET or PET/CT with different tracers in differentiating recurrent brain metastasis from radionecrosis after radiation therapy, demonstrated a good diagnostic accuracy of PET or PET/CT with both 18F-FDG and radiolabelled amino acid tracers (11C-methionine, 18F-FET, 18F-FDOPA) in this setting [12]. MRI and PET with different tracers showed similar diagnostic performance for the detection of recurrent brain metastasis after stereotactic radiosurgery; nevertheless, advanced MRI methods showed a significantly higher diagnostic performance in this setting compared to PET [8].
8 Diagnosis of Primary Central Nervous System Lymphoma (PCNSL)
18F-FDG PET and PET/CT showed considerable accuracy in identifying PCNSL among various brain lesions in immunocompetent patients (pooled sensitivity and specificity of 88% and 86%, respectively), therefore, 18F-FDG PET/CT could be a valuable diagnostic imaging method in this setting [17]. High diagnostic accuracy of 18F-FDG PET and PET/CT has also been demonstrated in identifying PCNSL among various brain lesions in patients with human immunodeficiency virus (HIV) infection [18].
9 Prognostic Value in Patients with Glioma
Beyond the diagnostic accuracy, PET/CT parameters, and particularly the TBR, may be significant prognostic factors in patients with glioma. A recent meta-analysis demonstrated that increased TBR at 18F-FDG PET, 11C-methionine PET and 18F-FET PET could indicate poor overall survival (pooled hazard ratios were 3.05 for 18F-FDG PET, 1.59 for 11C-methionine PET and 1.15 for 18F-FET PET) [5]. Another meta-analysis showed that the TBR and metabolic tumour volume at 11C-methionine PET are significant prognostic parameters for patients with gliomas. Patients with a high TBR have a higher risk of death, and patients with a high metabolic tumour volume have a higher risk of adverse events or death [10].
10 Conclusions
Evidence-based data demonstrated good diagnostic performance of PET with different tracers in detecting brain tumours, in particular radiolabelled amino acid tracers showed the highest diagnostic performance values. All the PET tracers evaluated had significant prognostic value in patients with glioma [27].
References
Treglia G, Sadeghi R, Del Sole A, Giovanella L. Diagnostic performance of PET/CT with tracers other than F-18-FDG in oncology: an evidence-based review. Clin Transl Oncol. 2014;16:770–5.
Muoio B, Giovanella L, Treglia G. Recent developments of 18F-FET PET in neuro-oncology. Curr Med Chem. 2018;25:3061–73.
Xiao J, Jin Y, Nie J, Chen F, Ma X. Diagnostic and grading accuracy of (18)F-FDOPA PET and PET/CT in patients with gliomas: a systematic review and meta-analysis. BMC Cancer. 2019;19:767.
Kim SJ, Ryul Shim S. Diagnostic value of radiolabeled amino acid PET for detection of pseudoprogression of brain tumor after treatment: a meta-analysis. Nucl Med Commun. 2019;40:965–72.
Zhang Q, Gao X, Wei G, Qiu C, Qu H, Zhou X. Prognostic value of MTV, SUVmax and the T/N ratio of PET/CT in patients with glioma: a systematic review and meta-analysis. J Cancer. 2019;10:1707–16.
Katsanos AH, Alexiou GA, Fotopoulos AD, Jabbour P, Kyritsis AP, Sioka C. Performance of 18F-FDG, 11C-methionine, and 18F-FET PET for glioma grading: a meta-analysis. Clin Nucl Med. 2019;44(11):864–9.
Furuse M, Nonoguchi N, Yamada K, Shiga T, Combes JD, Ikeda N, et al. Radiological diagnosis of brain radiation necrosis after cranial irradiation for brain tumor: a systematic review. Radiat Oncol. 2019;14:28.
Suh CH, Kim HS, Jung SC, Choi CG, Kim SJ. Comparison of MRI and PET as potential surrogate endpoints for treatment response after stereotactic radiosurgery in patients with brain metastasis. AJR Am J Roentgenol. 2018;211:1332–41.
Gao L, Xu W, Li T, Zheng J, Chen G. Accuracy of 11C-choline positron emission tomography in differentiating glioma recurrence from radiation necrosis: a systematic review and meta-analysis. Medicine. 2018;97:e11556.
Kim YI, Kim Y, Lee JY, Jang SJ. Prognostic value of the metabolic and volumetric parameters of (11)C-methionine positron-emission tomography for gliomas: a systematic review and meta-analysis. AJNR Am J Neuroradiol. 2018;39:1629–34.
Yu J, Zheng J, Xu W, Weng J, Gao L, Tao L, et al. Accuracy of (18)F-FDOPA positron emission tomography and (18)F-FET positron emission tomography for differentiating radiation necrosis from brain tumor recurrence. World Neurosurg. 2018;114:e1211–24.
Li H, Deng L, Bai HX, Sun J, Cao Y, Tao Y, et al. Diagnostic accuracy of amino acid and FDG-PET in differentiating brain metastasis recurrence from radionecrosis after radiotherapy: a systematic review and meta-analysis. AJNR Am J Neuroradiol. 2018;39:280–8.
Xu W, Gao L, Shao A, Zheng J, Zhang J. The performance of 11C-methionine PET in the differential diagnosis of glioma recurrence. Oncotarget. 2017;8:91030–9.
Falk Delgado A, Falk DA. Discrimination between primary low-grade and high-grade glioma with (11)C-methionine PET: a bivariate diagnostic test accuracy meta-analysis. Br J Radiol. 2018;91:20170426.
Yang Y, He MZ, Li T, Yang X. MRI combined with PET-CT of different tracers to improve the accuracy of glioma diagnosis: a systematic review and meta-analysis. Neurosurg Rev. 2019;42:185–95.
Verburg N, Hoefnagels FWA, Barkhof F, Boellaard R, Goldman S, Guo J, et al. Diagnostic accuracy of neuroimaging to delineate diffuse gliomas within the brain: a meta-analysis. AJNR Am J Neuroradiol. 2017;38:1884–91.
Zou Y, Tong J, Leng H, Jiang J, Pan M, Chen Z. Diagnostic value of using 18F-FDG PET and PET/CT in immunocompetent patients with primary central nervous system lymphoma: a systematic review and meta-analysis. Oncotarget. 2017;8:41518–28.
Yang M, Sun J, Bai HX, Tao Y, Tang X, States LJ, et al. Diagnostic accuracy of SPECT, PET, and MRS for primary central nervous system lymphoma in HIV patients: a systematic review and meta-analysis. Medicine. 2017;96:e6676.
Li Y, Jin G, Su D. Comparison of gadolinium-enhanced MRI and 18FDG PET/PET-CT for the diagnosis of brain metastases in lung cancer patients: a meta-analysis of 5 prospective studies. Oncotarget. 2017;8:35743–9.
Dunet V, Pomoni A, Hottinger A, Nicod-Lalonde M, Prior JO. Performance of 18F-FET versus 18F-FDG-PET for the diagnosis and grading of brain tumors: systematic review and meta-analysis. Neuro Oncol. 2016;18:426–34.
Li Z, Yu Y, Zhang H, Xu G, Chen L. A meta-analysis comparing 18F-FLT PET with 18F-FDG PET for assessment of brain tumor recurrence. Nucl Med Commun. 2015;36:695–701.
Wang X, Hu X, Xie P, Li W, Li X, Ma L. Comparison of magnetic resonance spectroscopy and positron emission tomography in detection of tumor recurrence in posttreatment of glioma: a diagnostic meta-analysis. Asia Pac J Clin Oncol. 2015;11:97–105.
Zhao C, Zhang Y, Wang J. A meta-analysis on the diagnostic performance of (18)F-FDG and (11)C-methionine PET for differentiating brain tumors. AJNR Am J Neuroradiol. 2014;35:1058–65.
Deng SM, Zhang B, Wu YW, Zhang W, Chen YY. Detection of glioma recurrence by 11C-methionine positron emission tomography and dynamic susceptibility contrast-enhanced magnetic resonance imaging: a meta-analysis. Nucl Med Commun. 2013;34:758–66.
Nihashi T, Dahabreh IJ, Terasawa T. Diagnostic accuracy of PET for recurrent glioma diagnosis: a meta-analysis. AJNR Am J Neuroradiol. 2013;34:944–50.
Dunet V, Rossier C, Buck A, Stupp R, Prior JO. Performance of 18F-fluoro-ethyl-tyrosine (18F-FET) PET for the differential diagnosis of primary brain tumor: a systematic review and metaanalysis. J Nucl Med. 2012;53:207–14.
Treglia G, Muoio B, Trevisi G, Mattoli MV, Albano D, Bertagna F, et al. Diagnostic performance and prognostic value of PET/CT with different tracers for brain tumors: a systematic review of published meta-analyses. Int J Mol Sci. 2019;20(19):E4669.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2020 The Author(s)
About this chapter

Cite this chapter
Treglia, G., Muoio, B. (2020). Evidence-Based PET for Brain Tumours. In: Treglia, G., Giovanella, L. (eds) Evidence-based Positron Emission Tomography. Springer, Cham. https://doi.org/10.1007/978-3-030-47701-1_3
Download citation
DOI: https://doi.org/10.1007/978-3-030-47701-1_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-47700-4
Online ISBN: 978-3-030-47701-1
eBook Packages: MedicineMedicine (R0)