
Abstract
The identification of interactions among parameters of health risk factors is a crucial step for the effective assessment and prevention of problems in unhealthy built environments . This chapter introduces the health risk management process in the context of the designs of healthy built environments (Sect. 4.1). In Sects. 4.2–4.3, comprehensive descriptions of all detected interactions among health risks and their parameters that have harmful impacts on user health and wellbeing are defined. Section 4.2 provides a detailed analysis of single group interactions between:
-
physical-physical,
-
chemical-chemical,
-
chemical-physical,
-
chemical-biological,
-
biological-biological,
-
biological-physical,
-
personal-physical,
-
personal-chemical, and
-
interactions between other health risk factors and their parameters.
In addition to single group interactions , multi-group interactions among health risk factors and their parameters are also analysed in Sect. 4.3. Additionally, synergistic and antagonistic effects are presented, and the main findings are supported by epidemiological studies. The chapter concludes with the tool developed for decision-making processes (Sect. 4.4) supported by the short-term and long-term benefits of holistic design (Sect. 4.5).
You have full access to this open access chapter, Download chapter PDF
4.1 Health Risk and Management Assessment Model in Built Environments
The term “health risk management” describes the process of evaluating alternative regulatory actions and selection among them. It entails the consideration of political, social, economic, and engineering information with risk-related information to develop, analyse, and compare regulatory options and to select the appropriate regulatory response to a potential health hazard (Paustenbach 2002; Yassi et al. 2001).
In the context of built environments , the health risk and management assessment is a dynamic approach. This process of risk and management assessment includes eight main components (Paustenbach 2002; Yassi et al. 2001):
Risk assessment
-
1.
Hazard identification (single group interactions : interactions between two groups of health risk factors and their parameters; multifactorial interactions are interactive influences among parameters of different groups of risk factors),
-
2.
Dose-response assessment (identify relevant toxicity data),
-
3.
Exposure assessment (identification of exposed populations and exposure pathways, direct and indirect methods for assessment values in different sources of identified parameters),
-
4.
Risk characterization (characterize and summarize potential effects of single and/or multifactorial hazards for adverse health).
Risk management
-
5.
Risk evaluation (defined options from different environmental health factors, socio-economic factors, and political aspects),
-
6.
Risk communication (informed decisions),
-
7.
Control and management of exposure (actions to implement the decisions)
-
8.
Risk management strategy (monitoring and evaluate the effectiveness of the action taken).
4.2 Single-Group Interactions
Single group interactions are interactions between two groups of health risk factors and their parameters, such as physical-physical, chemical-chemical, chemical-physical, chemical-biological, biological-biological, biological-physical, personal-physical, personal-chemical and interactions between other health risk factors and their parameters.
4.2.1 Physical-Physical Interactions
Detected physical-physical interactions are interactive influences among parameters of the group of physical risk factors (Table 4.1).
The first studies on SBS appeared in the 1970s; physical risk factors were primarily examined. The main reasons for this may be related to the introduction of thermal insulated building envelopes , synthetic materials, and the application of mechanical systems. Solutions for lowering energy use were partly defined on the level of thermally improved materials and mechanical systems.
Among physical risk factors, a number of studies examine the correlations between room air temperature , relative air humidity , and ventilation parameters. Additionally, other parameters of physical risk factors, such as noise , daylight, and electromagnetic fields and ions in relation to SBS were examined in a small number of studies.
Full-scale measurements (Omrani et al. 2017) were performed to investigate the effect of natural ventilation mode (i.e., single-sided, cross ventilation) on thermal comfort and ventilation performance. Results highlighted a significantly better performance of cross ventilation over single-sided ventilation. Indoor thermal conditions were found to be within the comfort zone more than 70% of the time under cross ventilation operation while single-sided ventilation provided adequate thermal conditions only 1% of the time.
In the Report by Commission of the European Communities (ECA 1989), indirect effects of low relative air humidity are defined and include static electricity and consequent electric discharges and variations of the respirable suspended particulate matter in indoor environments (ECA 1989). Smallwood (2018) determined that static electricity nuisance shocks have become prevalent since floor covering and shoe sole materials have been increasingly made from highly insulating materials, such as polymers. Additionally, the author concluded that atmospheric humidity has a significant role in floor electrical resistance and static charge build-up (Smallwood 2018).
Industrial machines, ventilation machinery, and other mechanical systems may produce low-frequency noise and vibrations . In current design practice, low-frequency noise and vibrations are often neglected, because they are not perceived. Schwartz (2008) highlighted that high-frequency noises—such as telephones, people talking, and computers—can actually mask the effects of low-frequency noise. If mechanical vibrations in the frequency range below 20 Hz (ground-borne vibrations) affect dwelling rooms, the annoying effects are perceived only by a small portion of exposed individuals as a physical effect (Findeis and Peters 2004).
Even if low-frequency noise is not perceived by occupants, it should not be ignored with regards to the health perspective. In the study on office environment by Burt (1996), low-frequency noise, produced by ventilation systems, was responsible for some of the SBS experienced by the occupants: fatigue, headache, nausea, concentration difficulties, disorientation, motion sickness, digestive disorders, cough, vision problems and dizziness. Burt (1996) concluded that repeated or long-term exposure to such amplified infrasound may trigger an allergic-type response in individuals. Similar findings were found by Hodgson et al. (1987) on vibrations in office environments, showing that an adjacent pump-room caused vibrations that resulted in the occurrence of SBS symptoms among a group of secretaries.
4.2.2 Chemical-Chemical Interactions
Detected chemical-chemical interactions are interactive influences among the parameters of the group of chemical risk factors (Table 4.2).
Studies on chemical risk factors are mainly focused on the links between SBS symptoms exposure to different emission sources, such as construction products, furniture, and household products . They revealed the possible adverse health effects of construction products on building occupants, during normal use of the building or during emergency situations (i.e. fire). Despite those issues, many construction and household products on the market may present potential health concerns. The composition of construction and household products in relation to the content of harmful substances is often questionable; the relevant legislation and inspection are incomplete.
Construction products, household products , furniture, and other equipment may emit harmful substances in the surrounding environment throughout their life cycle (Dovjak and Kristl 2011; Šestan et al. 2013). Wooden construction products and furniture (i.e., plywood, particleboard, fibreboard, oriented strand board (OSB), panel boards, urea-formaldehyde foam, etc.), paints, adhesives, varnishes, floor finishes, disinfectants, cleaning agents, and other household products emit formaldehyde (Šestan et al. 2013). In addition to its widespread use in everyday life, formaldehyde (and its health effects) is one of the most examined harmful substances in relation to construction products and indoor air quality issues. Adverse health effects from exposure to formaldehyde in prefabricated houses, especially irritation of the eyes and upper airways, were first reported in the mid-1960s (Salthammer et al. 2010). Current studies are focused on the potential exposure and cancer risk from formaldehyde emissions from installed construction products (Sheehan et al. 2017). A long-term study of formaldehyde emission decay from particle board has been carried out by Zinn et al. (1990). For products manufactured in 1986 and 1987, the overall three-quarter (75% of initial concentration) and half-lives were 38 and 216 days, respectively (Salthammer et al. 2010).
Polyvinyl chloride (PVC ) construction products, personal-care products, medical devices, detergents and surfactants, packaging, children ’s toys, modelling clay, waxes, paints, printing inks and coatings, pharmaceuticals, food products, and textiles contain phthalates, which are easily released into the environment because there is no covalent bond between the phthalates and plastics (Dovjak and Kristl 2011). The earliest research about their adverse effects on human health was when Šarić et al. (1976) published the article about malignant tumours of the liver and lungs in an area with the PVC industry. In the 1980s and ‘90s, the studies were focused primarily on cancer (Heudorf et al. 2007; Jaakkola et al. 1999; Blount et al. 2000). Moreover, studies in the late 1990s concluded that these chemicals are thought to be endocrine disruptors, responsible for low testosterone levels, declining sperm counts and quality, genital malformations, retarded sexual development or even reproductive abnormalities and increased incidences of certain types of cancer (Heudorf et al. 2007; Blount et al. 2000). Currently, the majority of studies (Jaakkola et al. 1999; Bornehag et al. 2004) showed the association between phthalates and asthma, allergies, or related respiratory effects. In the study by Subedi et al. (2017), concentrations of potentially toxic plasticizers (phthalates, non-phthalates) were investigated in 28 dust samples collected from three different indoor environments across the USA. The observed concentrations of these replacement non-phthalate plasticizers were as high as di-(2-ethylhexyl) phthalate, the most frequently detected phthalate plasticizer at the highest concentration worldwide, in most indoor dust samples. The estimated daily intakes of total phthalates (n = 7) by children and toddlers through indoor dust in childcare facilities were 1.6 times higher than the non-phthalate plasticizers (n = 3), whereas the estimated daily intake of total non-phthalates for all age groups at homes were 1.9 times higher than the phthalate plasticizers. Occupational intake of phthalate and non-phthalate plasticizers through the indoor dust at hair salons was more elevated than at homes in the USA.
In addition to plasticizers , flame retardants are used in a variety of construction products and furniture. Takeuchi et al. (2014) measured 59 compounds, including plasticizers (phthalates, adipates, and others) and flame retardants (organo-phosphates and brominated compounds), from indoor air samples from six houses in Sapporo, Japan. Among the 59 compounds measured in this study, 34 were detected from the indoor air of the six houses. These results suggested that compounds with higher volatility exist preferentially in the gas phase, whereas compounds with lower volatility exist preferentially in the particulate phase in indoor air.
Volatile organic compounds (VOCs) are emitted as gases from certain solids or liquids. VOCs include a variety of chemicals, some of which may have short- and long-term adverse health effects . Concentrations of many VOCs are consistently higher indoors (up to ten times higher) than outdoors (EPA 2017). Sources of VOCs in indoor environments include construction products, furniture, household products (waxes, detergent, insecticides ), products of personal hygiene (cosmetics), do-it-yourself goods (resins), office materials (photocopier ink) or ETS (ECA 1989). A cross-sectional epidemiological study by Azuma et al. (2017) examined the correlation between indoor air quality and building-related symptoms of office workers (N = 107 office workers during winter, 207 office workers during summer) in 17 air-conditioned office buildings in Tokyo, Osaka, and Fukuoka. The study found that several irritating VOCs (e.g., formaldehyde , acetaldehyde, ethylbenzene, toluene, and xylenes) that were positively correlated with the indoor air concentration among their VOCs were associated with upper respiratory symptoms, although their indoor air concentrations were lower than those specified by the indoor air quality guidelines.
Inefficient ventilation systems, incomplete combustion processes, unvented heating, gas cooking, tobacco smoking may result in higher concentrations of other indoor air quality (IAQ) pollutants such as CO2 , CO, NOX, SOX (ECA 1989). IAQ pollutants may present a significant source of odours (ECA 1989, Nakaoka et al. 2014), natural (e.g., users, animals, plants, etc.) or artificial origin (e.g., materials, systems, etc.). Odours are organic or inorganic compounds and can be both pleasant and unpleasant. Some odours can be health hazards, and some are not (CDC 2017).
Users emit bio-effluents (volatile and non-volatile organic compound) and bioaerosols (particles) (Bivolarova et al. 2017). The most commonly known bio-effluent produced by human metabolism is CO2 . Bioaerosols may consist of bacteria, fungi (and spores and cell fragments of fungi), viruses, microbial toxins, pollen, plant fibres, etc. (Douwes et al. 2003). Qualitative and quantitative characterization of bio-effluents and bioaerosols should be considered in the design of ventilation systems.
4.2.3 Chemical-Physical Interactions
Detected chemical-physical interactions are interactive influences among parameters of the group of chemical risk factors and parameters of the group of physical risk factors (parameters of thermal comfort , parameters related to building ventilation systems, noise , vibrations , daylight, EM fields, ions, ergonomic issues, universal design ).
The emission rates of harmful substances from the construction products, household products , furniture, and other indoor sources are influenced by environmental conditions, such as air temperature , surface temperatures , relative humidity of indoor air, air change rate and surface air velocity (ECA 1989; Haghighat et al. 1998; Sakai et al. 2004; Järnström et al. 2006; Blondel and Plaisance 2011; Clausen et al. 2012; Kim et al. 2012; Xu et al. 2009; Nimmermark and Gustafsson 2005). The impact of environmental parameters on the emission behaviours of various compounds was studied in laboratory conditions inside a test chamber or in real built environments . Huang et al. (2015) proved that relative humidity is one of the main environmental factors affecting the emission behaviours of formaldehyde from construction products. The results of their experimental study showed that formaldehyde emissions increased by 10 times as relative humidity increased from 20 to 85%. Xu and Ƶhang (2011) found the opposite, concluding that there is no distinguishable difference in the effective diffusion coefficient of formaldehyde when the relative humidity is between 25 and 50%.
Sakai et al. (2004) performed a comparative study in urban dwellings in Japan and Sweden and proved that indoor concentrations of formaldehyde were increased at higher air temperature and relative humidity. The same findings were reported in the study by Järnström et al. (2006) for new residential buildings in Finland and in the study by Blondel and Plaisance (2011) for students’ rooms in France. Järnström et al. (2006) measured higher concentrations of formaldehyde in summer, at higher air temperatures and relative humidity. Vice versa, lower concentrations were measured in winter, at lower air temperatures and drier air. Blondel and Plaisance (2011) concluded that the rise of formaldehyde emissions from indoor materials correlated with air temperature. Similar findings were confirmed in an experimental study in a test chamber by Zhang et al. (2007), where the increase of air temperature resulted in higher emission rates of formaldehyde from analysed materials.
In addition to air temperature and relative humidity, air velocity also has an important effect on the emissions of indoor materials. In a study by Zhu et al. (2013), the effect of ventilation on the VOCs concentration was analysed by using the developed integrated model for VOCs emission/sorption from/on building materials. The results showed that concentration in the air varies with the same tendency as the air exchange rate.
Pollutant emissions are also related to the type of HVAC system. Chen et al. (2016) studied formaldehyde emissions from porous building material under non-isothermal conditions. Experiments demonstrating the emission of formaldehyde during floor heating and air circulation systems were carried out in a controlled environmental chamber. The results showed that the equilibrium concentration in an airtight chamber with a floor heating system is higher than that in an air circulation heating system.
In addition to formaldehyde emissions, air temperature and relative humidity have a significant effect on the emissions of other indoor air pollutants, such as phthalates, VOCs and odours . Clausen et al. (2012) analysed the influences of air temperature and relative humidity on the emission of di-(2-ethylhexyl) phthalate (DEHP) from PVC flooring. The study concluded that DEHP concentrations increased substantially with increasing air temperature and were independent of the relative humidity. Similarly, the study by Nimmermark and Gustafsson (2005) showed that odour emission increased significantly with air temperature at constant ventilation rates. A comprehensive literature review by Haghighat et al. (1998) noted that emission rates of total volatile organic compounds (TVOCs) increased with air temperature for both paint and varnish. However, the individual compounds did not necessarily follow the same trend established by the TVOC; they showed greater emission rates at lower air temperatures. The effects of relative humidity on the emissions of TVOC differed between paint and varnish. Individual compounds showed higher emission rates for lower levels of humidity and vice versa. The VOC emission characteristics of these materials are essential for understanding indoor air pollution dynamics (Jiang et al. 2017). Jiang et al. (2017) investigated the emission characteristics of VOCs from particleboard in sealed or ventilated environmental chambers at different temperatures (23, 35, or 50 °C), with a focus on the emission of odorous compounds. The emissions of HCHO and total VOCs (TVOC) from the particleboard increased significantly with temperature, and the emitted VOC mixtures had complex chemical compositions. At room temperature (23 °C), n-hexane was the most abundant compound, except HCHO; but at higher temperatures, concentrations of hexanal and pentanal significantly increased. Moreover, due to their low odour thresholds, aldehydes , particularly hexanal and pentanal, were identified as the major odorous compounds emitted from the particleboard.
In addition to air temperature and relative humidity, VOC emissions are influenced by surface temperatures . Kim et al. (2012) measured VOC emissions from building materials in residential buildings in Korea with radiant floor heating systems. The results showed that the VOC emissions from flooring materials increased as the floor temperature rises. In particular, increased temperatures may accelerate chemical reactions within the material, leading to additional VOC emissions (Kim et al. 2012). Emitted pollutants can be adsorbed onto indoor surfaces (carpet, wood, skin) and re-emit in indoor air (Xu et al. 2009) or they may react with each other and form secondary pollutants.
High relative humidity in combination with room temperatures often results in dampness and odours . Dampness -related problems (i.e., mould spots, damp stains, water damage and condensation) are risk factors for the perceptions of odours and sensations of humid air and dry air, as proven by Wang et al. (2013), in domestic environments in Chongqing, China and Ƶhang et al. (2012) in workplace buildings in Uppsala, Sweden.
The type of building ventilation system (i.e., natural-ventilation vs. mechanical systems) was related to IAQ and SBS as it was presented in the comparative study by Costa and Brickus (2000) in Niteroi, Rio de Janeiro, Brazil. Occupants in naturally ventilated offices have fewer SBS symptoms than occupants of air-conditioned offices (Costa and Brickus 2000, Seppänen and Fisk 2002). The importance of effective household ventilation via window opening frequency in the prevention of the negative effects of home dampness exposure on common cold was highlighted in the study by Sun et al. (2017). A cross-sectional survey on home environment and childhood health collected 13,335 parent-reported questionnaires of 4–6-year-old children in Shanghai, China. The results revealed that dampness-related exposures and household ventilation habits (p-value for interaction <0.001) had a strong interaction effect on the incidence and duration of the common cold.
In a field experiment by Shan et al. (2016), two identical tutorial rooms were studied to compare human subjects’ thermal comfort , SBS , and short-term performance under mixing ventilation and passive displacement ventilation. Higher CO2 concentration was the main factor causing SBS related to the head, while both higher CO2 concentration and lower relative humidity contributed to SBS related to the eyes. As a consequence, SBS resulted from high CO2 concentration and low relative humidity could lead to decrease in short-term performance. Mixing ventilation leads to higher overall draft sensation while displacement ventilation results in the sensation of cold feet.
Inadequately functioning, obsolete, and poorly maintained HVAC systems , decreased number of air changes, and decreased volumes of clean air may lead to increased concentrations of indoor air pollutants and may result in the occurrence of SBS symptoms (ECA 1989; Redlich et al. 1997; Assimakopoulos and Helmis 2004; Seppänen et al. 1999). Moreover, ventilation rates strongly influence the emission rates from indoor sources, such as DEHP emission rates from PVC flooring. Similar findings were reported in a study by Hodgson (2000) in houses in Florida, where VOCs emission rates at the low and high ventilation rates decreased with decreasing compound volatility. Additionally, the ventilation system itself can be a source of air pollutants. Unsealed fibreglass and other insulation material lining the ventilation ducts can release particulate material into the air. Such material can also become wet, creating an ideal and often concealed site for the growth of microorganisms (Redlich et al. 1997). Azuma et al. (2017) studied the correlation between indoor pollutants and building-related symptoms on office workers (N = 107 workers during winter, 207 workers during summer) in 17 buildings with air-conditioning systems in Tokyo, Osaka, and Fukuoka. Results revealed that upper respiratory symptoms showed a significant correlation with increased indoor temperatures and increased indoor concentrations of suspended particles released from the ambient air pollution via air-conditioning systems during winter.
Construction products can affect the transport and removal of indoor VOCs by sorption and desorption. Zhu et al. (2013) developed an integrated model capable of predicting the emission/sorption of VOCs from/on building materials under variable air exchange rates. Construction products can act as sinks or sources of VOCs emission.
4.2.4 Chemical-Biological Interactions
Chemical-biological interactions are interactive influences among parameters of the group of chemical risk factors and parameters of the group of biological risk factors (i.e., moulds, bacteria, MVOCs, house dust ).
Household dust serves as a good proxy for assessing indoor air pollution (Gustafsson et al. 2018). A characterization of residential house-dust by Gustafsson et al. (2018) showed that the respirable fraction of dust contains aluminium and zinc as dominating metals, silicon dioxide and calcium carbonate as the major mineral components, and bacterial, fungi and skin fragments in an organic matrix.
House dust often contains substances that are emitted from construction products, i.e., phthalate esters and other plasticisers emitted from PVC products (Kishi et al. 2012; Bamai et al. 2014), brominated flame retardants (Kajiwara and Takigami 2016), etc. Bamai et al. (2016) estimated phthalate intake from urinary metabolite among Japanese children and house dust levels in living environment. The results suggested that, among Japanese children, house dust from low surfaces, such as living room floors, might play a meaningful role in the indoor environmental exposure pathway for BBzP and DEHP. Phthalate intake via dust ingestion seems more strongly related to health than total intake.
Polybrominated diphenyl ethers (PBDEs) and hexabromocyclododecanes (HBCDs) are widely used as synthetic additives to reduce the flammability of plastics, textile coatings, and electronic appliances (Kajiwara and Takigami 2016). Although the use of PBDEs and HBCDs has been phased out as per international regulations, they still contribute greatly to the overall emissions. Kajiwara and Takigami (2016) examined the concentrations, profiles, and mass distributions of polybrominated diphenyl ethers (PBDEs), hexabromocyclododecanes (HBCDs), and polybrominated dibenzo-p-dioxins/furans (PBDD/Fs) based on the particle sizes of house dust samples from five homes in Japan. PBDEs, HBCDs, and PBDFs were detected in all the samples analysed.
A direct or indirect relation between damp or mould in the home and respiratory health were examined by Peat et al. (1998). Home dampness is thought to have health consequences because it has the potential to increase the proliferation of house-dust mites and moulds, both of which are allergens .
4.2.5 Biological-Biological Interactions
In the 1980s, in addition to physical risk factors, a number of studies examined biological risk factors, specifically the association between the presence of many biological agents in the indoor environment and dampness-related problems (mould spots, damp stains, water damage, and condensation) as well as inadequate ventilation. Studies on the exposure to other biological risk factors and SBS occurrence are scarce at present, mainly due to the fact that SBS but also BRI presents a common result of exposure to biological agents (i.e., aspergillosis).
Biological-biological interactions are interactive influences among parameters of the group of biological risk factors (Table 4.3).
The major sources of micro-organisms in indoor environment areas are humans, pets, room plants, waste, house dust , textiles, carpets, furniture fillers, and air filters for HVAC systems that are not properly maintained or not replaced in time (Yassin and Almouqatea 2010).
The association between MVOCs, dampness, and mould was reported in the study by Assimakopoulos and Helmis (2004) on a public building in the centre of Athens and in the study by Sahlberg et al. (2013) in 159 homes in Reykjavik, Uppsala and Tartu. Opposite findings were found in a study by Wieslander et al. (2007) on health effects in office workers (N = 18) in a medical casebook archive with dampness caused by flooding. The measurements of moulds and microbial volatile organic compounds could not identify any obvious exposure contrast between the damp building and the dry control building. The flooded building had slightly higher levels of MVOC . However, subjects previously exposed to building dampness had an increase of symptoms.
Examination of MVOCs in indoor air has also become an important method for the detection of the type and intensity of masked contamination by moulds (Fiedler et al. 2001; Choi et al. 2017).
4.2.6 Biological-Physical Interactions
Detected biological-physical interactions are interactive influences among parameters of the group of biological risk factors and parameters of the group of physical risk factors.
High relative air humidity in combination with air temperature may lead to the occurrence of condensation on surfaces, material damage, dampness, and toxic mould growth (ECA, 1989).
Moisture and temperature are the two key environmental parameters that determine the possibility of mould growth on construction complexes (Sautour et al. 2002). At relative humidity at or above 75–80% (0.75–0.8 water activity, water available in the material for microbial growth,), there is a possible risk of mould growth on construction products (Grant et al. 1989; Johansson et al. 2013). Relative humidity is affected by temperature, as temperature is reduced below 5 or increased above 35 °C (Zak and Wildman 2004), cellular processes are slowed down. In addition to air temperature and relative humidity, the type of material and its specific critical moisture level are important influential factors. If this is exceeded, there is a risk that mould fungi will develop on the material.
In indoor active spaces, the temperature and relative humidity often fluctuate due to seasonal variations, user activities, etc. The effect of cyclic moisture and temperature on mould growth on wood compared to steady-state conditions was studied by Johansson et al. (2013). The authors proved that the duration of favourable conditions of relative humidity was decisive for mould growth and fluctuating temperature lead to slower mould growth. Additionally, the impact of moisture content in construction products on mould growth is presented in more detail in Sect. 4.4.
In a study by Lappalainen et al. (2015), VOC emissions from hidden mould growth were investigated using an IAQ simulator test. MVOCs can be released from a moisture-damaged wall structure into an indoor environment, and the impact of the relative humidity of the material is remarkable. The concentration of MVOC is also related to absolute humidity and ventilation efficiency. A case-control investigation (198 cases and 202 controls) showed that homes with a high concentration of the MVOC were not only associated with a high absolute humidity but were also poorly ventilated. Specifically, joint exposure to high MVOCs and high absolute humidity was associated with 2.6-times greater odds of the doctor-diagnosed childhood asthma (95% CI , 0.7–8.91; P = 0.137).
Additionally, mites as important biological agents are related to a room’s relative humidity. They can be destroyed by keeping absolute humidity below 7 g/kg of air (about 45%) during the winter time (ECA 1989). If relative humidity is too low, which usually happens during the heating season, humidifiers are introduced. Humidifiers provide an optimal place for microbes to flourish. In addition to humidifiers, dehumidifiers, cooling devices, indoor A/C units are problematic for the growth of microorganisms (ECA 1989).
Salimifard et al. (2017) investigated the impacts of humidity and air swirl on the resuspension of biological particles (i.e., quartz, dust mite, cat fur, dog fur, and bacterial spore-Bacillus thuringiensis as an anthrax simulant) from floor and duct surfaces. The results showed that the particle property of being hydrophilic or hydrophobic plays an important role in the particle resuspension rate. The resuspension rates of hydrophilic dust mite particles increase up to two orders of magnitude as relative humidity decreased from 80 to 10% at 25 °C. However, the resuspension rates of cat fur and dog fur particles that are hydrophobic are within the measurement error range (±15%) over 10–80% relative humidity. With regard to the resuspension of bacterial spores (Bacillus thuringiensis) from a duct surface, the resuspension rates are substantially affected by air swirl velocity and particle size (Salimifard et al. 2017).
Human-made water systems (e.g., hot water systems, ventilation systems, cooling towers, humidifiers, whirlpool spas) are common sources of outbreaks of Legionella infection (NIPH 2012). Transmission can also occur in public and residential buildings . Incidence of the disease is higher in the summertime, possibly because of increased use of cooling towers for air conditioning systems and differences in water chemistry when outdoor temperatures are higher (Prussin et al. 2017).
Major indoor environmental factors , such as relative humidity, characteristics of air ventilation systems, seasonal variation, temperature, and chemical composition of the air influencing bioaerosol concentration (Law et al. 2001; Park et al. 2001). Studies proved (Law et al. 2001; Park et al. 2001) that concentrations of endotoxin and airborne fungi were positively related to indoor relative humidity (higher concentration associated with higher relative humidity). Relative humidity also affects the infectivity of airborne viruses (Verreault et al. 2008).
4.2.7 Personal-Physical Interactions
In the 1990s, researchers realized that SBS was influenced also by psychosocial, personal, and other risk factors . Nevertheless, psychosocial, personal and other risk factors remain neglected research areas.
Detected physical-personal interactions are interactive influences among parameters of the group of physical risk factors and parameters of the group personal risk factors (gender , health status , individual differences).
A literature survey on how different factors influence human comfort in indoor environments (Frontczak and Wargocki 2011) showed that thermal comfort was influenced by the level of education, the relationship with superiors and colleagues and time pressure, but not by gender , age , body build, fitness, health, self-estimated environmental sensitivity, menstruation cycle, pattern of smoking and coffee drinking, job stress or hours worked per week. Additionally, the impact of individuality on thermal sensation was presented in greater detail in Chaps. 1 and 2.
Social status is a significant health determinant related to built environments . Several studies (Metin Özcan et al. 2013; Yun and Steemers 2011; Santamouris et al. 2007) evaluated the association between social status and indoor environmental quality issues. The considered socio-economic indicator in these studies was fuel poverty.
BOX 4.1 Fuel poverty
A person is to be regarded as living “in fuel poverty” if he is a member of a household living on a lower income in a home that cannot be kept warm at a reasonable cost (WHECA 2000). A frequently used definition is that when a household needs to spend more than 10% of its income to keep its dwelling adequately warm and for other energy services, it is fuel poor (Boardmann 1991).
Fuel poverty is measured by:
-
inability to keep homes adequately warm,
-
arrears on utility bills,
-
people living in a dwelling with a leaking roof, damp walls, floors or foundation (Kontonasiou et al. 2015).
Between 50 and 125 million people in the EU are estimated to suffer from fuel poverty (WHO 2012). The number will inevitably rise in the future as global energy prices increase (EPEE 2017). The data from the Assessment report on environmental health inequalities in Europe (WHO 2012) provide strong evidence that the non-sanitary housing inequalities—overcrowding, dampness and thermal comfort related to cool and warm homes—exist in almost every country. Similar results were found in a Pan-European study (Velux 2016; Velux Group 2017), Europeans who live in energy poverty are almost three times as likely to live in damp, unhealthy buildings.
Low-income populations, and especially low-income single-parent households and the elderly are the most affected across all indicators.
Fuel poverty is strongly related to ability to keep a home comfortably warm in winter and comfortably cool in summer (WHO 2012; BPIE 2014). Forty-five percent of the studied European population reduce their temperatures to lower their energy bills (Velux 2016). In addition to winter, summer indoor air temperatures may be a problem. The proportion of the general population unable to keep their dwellings comfortably cool in summer is even higher than the proportion unable to keep the home warm in winter (WHO 2012).
The increasing trend of fuel poverty is related to indoor environmental quality issues. In 2012, 12.9% of the EU-28 population declared that their dwelling was not comfortably warm during winter, and almost 20.0% of Europeans perceived their dwellings to be not sufficiently insulated against excessive heat during summer (Eurostat 2017).
The environmental health inequalities in relation to built environment issues represent critical research areas on the global and national scales. Findings on the association between socio-economic indicators and indoor environmental quality are beneficial especially in defining national laws on housing and social policies as well as defining priority actions to ensure their effective implementation throughout the country.
For example, in 2015, households in Slovenia spent on average 6.7% of their disposable income on electricity, gas and other fuels, which is 0.7 of a percentage point less than in 2012 (latest available data) and the same as in 2000. Having reviewed the distribution of households by income quintiles, we found that expenditure for electricity, gas and other fuels in 2015 in the first quintile (representing 20% of households with the lowest income) represented on average 17.7%. Fuel poverty indicators among people at risk of poverty in Slovenia are: 37.5% arrears on utility bills (10% EU average), 17.3% inability to keep home adequately warm (10.8% EU average) and 46.1% dwellings with leakages & damp walls (15.1% EU average) (Kontonasiou et al. 2015). Socio-economic status is related to indoor environmental quality issues. The results of the online pilot survey in Slovenia on 714 respondents (Recek 2017; Recek et al. 2019) showed that households with a better socio-economic status spend more household income for a better living comfort and consequently stay in facilities with better indoor environmental quality. Such environmental quality is also detected in buildings with higher energy efficiency . Based on the results of the online survey, the socio-economic status of a household does not influence the energy efficiency of a building. The main reason for the investment in increased energy efficiency of buildings is lower energy consumption for heating, to which respondents give priority over indoor environmental quality (Recek 2017; Recek et al. 2019).
4.2.8 Personal-Chemical Interactions
The most important findings of the literature review show that many studies have examined the correlation between SBS symptoms and physical risk factors as well as the correlation between SBS symptoms and chemical risk factors, while the evidence on the correlation between SBS symptoms and biological, psychological, personal and other risk factors is for the moment scarce.
Detected personal-chemical interactions are interactive influences among parameters of the group of personal risk factors and parameters of the group of chemical risk factors.
Many studies have focused on the adverse health effects of indoor air pollutants among highly sensitive groups of individuals, such as children , the elderly , and occupational groups (Heudorf et al. 2007; Jaakkola et al. 1999).
Numerous epidemiological studies have shown associations between air pollution and reduced lung function and increased prevalence of respiratory diseases among children and young adults (Sierra-Vargas and Teran 2012). Current epidemiological studies that explore the impact of indoor air quality on respiratory diseases are mostly limited to estimations of prevalence or incidence observed in a particular age group (Eder et al. 2006). Due to their physiological characteristics, children are vulnerable in relation to environmental impact, as they inhale more air than adults do and, therefore, their exposure is greater. Toxic substances may disrupt or interfere with the rapid development of various body functions, which can lead to irreversible diseases and organ damage. Indoor pollutants can cause or aggravate various medical conditions such as allergies, asthma, and other respiratory diseases. Thus, a healthy school environment is crucial in protecting the health of children since they spend up to eight hours per day and nine months per year in the school premises (WHO 2004). The number of studies exploring the association between respiratory diseases and indoor air quality is increasing although the number of studies in educational institutions remains relatively low, as most epidemiological research focuses on indoor air at home. One indicator of respiratory disease is reduced lung function, which can be measured with spirometry. In this procedure, the volume and rate of exhaled air is measured, from which the state of illness in the respiratory tract may be inferred (Kaminsky 2012). Asthma is the most common childhood disease in developed countries with a statistically significant morbidity and increasing prevalence (Eder et al. 2006). Typical symptoms are bronchial hyper-responsiveness, chronic inflammation of the airways, and recurrent wheezing (Weichenthal et al. 2007). The identification of air pollutants that are causally associated with the development of asthma is extremely difficult due to the complex combination of pollutants and etiological heterogeneity of asthma (Delfino 2002).
The positive correlation between oxidative stress, indoor air pollution (VOC, CO2 ), and SBS complaints was proved in the study by Lu et al. (2007) among 389 office workers in 87 government offices of eight high-rise buildings in Taipei, Taiwan.
4.2.9 Interactions Between Other Health Risk Factors and Their Parameters
The strong relationship between ownership and building age was proved by Engvall et al. (2000) in Stockholm, 609 multi-family buildings with 14,235 dwellings . Subjects owning their own building reported less SBS , but 5% of all buildings built before 1961, 13% of those built in 1976-1984, and 15% of those built in 1985–1990 would have significantly more SBS than expected. Mizoue et al. (2001) examined these relations using data from a 1998 cross-sectional survey of 1,281 municipal employees who worked in a variety of buildings in a Japanese city. Working overtime for 30 or more hours per month was also associated with SBS symptoms. Personal lifestyles are an additional factor.
The association between personal and psychosocial factors was confirmed in the study by Ooi and Goh (1997). The authors found an incremental trend in prevalence of SBS among office workers who reported high levels of physical and mental stress and decreasing climate of co-operation. Similar findings were reported in the study by Burge (2004), where SBS symptoms were generally more common and more problematic in the stressed, the unloved, and in individuals who feel powerless to change their situation (Burge 2004). Another important issue is related to possibility of individual regulation and control of indoor environmental parameters. Poor individual control of temperature and lighting are associated with increased symptoms (Jaakkola et al. 1989). The study by Burge (2004) proved a strong association between lack of control of the office environment and symptoms. Two quantitative studies (Temeljotov Salaj et al. 2015; Baričič et al. 2014) on 1,036 office workers in Slovenia and 394 office workers in Lebanon showed that real-estate factors of the workspace—in terms of the assessment of office building and the position of the employee, as well as the workspace design —have an impact on the satisfaction of employees and, consequently, their assessment of health.
4.3 Multi-group Interactions
Detected multifactorial interactions are interactive influences among parameters of different groups of risk factors. Many studies have analysed the association between various risk factors for SBS .
The effect of physical, chemical and personal health risk factors and their parameters were analysed by Burge (2004). Burge (2004) found out that there was an association between increasing air temperature , overcrowding, and inadequate ventilation and the occurrence of SBS . Household formaldehyde exposure and its associations with dwelling characteristics, lifestyle behaviours, and childhood health outcomes in Shanghai, China was studied by Huang et al. (2017). Examining 409 children ’s bedrooms, the authors determined that bedrooms with mechanical ventilation had lower formaldehyde concentrations than those with natural ventilation. Results indicated that household formaldehyde exposure may increase the risk of the common cold in childhood. Household formaldehyde had few significant associations with the studied illnesses. Families with sick children perhaps pay more attention to improving indoor air quality .
The effect of physical, chemical and microbiological characteristics of 19 governmental office buildings in the Netherlands and SBS were analysed by Teeuw et al. (1994). Moreover, Skov et al. (1990) performed a multivariate logistic regression analyses on 2,369 office workers in 14 buildings in Copenhagen, Denmark, in which the influence of various factors, such as the concentration of macromolecular organic floor dust, the floor covering, the number of workplaces in the office, the age of the building, the type of ventilation, shelf factor and fleece factor on SBS symptoms was investigated.
The effect of physical, chemical, biological and personal factors was also evaluated in residential buildings. Lu et al. (2016) studied associations between outdoor air pollution, meteorological parameters, and selected indoor exposure and building characteristics at home and weekly SBS symptoms in a standardized questionnaire study among 3,485 randomly selected adults in China. Indoor factors played a major role in SBS symptoms. Mould/dampness on the floor/ceiling was associated with fatigue OR = 1.60 (1.11–2.30) and headache OR = 1.80 (1.07–3.04). Mouldy odour was associated with fatigue OR = 1.59 (1.07–2.37) and dermal symptoms OR = 1.91 (1.21–3.02). Windowpane condensation in winter was associated with fatigue OR = 1.73 (1.30–2.31) and throat symptoms OR = 1.53 (1.01–2.31). Damp bed clothing was related with throat symptom OR = 1.62 (1.09–2.40). Home redecoration was associated with fatigue OR = 1.49 (1.07–2.06). Frequent window opening was associated with less nose symptoms OR = 0.54 (0.36–0.82), and mechanical ventilation in the bathroom reduced dermal symptoms OR = 0.66 (0.44–0.99). Females were more susceptible to redecoration and windowpane condensation than men were. No associations with SBS were observed for outdoor air pollutants or meteorological parameters in the final models combining indoor and outdoor factors, although SO2, temperature, and relative humidity were associated with some SBS symptoms (fatigue, eyes and nose symptoms) in the separate outdoor models. In conclusion, indoor mould/dampness, air pollution from redecoration, and poorer ventilation conditions in dwellings can be risk factors for SBS symptoms in an adult Chinese population, especially among females (Lu et al. 2016).
The effect of personal , physical, and biological factors was also statistically evaluated on a larger scale. The EU SILC survey (Ecofys 2017) on 100,000 individual households and more than 250,000 adults (16 years and older) proved statistically very significant correlations among socio-economic indicators, state of building, and health issues. Around 33% of adults (16.2 million) report dampness when being unable to keep their dwelling warm, but only 12% when being able to do so. The probability that adults report dampness is 2.8 times higher when they are unable to keep their dwelling warm. In multi-family buildings, this probability is around 2.5 times higher, and in single-family buildings, this probability is approximately three times higher in comparison to when there are no difficulties. A share of 13% of adults (6.4 million) report lack of daylight when being unable to keep their dwelling warm, but only 6% when being able to do so; 20% of adults (10 million) report poor health when being unable to keep their dwelling warm, but only 9% when being able to do so.
Several studies make the same conclusions that it is difficult to pinpoint the causative factor for SBS due to multifactorial effects. In a study of an air-conditioned building in Niteroi, Rio de Janeiro, Brazil, Costa and Brickus (2000) concluded that poor individual control of temperature and lighting are associated with increased symptoms. A univariate analysis, performed by Abdel-Hamid et al. (2013) at the Faculty of Medicine, Ain Shams University, Cairo, Egypt showed that poor lighting, poor ventilation, lack of sunlight, absence of air currents, high noise , temperature, humidity, environmental tobacco smoke , use of photocopiers, and inadequate office cleaning were statistically associated with SBS symptoms. Building characteristics , such as year of construction and the effect of indoor emissions lead to SBS. New houses and new furniture result in higher emissions (Takigawa et al. 2012).
4.4 Decision-Making Tool in the Design of Built Environments
The identification of risk factors and their parameters is a crucial step for effective prevention and control of health outcomes in the built environments . Additionally, it is important to detect all interactive influences among factors and their parameters. Detected interactive influences among parameters are problematic fields that have to be eliminated or minimized.
BOX 4.2 Problematic field
A problematic field represents a main focus point in the decision-making process . Specifically, it includes:
-
single or multi-group interactions between parameters in built environment,
-
exposure time ,
-
exposure population, especially vulnerable population groups .
For every problematic field, causes and consequences are defined, which serve as a basis for the development of effective measures, accompanied by step-by-step activities to be used in the decision-making process in the design of built environments (Fig. 4.1).

General decision-making process in built environment
BOX 4.3 Decision-making in the design of built environments
Decision making is the process of identifying the likely consequences of decisions, establishing the importance of single and multi-group interactions between health risk factors, to select the best course of action, to protect user’s health in built environment. It should be included in all steps of building design .
Following the evidence-based design approach, the total of 527 sources of literature (Table 4.4) were analysed and presented in previous chapters. As a synthesis, a tool for decision-making process is developed.
BOX 4.4 Evidence-based design approach
The Center for Health Design (CHD) defines evidence-based design approach as “the deliberate attempt to base building decisions on the best available research evidence with the goal of improving outcomes and of continuing to monitor the success or failure for subsequent decision-making.” An evidence-based model can be used for all design decisions (Malkin 2008).
The tool is shaped in the form of a matrix, a rectangular array of numbers, symbols, or expressions, arranged in rows and columns. According to our primary goal, to design a healthy built environment with mastered health risk factors and their parameters, altogether six groups of health risk factors and 23 parameters are arranged in rows and columns (Fig. 4.2). Interactive influences among parameters are marked separately in at the crossing points between rows and columns, positioned in the middle of the matrix. For example, cell 9-1 presents the detected interactive influence between physical and chemical health hazard factors, specifically air temperature and formaldehyde emissions from materials (described more in detail in Sect. 4.2).

Abbreviations: VOCs-volatile organic compounds , ETS-environmental tobacco smoke , MMMF - man-made mineral fibre, Tai-air temperature , Tsurf-surface temperature, RHai-relative humidity of indoor air, EM-electromagnetic fields, MVOC - microbes’ volatile organic compounds
Designed tool for decision-making process in the design of built environments
A detected interactive influence represents a potential problem field that has to be eliminated or minimized. For every marked cell, step-by-step activities for effective prevention and control of health risk factors and their parameters have to be defined. Planned activities should be considered for all possible influences of other factors and parameters (i.e., positive or negative). In such a way, the matrix enables doing that and can be used as a tool for the decision-making process . It enables further upgrading according to new research findings.
BOX 4.5 Decision-making process in the design of built environments: case study
Step 1: Definition of the main problem, identifying hazards:
-
Problem: appearance of mould (Fig. 4.3)
Fig. 4.3 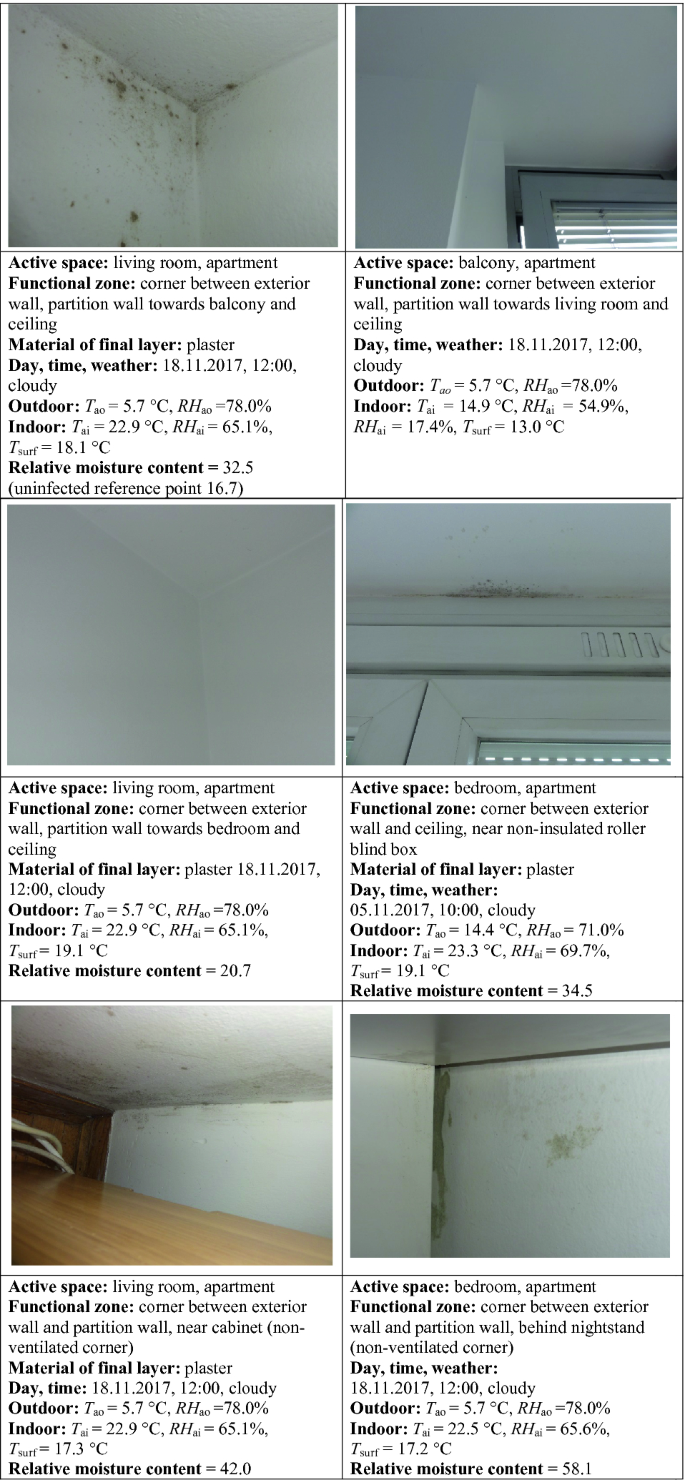
Abbreviations: Tao = outdoor air temperature (°C), RHao = relative air humidity of outdoor air (%), Tai = indoor air temperature (°C), RHai = relative humidity of indoor air (%), Tsurf = surface temperature of final layer (°C), relative moisture content measured on final layer
Identified mouldy active spaces, functional zones, material and measured environmental parameters.
-
Built environment : single room apartment, NE-oriented
-
Infected active space: living room, bedroom
-
Exposure population: 3 occupants
-
Exposure time: 2 years, without noticeable health outcomes
-
Duration : whole year, increase growth in October-March (temperate climate )
-
Indicator: mould spots, draught environment
-
Position, infected materials: final layers of constructional complexes, plaster; corners, behind furniture

Step 2. List of detected causes (building, system, user):
-
Building: improper design of building envelope, inadequate composition of construction complexes (e.g., inadequate damp proof membrane, vapour barrier, thermal insulation, etc.), defects on intersections, geometric thermal bridges and construction thermal bridges (allows higher heat transfer than the surrounding thermal envelope), etc.
-
system: inadequate ventilation, improper design of building envelope and system
-
occupants’ habits (cooking, indoor laundry drying)
-
furniture position
-
other possible causes are not present: irregularities in plumbing system, floods, etc.
Step 3. Definition of measures and step-by-step activities:
-
specific goal: elimination of irregularities in construction complexes, systems, environment
-
methods: measures of surface temperatures , material moisture content, indoor and outdoor environmental parameters; simulations of heat and moisture transfer before and after renovated construction complexes; characterization of mould species, concentration in air in special cases
-
elimination of geometric and construction heat bridges with additional thermal insulation (upper part of the window, corner, etc.), installation of vapour barriers
-
improved ventilation system in kitchen and bathroom
-
elimination of irregularities in heating system
-
education and training of all occupants (increased natural ventilation of all apartment, sock ventilation, drying laundry outdoors or in drying machine, use of ventilation devices in kitchen and bathroom etc.), increased distance between furniture position and wall
Step 4. Hazard calculation, comprehensive approach:
-
interaction between parameters: definition of the consequences on other physical, chemical, biological health risk factors and their parameters: 1–17, 2–17, 3–17, 8–17, 12–17, 15–17, 17–17, 18–17, 19–17, 20–17
-
optimal air temperature and relative air humidity levels according to user comfort and draught elimination
Step 5. Realization, efficiency evaluation:
-
elimination of mould
-
periodic monitoring of built environment, conditions and activities
With usage of the designed tool for decision-making process , similar activities, as it presented for mould (Fig. 4.3), can be performed for every detected problem in built environments (i.e., poor indoor air quality , thermal discomfort, etc.). Finally, the designed strategy includes holistic actions at the level of physical, chemical, biological, psychosocial, personal and other groups of risk factors and their interactive influences.
4.5 Short-Term and Long-Term Benefits of Holistic Design
It is expected that the implementation of design strategy will result in healthy and comfortable conditions , as well as increased productivity and decreased health costs with economic benefits. Moreover, such a holistic design of healthy built environments results in achieving overall efficiency of buildings, new or renovated ones. Construction or renovation leading to a healthy building results in minimized adverse health outcomes . This encourages a higher renovation rate that will bring large-scale benefits to individuals and society alike.
In addition to health, the environment, and the economy, the holistic design of healthy built environment renovations has several benefits (European Parliament 2016):
-
Environmental benefits : greenhouse gas emissions reduction, reduced usage of materials, energy savings,
-
Economic benefits: employment, GDP and public budgets, innovation, sectoral modernization, energy security, energy bill savings, increase in property value, tenant satisfaction,
-
Health benefits : reduction of energy poverty, productivity benefits, wellbeing , comfort benefits.
Up to today, many cost-benefit studies were performed to assess the financial benefits of performed activities for improving the quality of built environments . The potential financial benefits of improving indoor environments exceed costs by factors of 9 and 14 (Fisk 1999). For the US, Fisk and Rosenfeld (1997) estimated that potential annual savings and productivity gains ranged from $6 to $19 billion from reduced respiratory disease; $1–$4 billion from reduced allergies and asthma, $10–$20 billion from reduced symptoms of SBS , and $12–$125 billion from direct improvements in worker performance unrelated to health. Similar findings were recorded in the studies by Dutton et al. (2013) and Wargocki (2013).
BOX 4.6 Cost-benefit analysis (CBA)
Cost-benefit analysis (CBA) offers a method of economic evaluation that values all benefits against all costs. The resulting cost-benefit ratio indicates whether or not the benefits outweigh the costs of an intervention and hence provides a decision-making tool with a broad societal perspective (WHO 2017).
Dutton et al. (2013) assessed the impact of a natural ventilation retrofit of 10% of California’s office stock on the prevalence of SBS symptoms and associated costs; doing so would result in 22,000–56,000 fewer people reporting symptoms in a given week. Wargocki (2013) showed that crude estimates suggest that 2 million healthy life years can be saved in Europe by avoiding exposure to indoor air pollutants in non-industrial buildings. Healthy indoor air quality at work can increase people’s productivity up to 10% (Wyon and Wargocki 2013). Similar estimates have been made for the U.S. as regards exposures to air pollutants in residential buildings. The potential annual savings and productivity gains have been estimated to be as high as $168 billion in the U.S. (1997 estimate as no newer data are available). A saving of $400 per employee per year (2000 estimate) was estimated due to reduced absenteeism being the result of improved indoor air quality. In Europe, the annual productivity benefits were estimated to be at the level of about €330 per worker (2000 estimate as no newer data are available) (Wargocki 2013). Recent studies have shown that costs of poor indoor environment for the employer, the building owner, and for society as a whole are often considerably higher than the cost of the energy used in the same building (EN 15251:2007).
Similar findings were made by:
Selkowitz, Energy Technologies Area (ETA), Lawrence Berkeley National Laboratory cautioned: “Very generally, if you look at costs in very round numbers, energy costs about $2 per square foot per year, and people cost about $200 per square foot” in an office building. So even a tiny improvement in productivity or sick time will pay off far more quickly than energy savings, he said (Washington Post 1999).
Temeljotov Salaj et al. (2017) highlighted the negative impacts of economic crises: “Economic crisis has impacts on workplace conditions, affects the satisfaction of employees and consequently occupational health. Implementing aspects of better workplace conditions introduces a better base of value for employees and employers”, they concluded (Temeljotov Salaj et al. 2017, p. 2088).
In conclusion, well-designed buildings are those which are fit for their purpose (Lavin et al. 2006). Healthy buildings are more than that (Fig. 4.4).

Concept of healthy built environments
The presented concept of healthy built environments with a design strategy is necessary for the future planning of healthy and comfortable buildings and is a basis for successful renovations. For this reason, it is essential to understand all benefits of such holistic approach as well as negative side-effects of current unilateral design that is currently in progress. Therefore, it is necessary to implement the strategy at the first step of design, at the planning stage.
Readers of this book acquire comprehensive knowledge and clear understanding of the health risk factors and their influences from various disciplines. In this way, it promotes multidisciplinary cooperation between various fields that is necessary for efficient control and prevention against negative health outcomes in built environments .
All of us have responsibility to place human, as an individual and his values, in the front of design (Krašovec 2019).
References
Abdel-Hamid, M., Hakim, A. S., Elokda, E. E., & Mostafa, N. S. (2013). Prevalence and risk factors of sick building syndrome among office workers. Journal of the Egyptian Public Health Association, 88, 109–114. https://doi.org/10.1097/01.EPX.0000431629.28378.c0.
Assimakopoulos, V. D., & Helmis, C. G. (2004). On the study of a sick building: The case of Athens Air Traffic Control Tower. Energy and Buildings, 36, 15–22. https://doi.org/10.1016/S0378-7788(03)00043-4.
Azuma, K., Ikeda, K., Kagi, N., Yanagi, U., & Osawa, H. (2017). Physicochemical risk factors for building-related symptoms in air-conditioned office buildings: Ambient particles and combined exposure to indoor air pollutants. Science of the Total Environment 616–617:1649–1655. https://www.ncbi.nlm.nih.gov/pubmed/29070452. Retrieved December 3, 2018, from https://doi.org/10.1016/j.scitotenv.2017.10.147.
Bamai, Y. A., Araki, B. A., Kawai, T., Tsuboi, T., Saito, I., Yoshioka, E., et al. (2014). Associations of phthalate concentrations in floor dust and multi-surface dust with the interior materials in Japanese dwellings. Science of the Total Environment, 468–469, 147–157. https://doi.org/10.1016/j.scitotenv.2013.07.107.
Bamai, Y. A., Araki, A., Kawai, T., Tsuboi, T., Saito, I., Yoshioka, E., et al. (2016). Exposure to phthalates in house dust and associated allergies in children aged 6–12 years. Environment International, 96, 16–23. https://doi.org/10.1016/j.envint.2016.08.025.
Baričič, A., & Temeljotov Salaj, A. (2014). The impact of office workspace on the satisfaction of employees and their overall health - research presentation. SlovMedJour, 83(3), 217–231.
Bivolarova, M., Kierat, W., Zavrl, E., Popiolek, Z., & Melikov, A. (2017). Effect of airflow interaction in the breathing zone on exposure to bio-effluents. Building and Environment, 125, 216–226. https://doi.org/10.1016/j.buildenv.2017.08.043.
Blondel, A., & Plaisance, H. (2011). Screening of formaldehyde indoor sources and quantification of their emission using a passive sampler. Building and Environment, 46, 1284–1291. https://doi.org/10.1016/j.buildenv.2010.12.011.
Blount, B. C., Silva, M. J., Caudill, S. P., Needham, L. L., Pirkle, J. L., Sampson, E. J., et al. (2000). Levels of seven urinary phthalate metabolites in a human reference population. Environmental Health Perspectives, 108, 979–982. https://doi.org/10.1289/ehp.00108979.
Boardmann, B. (1991). Fuel poverty: From cold homes to affordable warmth. London: Belhaven Press.
Bornehag, C. G., Sundell, J., Weschler, C. J., Sigsgaard, T., Lundgren, B., Hasselgren, M., et al. (2004). The association between asthma and allergic symptoms in children and phthalates in house dust: a nested case–control study. Environmental Health Perspectives, 112, 1393–1397. https://doi.org/10.1289/ehp.7187.
BPIE. (2014). Buildings Performance Institute Europe. Alleviating fuel poverty in the EU investing in home renovation, a sustainable and inclusive solution. Retrieved November 9, 2018, from http://bpie.eu/wp-content/uploads/2015/10/Alleviating-fuel-poverty.pdf.
Burge, P. S. (2004). Sick building syndrome. Occupational and Environmental Medicine, 61, 185–190. https://doi.org/10.1136/oem.2003.008813.
Burt, T. (1996). Sick Building Syndrome: Acoustic Aspects. Indoor and Built Environment, 5(1), 44–59. http://smithvilleturbinesoppositionparty.ca/news/wp-content/uploads/2015/03/Indoor-and-Built-Environment-1996-Burt-44-59.pdf. Retrieved December 3, 2018, from http://dx.doi.org/10.1177/1420326X9600500107.
CDC. (2015). The National Institute for Occupational Safety and Health (NIOSH) Indoor Environmental Quality. Chemicals and Odors. Retrieved December 3, 2017, from https://www.cdc.gov/niosh/topics/indoorenv/chemicalsodors.html.
Chen, Z., Shi, J., Shen, X., Ma, Q., & Xu, B. (2016). Study on formaldehyde emissions from porous building material under non-isothermal conditions. Applied Thermal Engineering, 101, 165–172. https://doi.org/10.1016/j.applthermaleng.2016.02.134.
Choi, H., Schmidbauer, N., & Bornehag, C.-G. (2017). Volatile organic compounds of possible microbial origin and their risks on childhood asthma and allergies within damp homes. Environment International, 98, 143–151. https://doi.org/10.1016/j.envint.2016.10.028.
Clausen, P., Liu, Z., Kofoed-Sørensen, V., Little, J., & Wolkoff, P. (2012). Influence of temperature on the emission of di-(2-ethylhexyl) phthalate (DEHP) from PVC flooring in the emission cell FLEC. Environmental Science and Technology, 17(46), 909–915. https://doi.org/10.1021/es2035625.
Costa, M., & Brickus, L. (2000). Effects of ventilation systems on prevalence of symptoms associated with sick buildings in Brazilian commercial establishments. Archives of Environmental Health, 55, 279–283. https://doi.org/10.1080/00039890009603419.
Delfino, R. J. (2002). Epidemiologic evidence for asthma and exposure to air toxics: linkages between occupational, indoor, and community air pollution research. Environmental Health Perspectives, 110(4), 573–589. https://doi.org/10.1289/ehp.02110s4573.
Douwes, J., Thorne, P., Pearce, N., & Heederik, D. (2003). Bioaerosol health effects and exposure assessment: Progress and prospects. Annals of Occupational Hygiene, 47(3), 187–200. https://doi.org/10.1093/annhyg/meg032.
Dovjak, M., & Kristl, Ž. (2011). Health concerns of PVC materials in the built environment. International Journal Sanitary Engineering Research, 5, 4–26.
Dutton, S. M., Banks, D., Brunswick, S. L., & Fisk, W. J. (2013). Health and economic implications of natural ventilation in California offices. Building and Environment, 67, 34–45. https://doi.org/10.1016/j.buildenv.2013.05.002.
ECA. (1989). Indoor air quality & its impact on man. COST Project 613. Environment and Quality of Life Report No. 4. Sick Building Syndrome. A Practical Guide. In. Luxembourg.: Commission of the European Communities. Directorate General for Science. Research and Development. Joint Research Centre - Institute for the Environment. Commission of the European Communities, ECA.
Ecofys. (2017). The relation between quality of dwelling, socio-economic status and health in EU28 and its Member States. Scientific report as input for Healthy Homes, Barometer 2017, Hermelink A, Ashok J. Retrieved December 3, 2018, from http://www.ecofys.com/files/files/ecofys-2017-relation-between-quality-of-dwelling-and-health-final.pdf.
Eder, W., Ege, M. J., & von Mutius, E. (2006). The asthma epidemic. New England Journal of Medicine, 355, 2226–2235. https://doi.org/10.1056/NEJMra054308.
EN. (15251:2007). Indoor environmental input parameters for design and assessment of energy performance of buildings addressing indoor air quality, thermal environment, lighting and acoustics.
Engvall, K. (2000). Development of a multiple regression model to identify multi-family residential buildings with a high prevalence of sick building syndrome (SBS). Indoor Air, 10, 101–110. https://doi.org/10.1034/j.1600-0668.2000.010002101.x.
EPA. (2017). VOC. Retrieved December 3, 2018, from https://www.epa.gov/indoor-air-quality-iaq/volatile-organic-compounds-impact-indoor-air-quality.
EPEE. (2017). European fuel Poverty and Energy Efficiency (EPEE). Epee Project. Retrieved December 3, 2018, from https://ec.europa.eu/energy/intelligent/projects/en/projects/epee.
Eurostat. (2017). Housing conditions. Retrieved December 3, 2018, from http://ec.europa.eu/eurostat/statistics-explained/index.php/Housing_conditions.
European Parliament. (2016). Directorate general for internal policies policy department A: Economic and scientific policy. In I. Artola, K. Rademaekers, R. Williams, J. Yearwood (Eds.), Boosting building renovation: What potential and value for Europe? Retrieved December 3, 2018, from http://www.europarl.europa.eu/RegData/etudes/STUD/2016/587326/IPOL_STU(2016)587326_EN.pdf.
Fiedler, K., Schütz, E., Geh, S. (2001). Detection of microbial volatile organic compounds (MVOCs) produced by moulds on various materials. International Journal of Hygiene and Environmental Health, 204(2–3), 111–121. https://ac.els-cdn.com/S1438463904700826/1-s2.0-S1438463904700826-main.pdf?_tid=1b14e6dc-d4f9-11e7-a4e2-00000aab0f01&acdnat=1511955382_ed059f335714e49946d64694b22b87e3. Retrieved December 3, 2017, from. http://dx.doi.org/10.1078/1438-4639-00094.
Findeis, H., & Peters, E. (2004). Disturbing effects of low frequency sound immissions and vibrations in residential buildings. Noise Health, 6(23), 29–35. Retrieved December 3, 2017 from https://www.ncbi.nlm.nih.gov/pubmed/15273022.
Fisk, W. J. (1999). Estimates of potential nationwide productivity and health benefits from better indoor environments: An update. In: J. Spengler, J. Samet, & J. McCarthy (2001) Indoor air quality handbook McGraw Hill: McGraw-Hill Education. Retrieved December 3, 2018 from https://www.accessengineeringlibrary.com/browse/indoor-air-quality-handbook.
Fisk, W. J. & Rosenfeld, A. H. (1997). Estimates of improved productivity and health from better indoor environments. Indoor Air 7(3), 158–172. https://indoor.lbl.gov/publications/estimates-improved-productivity-and. Retrieved December 3, 2017 from http://dx.doi.org/10.1111/j.1600-0668.1997.t01-1-00002.x.
Frontczak, M., & Wargocki, P. (2011). Literature survey on how different factors influence human comfort in indoor environments. Building and Environment, 46, 922–937. https://doi.org/10.1016/j.buildenv.2010.10.021.
Gustafsson, Å., Krais, A. M., Gorzsás, A., Lundh, T., & Gerde, P. (2018) Isolation and characterization of a respirable particle fraction from residential house-dust. Environmental Research, 161, 284–290. http://www.sciencedirect.com/science/article/pii/S0013935117316717 Retrieved December 3, 2017 from http://dx.doi.org/10.1016/j.envres.2017.10.049.
Grant, C., Hunter, C. A., Flannigan, B., & Bravery, A. F. (1989). The moisture requirements of moulds isolated from domestic dwellings. International Biodeterioration, 25(4), 259–284. https://doi.org/10.1016/0265-3036(89)90002-X.
Haghighat, F., & De Bellis, L. (1998). Material emission rates: literature review, and the impact of indoor air temperature and relative humidity. Building and Environment, 33, 261–277. https://doi.org/10.1016/S0360-1323(97)00060-7.
Heudorf, U., Mersch-Sundermann, V., & Angerer, J. (2007). Phthalates: toxicology and exposure. International Journal of Hygiene and Environmental Health, 210, 623–634. https://doi.org/10.1016/j.ijheh.2007.07.011.
Hodgson, M., Permar, E., Squire, G., Allera, C. W., & Parkinson, D. K. (1987) Vibrations as a cause of “tight-building syndrome” symptoms. ibid, 2, 449–453.
Hodgson, A. T. (2000). Volatile organic compound concentrations and emission rates in new manufactured and site-built houses. Indoor Air, 10, 178–192. https://doi.org/10.1034/j.1600-0668.2000.010003178.x.
Huang, S., Xiong, J., & Zhang, Y. (2015). The impact of relative humidity on the emission behaviour of formaldehyde in building materials. Procedia Engineering, 121, 59–66. https://doi.org/10.1016/j.proeng.2015.08.1019.
Huang, C., Liu, W., Cai, J., Wang, X., Zou, Z., & Sun, C. (2017). Household formaldehyde exposure and its associations with dwelling characteristics, lifestyle behaviours, and childhood health outcomes in Shanghai, China. Building and Environment, 125, 143–152. https://doi.org/10.1016/j.buildenv.2017.08.042.
Jaakkola, J., Heinonen, O., & Seppänen, O. (1989). Sick building syndrome, sensation of dryness and thermal comfort in relation to room temperature in an office building: Need for individual control of temperature. Environment International 15, 163–168. Retrieved December 3, 2017 from http://dx.doi.org/10.1016/0160-4120(89)90022-6.
Jaakkola, J., Oie, L., Nafstad, P., Botten, G., Samuelsen, S. O., & Magnus, P. (1999). Surface materials in the home and development of bronchial obstruction in young children in Oslo, Norway. American Journal of Public Health, 84(2), 188–192. https://doi.org/10.2105/AJPH.89.2.188.
Järnström, H., Saarela, K., Kalliokoski, P., & Pasanenc, A.-L. (2006). Reference values for indoor air pollutant concentrations in new, residential buildings in Finland. Atmospheric Environment, 40, 7178–7191. https://doi.org/10.1016/j.atmosenv.2006.06.021.
Jiang, C., Li, D., Zhang, P., Li, J., Wang, J., & Yu, J. (2017). Formaldehyde and volatile organic compound (VOC) emissions from particleboard: Identification of odorous compounds and effects of heat treatment. Building and Environment, 117, 118–126. https://doi.org/10.1016/j.buildenv.2017.03.004.
Johansson, P., Bok, G., & Ekstrand-Tobin, A. (2013). The effect of cyclic moisture and temperature on mould growth on wood compared to steady state conditions. Building and Environment, 65, 178–184. https://doi.org/10.1016/j.buildenv.2013.04.004.
Kajiwara, N., & Takigami, H. (2016). Particle size distribution of brominated flame retardants in house dust from Japan. Emerging Contaminants, 2(2), 109–117. https://doi.org/10.1016/j.emcon.2016.03.005.
Kaminsky, D. A. (2012). What does airway resistance tell us about lung function? Respiratory Care, 57(1), 85–96. https://doi.org/10.4187/respcare.01411.
Kim, S. S., Kang, D. H., Choi, D. H., Yeo, M. S., & Kim, W. K. (2012). VOC emission from building materials in residential buildings with radiant floor heating systems. Aerosol and Air Quality Research, 12, 1398–1408. https://doi.org/10.4209/aaqr.2011.11.0222.
Kishi, R., Araki, A., Saitoh, I., Shibata, E., Morimoto, K., Nakayama, K., et al. (2012). Phthalate in house dust and its relation to sick building syndrome and allergic symptoms. In 30th International Congress on Occupational Health organized in Cancun from March 18th to March 23rd, 2012, Mexico.
Kontonasiou, E., Atanasiu, B., & Mariottini, F. (2015). Fuel poverty mitigation through energy efficiency in buildings. BPIE EU, Buildings Performance Institute Europe, Bruxelles. Retrieved December 3, 2018 from http://bpie.eu/wp-content/uploads/2015/10/BPIEposter-Fuel-Poverty20151.pdf.
Krašovec, J. (2019). Human values of an individual in space and time. Vrednote človeka kot osebnega bitja v prostoru in času. In: M. Dovjak, J. Krašovec (Eds.), Role and meaning of individual in the process of building construction. Invited lecture. Vloga in pomen posameznika v procesu graditve stavb. Invited lecture. Dvorana Slovenske matice, Ljubljana, 26.02.2019. Retrieved Februay 28, 2019, from http://www.slovenska-matica.si/events/predavanje-vloga-pomen-posameznika-v-procesu-graditve-stavb/.
Lappalainen, V., Sohlberg, E., Järnström, H., Laamanen, J., Viitanen, H., & Pasanen, P. (2015). IAQ simulator tests: VOC emissions from hidden mould growth. Energy Procedia, 78, 1212–1217. https://doi.org/10.1016/j.egypro.2015.11.187.
Lavin, T., Higgins, C., Metcalfe, O., & Jordan, A. (2006). Health impacts of the built environment a review. Institute of Public Health in Ireland, July 2006. Retrieved December 3, 2018, from https://www.publichealth.ie/files/file/Health_Impacts_of_the_Built_Environment_A_Review.pdf.
Law, A. K. Y., Chau, C. K., & Chan, G. Y. S. (2001). Characteristics of bioaerosol profile in office buildings in Hong Kong. Building and Environment, 36(4), 527–541. https://doi.org/10.1016/S0360-1323(00)00020-2.
Lu, C. Y., Ma, Y. C., Lin, J. M., Li, C. Y., Lin, R. S., & Sung, F. C. (2007). Oxidative stress associated with indoor air pollution and sick building syndrome-related symptoms among office workers in Taiwan. Inhalation Toxicology, 19, 57–65. https://doi.org/10.1080/08958370600985859.
Lu, C., Deng, Q., Li, Y., Sundell, J., & Norbäck, D. (2016). Outdoor air pollution, meteorological conditions and indoor factors in dwellings in relation to sick building syndrome (SBS) among adults in China. Science of the Total Environment 560–561, 186–196. http://www.sciencedirect.com/science/article/pii/S0048969716307148. Retrieved December 3, 2017, from http://dx.doi.org/10.1016/j.scitotenv.2016.04.033.
Malkin, J. (2008). A visual reference for evidence-based design. Concord, CA, USA: Center for Health Design.
Metin Özcan, K., Gülay, E., & Üçdoğruk, S. (2013). Economic and demographic determinants of household energy use in Turkey. Energy Policy, 60, 550–557. https://doi.org/10.1016/j.enpol.2013.05.046.
Mizoue, T., Reijula, K., & Andersson, K. (2001). Environmental tobacco smoke exposure and overtime work as risk factors for sick building syndrome in Japan. American Journal of Epidemiology, 154, 803–808. https://doi.org/10.1093/aje/154.9.803.
Nakaoka, H., Todaka, E., Seto, H., Saito, I., Hanazato, M., Watanabe, M., et al. (2014). Correlating the symptoms of sick-building syndrome to indoor VOCs concentration levels and odour. Indoor and Built Environment, 23, 804–813. https://doi.org/10.1177/1420326X13500975.
Nimmermark, S., & Gustafsson, G. (2005). Influence of temperature, humidity, and ventilation rate on the release of odour and ammonia in a floor housing system for laying hens. Agricultural Engineering International, VII 15.
NIPH. (2012). Guidelines for reducing the risk of Legionella growth. Ljubljana: NIPH.
Omrani, S., Garcia-Hansen, V., Capra, B. R., & Drogemuller, R. (2017). Effect of natural ventilation mode on thermal comfort and ventilation performance: Full-scale measurement. Energy Buildings, 156, 1–16. http://dx.doi.org/10.1016/j.enbuild.2017.09.061.
Ooi, P., & Goh, K. (1997). Sick building syndrome: an emerging stress-related disorder? International Journal of Epidemiology, 26, 1243–1249. https://doi.org/10.1093/ije/26.6.1243.
Park, J. H., Spiegelman, D. L., Gold, D. R., Burge, H. A., & Milton, D. K. (2001). Predictors of airborne endotoxin in the home. Environmental Health Perspectives, 109(8), 859–864. https://doi.org/10.1289/ehp.01109859.
Paustenbach, D. J. (2002). Human and ecological risk assessment: Theory and pactice (1st ed.). D. J. Paustenbach, &W. K. Reilly (Foreword). John Wiley and Sons, New York.
Peat, J., Dickerson, J., & Li, J. (1998). Effects of damp and mould in the home on respiratory health: a review of the literature. Allergy, 53, 120–128. https://doi.org/10.1111/j.1398-9995.1998.tb03859.x.
Prussin, A. J., Schwake, O. D., & Marr, L. C. (2017). Ten questions concerning the aerosolization and transmission of Legionella in the built environment. Building and Environment, 123, 684–695. https://doi.org/10.1016/j.buildenv.2017.06.024.
Recek, P. (2017). The quality of indoor environment in association with socio-economic indicators. Pilot Study: Faculty of Health Sciences, University of Ljubljana, Ljubljana.
Recek, P., Kump, T., & Dovjak, M. (2019). Indoor environmental quality in relation to socioeconomic indicators in Slovenian households. Journal of Housing and the Built Environment. https://doi.org/10.1007/s10901-019-09659-x.
Redlich, C. A., Sparer, J., & Cullen, M. R. (1997). Sick-building syndrome. The Lancet, 349, 1013–1016. https://doi.org/10.1016/S0140-6736(96)07220-0.
Sahlberg, B., Gunnbjörnsdottir, M., Soon, A., Jogi, R., Gislason, T., Wieslander, G., et al. (2013). Airborne molds and bacteria, microbial volatile organic compounds (MVOC), plasticizers and formaldehyde in dwellings in three North European cities in relation to sick building syndrome (SBS). Science of the Total Environment, 444, 433–440. https://doi.org/10.1016/j.scitotenv.2012.10.114.
Sakai, K., Norbäck, D., Mi, Y., Shibata, E., Kamijima, M., Yamada, T., et al. (2004). A comparison of indoor air pollutants in Japan and Sweden: formaldehyde, nitrogen dioxide, and chlorinated volatile organic compounds. Environmental Research, 94, 75–85. https://doi.org/10.1016/S0013-9351(03)00140-3.
Salthammer, T., Mentese, S., & Marutzky, R. (2010). Formaldehyde in the indoor environment. Chemical Reviews, 110, 2536–2572. https://doi.org/10.1021/cr800399g.
Salimifard, P., Rim, D., Gomes, C., Kremer, P., & Freihaut, J. D. (2017). Resuspension of biological particles from indoor surfaces: Effects of humidity and air swirl. Science of the Total Environment, 583, 241–247. https://doi.org/10.1016/j.scitotenv.2017.01.058.
Santamouris, M., Kapsis, K., Korres, D., Livada, I., Pavlou, C., & Assimakopoulos, M. N. (2007). On the relation between the energy and social characteristics of the residential sector. Energy Build 39(8), 893–905. Retrieved December 3, 2018, from http://dx.doi.org/10.1016/j.enbuild.2006.11.001.
Sautour, M., Soares Mansur, C., Divies, C., Bensoussan, M., & Dantigny, P. (2002). Comparison of the effects of temperature and water activity on growth rate of food spoilage moulds. Journal of Industrial Microbiology & Biotechnology, 28, 311–315. https://doi.org/10.1038/sj.jim.7000248.
Schwartz, S. (2008). Linking noise and vibration to sick building syndrome in office buildings 2008. Air & Waste Management Association. Retrieved December 3, 2018, from http://sandischwartz.com/wp-content/uploads/2015/07/EM_Magazine_final_printed_article.pdf.
Sekulska, M., Piotraszewska-Pająk, A., Szyszka, A., Nowicki, M., & Filipiak, M. (2007). Microbiological quality of indoor air in university rooms. Polish Journal of Environmental Studies, 16(4), 623–632.
Seppänen, O., Fisk, W., & Mendell, M. (1999). Association of ventilation rates and CO2 concentrations with health and other responses in commercial and industrial buildings. Indoor Air, 9, 226–252. https://doi.org/10.1111/j.1600-0668.1999.00003.x.
Seppänen, O., & Fisk, W. (2002). Association of ventilation system type with SBS symptoms in office workers. Indoor Air, 12, 98–112. https://doi.org/10.1034/j.1600-0668.2002.01111.x.
Shan, X., Zhou, J., Chang, V. W.-C., & Yan, E.-H. (2016) Comparing mixing and displacement ventilation in tutorial rooms: Students’ thermal comfort, sick building syndromes, and short-term performance. Building and Environment, 102, 128–137. http://dx.doi.org/10.1016/j.buildenv.2016.03.025.
Sheehan, P., Singhal, A., Bogen, K. T., MacIntosh, D., Kalmes, R. M., & McCarthy, J. (2017). Potential exposure and cancer risk from formaldehyde emissions from installed Chinese manufactured laminate flooring. Risk Analysis, 38(6), 1128–1142. https://doi.org/10.1111/risa.12926.
Sierra-Vargas, M. P., & Teran, L. M. (2012). Air pollution: Impact and prevention. Respirology, 17(7), 1031–1038.
Skov, P., Valbjorn, O., & Pedersen, B. V. (1990). Influence of indoor climate on the sick building syndrome in an office environment. Scandinavian Journal of Work, Environment & Health, 16(5), 363–371.
Smallwood, J. (2018). 7: Reducing static electricity in carpets. In Advances in carpet manufacture (2nd ed., pp. 135–162). The textile institute book series https://doi.org/10.1016/B978-0-08-101131-7.00008-3.
Subedi, B., Sullivan, K. D., & Dhungana, B. (2017). Phthalate and non-phthalate plasticizers in indoor dust from childcare facilities, salons, and homes across the USA. Environmental Pollution, 230, 701–708. https://doi.org/10.1016/j.envpol.2017.07.028.
Sun, C., Huang, C., Liu, W., Zou, Z., Hu, Y., & Shen, L. (2017). Home dampness-related exposures increase the risk of common colds among preschool children in Shanghai, China: Modified by household ventilation. Building and Environment, 124, 31–41. https://doi.org/10.1016/j.buildenv.2017.07.033.
Šarić, M., Kulcar, Z., Zorica, M., & Gelić, I. (1976). Malignant tumors of the liver and lungs in an area with a PVC industry. Environmental Health Perspectives, 17, 189–192. https://doi.org/10.1289/ehp.7617189.
Šestan, P., Kristl, Ž., & Dovjak, M. (2013). Formaldehyde in the built environment and its potential impact on human health. Gradbeni vestnik, 62, 191–203.
Takeuchi, S., Kojima, H., Saito, I., Jin, K., Kobayashi, S., Tanaka-Kagawa, T., et al. (2014). Detection of 34 plasticizers and 25 flame retardants in indoor air from houses in Sapporo, Japan. Science of the Total Environment, 491–492, 28–33. https://doi.org/10.1016/j.scitotenv.2014.04.011.
Takigawa, T., Saijo, Y., Morimoto, K., Nakayama, K., Shibata, E., Tanaka, M., et al. (2012). A longitudinal study of aldehydes and volatile organic compounds associated with subjective symptoms related to sick building syndrome in new dwellings in Japan. Science of the Total Environment, 417–418, 61–67. https://doi.org/10.1016/j.scitotenv.2011.12.060.
Teeuw, K., Vandenbroucke-Grauls, C., & Verhoef, J. (1994). Airborne gram-negative bacteria and endotoxin in sick building syndrome. A study in Dutch governmental office buildings. Archives of Internal Medicine, 154, 2339–2345. https://doi.org/10.1001/archinte.154.20.2339.
Temeljotov Salaj, A., Maamari, B., Baričič, A., & Lohne, J. (2015). The influence of workplace on overall health in Slovenia and Lebanon-empirical research. HealthMed, 9(7), 281–300.
Temeljotov Salaj, A., Baričič, A., & Maamari, B. (2017). How the economic crisis affects workplace conditions and occupational health. Journal of Construction Project Management and Innovation, 7(2), 2088–2103.
Velux. (2016). The healthy homes barometer 2016. Retrieved December 3, 2018, from http://www.velux.com/article/2016/energy-renovation-resonates-with-european-home-owners.
Velux Group. (2017). Healthy homes barometer 2017. Retrieved December 3, 2018, from http://velcdn.azureedge.net/~/media/com/health/healthy-home-barometer/507505-01%20barometer_2017.pdf.
Verreault, D., Moineau, S., & Duchaine, C. (2008). Methods for sampling of airborne viruses. Microbiology and Molecular Biology Reviews, 72(3), 413–444. https://doi.org/10.1128/MMBR.00002-08.
Wang, J., Li, B., Yang, Q., Yu, W., Wang, H., Norback, D., et al. (2013). Odors and sensations of humidity and dryness in relation to sick building syndrome and home environment in Chongqing, China. PLoS One, 8, e72385 http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0072385. Retrieved December 3, 2017, from http://dx.doi.org/10.1371/journal.pone.0072385.
Wargocki, P. (2013). Productivity and health effects of high indoor air quality. In Reference module in earth systems and environmental sciences. https://www.sciencedirect.com/science/article/pii/B978012409548901993X. Retrieved December 3, 2018, from http://dx.doi.org/10.1016/B978-0-12-409548-9.01993-X.
Washington Post. (1999). Daylighting and productivity-CEC PIER. Study says natural classroom lighting can aid achievement. By Cooper KJ. Washington Post Staff Writer Washington Post, Friday, November 26, 1999, Page A14. Retrieved December 3, 2018, from http://h-m-g.com/projects/daylighting/publicity%20daylighting.htm.
WHECA. (2000). Warm homes and energy conservation act 2000. Retrieved December 3, 2018, from https://www.legislation.gov.uk/ukpga/2000/31/contents.
WHO. (2004). Children’s health and the environment. Geneva: World Health Organization.
WHO. (2012). Environmental health inequalities in Europe. Retrieved December 3, 2018, from http://www.euro.who.int/__data/assets/pdf_file/0010/157969/e96194.pdf?ua=1.
WHO. (2017). Indoor air pollution. Cost-benefit analysis of interventions. Retrieved December 3, 2017, from http://www.who.int/indoorair/interventions/cost_benefit/en/.
Weichenthal, S., Dufresne, A., & Infante-Rivard, C. (2007). Indoor ultrafine particles and childhood asthma: Exploring a potential public health concern. Indoor Air, 17, 81–91. https://doi.org/10.1111/j.1600-0668.2006.00446.x.
Wieslander, G., Norback, D., & Venge, P. (2007). Changes of symptoms, tear film stability and eosinophilic cationic protein in nasal lavage fluid after re-exposure to a damp office building with a history of flooding. Indoor Air, 17, 19–27. https://doi.org/10.1111/j.1600-0668.2006.00441.x.
Wyon, D. F., & Wargocki, P. (2013). Effects of indoor environment on performance. ASHRAE Journal 46–50. Retrieved November 10, 2017, from http://www.rehva.eu/fileadmin/REHVA_Journal/REHVA_Journal_2013/RJ_issue_4/p.6/06-10-RJ1304_web.pdf.
Xu, J., & Zhang, J. S. (2011). An experimental study of relative humidity effect on VOCs effective diffusion coefficient and partition coefficient in a porous medium. Building and Environment, 46(9), 1785–1796. https://doi.org/10.1016/j.buildenv.2011.02.007.
Xu, Y., Cohen Hubal, E., & Little, J. (2009). Predicting residential exposure to phthalate plasticizer emitted from vinyl flooring: a mechanistic analysis. Environmental Science and Technology, 43, 2374–2380. https://doi.org/10.1021/es801354f.
Yassi, A., Kjellstrom, T., de Kok, T., & Guidotti, T. (2001). Basic environmental health: Oxford University Press, Inc.
Yassin, M., & Almouqatea, S. (2010). Assessment of airborne bacteria and fungi in an indoor and outdoor environment. International Journal of Environmental Science and Technology, 7(3), 535–544. https://doi.org/10.1007/BF03326162.
Yun, G. Y., & Steemers, K. (2011). Behavioural, physical and socio-economic factors in household cooling energy consumption. Applied Energy, 88(6), 2191–2200. https://doi.org/10.1016/j.apenergy.2011.01.010.
Zak, J. C., & Wildman, H. G. (2004) 14-Fungi in stressful environments. In Biodiversity of fungi (pp. 303–315). Burlington: Academic Press.
Zhu, L., Deng, B., & Guo, Y. (2013). A unified model for VOCs emission/sorption from/on building materials with and without ventilation. International Journal of Heat and Mass Transfer, 67, 734–740. http://www.sciencedirect.com/science/article/pii/S001793101300762X. Retrieved December 3, 2018, from http://dx.doi.org/10.1016/j.ijheatmasstransfer.2013.08.092.
Zhang, Y., Luo, X., Wang, X., Qian, K., & Zhao, R. (2007). Influence of temperature on formaldehyde emission parameters of dry building materials. Atmospheric Environment, 41(15), 3203–3216. https://doi.org/10.1016/j.atmosenv.2006.10.081.
Ƶhang, X., Sahlberg, B., Wieslander, G., Janson, C., Gislason, T., & Norback, D. (2012). Dampness and moulds in workplace buildings: Associations with incidence and remission of sick building syndrome (SBS) and biomarkers of inflammation in a 10 year follow-up study. Science of the total environment, 430, 75–81.
Zinn, T. W., Cline, D., & Lehmann, W. F. (1990). Long-term study of formaldehyde emission decay from particleboard. Forest Products Journal, 40(6), 15–18.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2019 The Author(s)
About this chapter

Cite this chapter
Dovjak, M., Kukec, A. (2019). Interactions Among Health Risk Factors and Decision-Making Process in the Design of Built Environments. In: Creating Healthy and Sustainable Buildings. Springer, Cham. https://doi.org/10.1007/978-3-030-19412-3_4
Download citation
DOI: https://doi.org/10.1007/978-3-030-19412-3_4
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-19411-6
Online ISBN: 978-3-030-19412-3
eBook Packages: MedicineMedicine (R0)