
Abstract
Diseases of the air space of the lung share many common findings and presentation that it makes more sense to be grouped together in a differential diagnosis. The common imaging finding is usually as a lung infiltrate or consolidation of some type of distribution or another. Trying to find the putative cause for the imaging pattern is a good first step in narrowing the differential diagnosis and answering the question: what accounts for this pattern on imaging studies? Most of these diseases have an acute or subacute onset and exhibit restrictive pattern on pulmonary function tests. When treated promptly, they resolve completely with little or no residual injury to the lung architecture.
On a small biopsy it is important to have a clinical history and imaging results before embarking on a descriptive rather than a definitive diagnosis. The smaller the sample, the more information is needed to complete the picture. Pulmonologists should be advised to target the part of the lung that should provide the most information related to the process under investigation. An endobronchial wall biopsy is not suitable in the setting of investigating a lung infiltrate as part of the alveolated lung has to be included.
The category of airspace-occupying diseases of the lung includes:
-
1.
Acute lung infections such as bacterial and viral pneumonias
-
2.
Acute lung injury pattern which includes bronchiolitis obliterans/organizing pneumonia and diffuse alveolar damage
-
3.
Intra-alveolar hemorrhage
-
4.
Pulmonary alveolar proteinosis
-
5.
Pulmonary edema
-
6.
Pneumocystis pneumonia
-
7.
Lymphangitic carcinomatosis
In all of these instances, there are ground-glass opacities obscuring the air space. Most clinicians would describe the imaging as “infiltrate” or “consolidation.” The task for the pathologist is to find the pertinent finding that could account for the imaging.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others



Keywords
- Bronchopneumonia
- Bronchiolitis obliterans/organizing pneumonia
- Cryptogenic organizing pneumonia
- Diffuse alveolar damage
- Intra-alveolar hemorrhage
- Pulmonary alveolar proteinosis
- Aspiration pneumonia
- Lipoid pneumonia
Acute Pneumonias
Acute pneumonias could be divided into infectious, which include bacterial, fungal, and viral ones, and noninfectious which include aspiration, lipoid, and allergic ones. In most cases of bacterial or viral pneumonia, a biopsy is not needed to make the diagnosis as other microbiological studies or empirical treatment is instated based on the clinical picture and imaging finding. Only in cases that do not respond to antibiotics or because of other compounding factor like in immunocompromised patients, a biopsy is obtained, and the infectious process is evident through the presence of numerous neutrophils with or without a mucopurulent exudate as in Fig. 4.1a, b.

Low magnification view of the fibrinopurulent exudate in the alveolar space with thickening of the interalveolar septa in (a). A higher magnification of the same pattern shows the neutrophilic infiltrate in the alveoli as well as in the interstitium in (b)
On a small biopsy, the presence of acute inflammation and/or necrosis is a fortuitous finding. It tends to be sporadic or focal judging from the autopsy material. Usually, by the time a patient is scheduled for a biopsy, the most common finding is the organizing pneumonia which will be discussed later under the acute lung injury pattern.
Viral pneumonia could present in different ways. Adenovirus infection could be subtle and shows only as dark smudgy nuclei in the alveolar lining or with viral cytopathic effect showing ground-glass nuclei. On the other hand, influenza virus and herpes simplex virus (HSV) tend to cause areas of necrosis and some neutrophilic infiltrate similar to that of bacterial pneumonia. The clue to the viral etiology would be based on the presence of viral cytopathic changes with nuclear inclusions in case of the HSV and ground-glass nuclei in the influenza virus. These findings could be present in the background of diffuse alveolar damage (DAD), and recognizing the viral etiology or other etiologies in general is important in the treatment of these cases. Cytomegalovirus induces only chronic inflammation and is characterized by the enlarged cells with basophilic nuclear inclusions. The virus usually infects alveolar lining cells and endothelial cells.
Acute Lung Injury Pattern
The clinical definition of acute lung injury has evolved over the years. In its latest iteration, it is defined as the ratio of the partial pressure of the arterial oxygen relative to that pressure in inspired air. A ratio of <300 is considered indicative of acute lung injury, and a ratio <200 confirms respiratory failure due to acute respiratory distress syndrome (ARDS) [1].
From the histopathologic point of view, the acute lung injury pattern is one that is predominantly of organizing fibrosis mainly by fibroblastic proliferation and a recent myxoid background. The fibrosis is of the recent type without dense collagen deposition or distortion of lung architecture as would be highlighted by a reticulin stain. The main two entities of this pattern are DAD which is the majority of cases of ARDS. The idiopathic variant of DAD is acute interstitial pneumonia (AIP) or Hamman-Rich disease. The other entity is bronchiolitis obliterans/organizing pneumonia (BOOP) with its idiopathic variant called cryptogenic organizing pneumonia (COP) [2]. There is a substantial overlap in the histomorphologic features between BOOP and DAD. In both of these entities, there are commonly:
-
1.
Thickening of the interalveolar septa with mild chronic inflammatory infiltrate and fibroblastic proliferation. The septa could also demonstrate intercellular edema exaggerating the thickness of the septa and making it appear as a reticular pattern.
-
2.
Proliferation of type II pneumocytes lining the alveolar spaces.
-
3.
Proliferation of the fibroblasts forming polypoid and fascicular bundles filling up the alveolar spaces to be called “fibroblastic plugs.” The latter could plug the alveolar air spaces or the bronchial lumens.
The lung will turn into a consolidated mass with sporadic air spaces in predominantly fibroelastic mass comprised by the thick septa and fibroblastic plugs [3]. This in turn hinders gas diffusion and hence results in the shortness of breath and hypoxia when measuring blood gases.
Bronchiolitis Obliterans/Organizing Pneumonia
It is by far the most common pattern seen on a lung biopsy. Several reasons account for that; BOOP could be encountered as a reaction to the primary lung injury. This would include post-infectious pneumonia, inhalational injury, post radiation, aspiration pneumonia, and in the setting of collagen vascular disease. In addition, BOOP could be present around mass lesions in the lung such as tumors or granulomas. In the latter situation, if there is familiarity with imaging finding and if there is suspicion for a mass lesion, it is important to communicate to the clinician that the presence of BOOP could be a nonspecific finding, which does not account for the mass lesion seen on imaging. The other scenario where BOOP can be present is as a minor component of other disease entities such as hypersensitivity pneumonia or nonspecific interstitial pneumonia [4].
Histopathologic Features
BOOP usually appears as polypoid structures bulging into the air spaces in the peribronchial areas with a short stalk embedded in the interstitium (Fig. 4.2a, b). Some fascicles of elongated fibroblasts could be seen extended in parallel to the interalveolar septa. Using collagen stains such as Movatt stain, the highlighted light green color of recent organizing fibrosis pattern appears as a tree of cauliflower extending throughout the lung parenchyma in the area of biopsy [5]. The polypoid masses used to be called “Masson’s bodies.” The interstitial cellular infiltrate is usually comprised by a mixture of lymphocytes, plasma cells, macrophages, and neutrophils (Fig. 4.3a, b ). The presence of lymphoid aggregates or lymphoid follicles with germinal centers should raise the possibility of a more chronic process such as hypersensitivity pneumonia (HP) or collagen vascular disease. The presence of poorly formed granulomas and eosinophils would make the first more likely, and the history and serologic testing would confirm the latter.

Low power magnification of a small biopsy showing the pale areas with the myxoid fibroblastic plugs and the cellular infiltrate in the thickened interalveolar septa. The air spaces are markedly reduced by the infiltrate (a). The polypoid plug with its stalk is shown with swirling bands of fibroblasts (b)

Another example of a polypoid fibroblastic plug filling up the alveolar space (a), and another one is almost obliterating the bronchial lumen (b)
Whereas, in most cases, the histomorphologic features do not provide the underlying etiology of BOOP, it is important to not ignore some of the easily recognizable etiologies. Finding a frothy material in the alveolar space in an immunocompromised patient would suggest Pneumocystis jiroveci pneumonia. In addition, looking for viral inclusions or smudgy nuclei characteristic of adenovirus infection would elicit the causing agent in some cases.
Sometimes, it is difficult to rule out DAD based on a small biopsy, and because of the significant overlap between BOOP and DAD, an umbrella term such as “acute lung injury pattern” may be a useful first step in characterizing the lesion in the lung. DAD usually has an interstitial pattern with less fibroblastic plugs and more fascicles of fibroblasts and of course the hallmark of hyaline membrane. These could be sporadic and not included in the small transbronchial biopsy, but the use of acute lung injury pattern could cover both entities as they share common therapeutic and management pathways.
Another term that is usually confused with BOOP is obliterative bronchiolitis or constrictive bronchiolitis. Many in the lung transplant community refer to it as “bronchiolitis obliterans” which is the opposite of BOOP clinically and histopathologically. Obliterative bronchiolitis most commonly occurs as a late complication of transplant rejection and is mainly a small airway disease. The lung parenchyma is almost normal, and the main problem is the presence of an annular band of fibrosis constricting the lumen of the small airways [6]. Movatt stain is helpful in highlighting the fibrosis.
Idiopathic BOOP is usually a problem on imaging and clinically. As the name suggests, there is no prior incident to suggest the presence of a sole area of consolidation or ground-glass opacity in the lung, and suspicion of malignancy is in the differential diagnosis, especially for adenocarcinoma in situ, which used to be called bronchioloalveolar carcinoma. This particular type was recognized as a separate clinicopathologic entity and given the name COP. However, from the histopathologic standpoint, it is similar in every aspect to BOOP [7].
Diffuse Alveolar Damage and Adult Respiratory Distress Syndrome
DAD is characterized by an insidious onset and a rapid course of respiratory failure requiring mechanical ventilation in most cases. In clinical terminology, this is recognized as ARDS. However, there are several etiologies that could result in ARDS but fail to show the characteristic findings of DAD in histopathologic examination. For instance, acute silicosis could result in massive pulmonary edema that results in ARDS, but the pathology of course is not that of DAD. All cases of DAD are considered part of ARDS but not all cases of ARDS would result in DAD. The list of potential causative agents is long and variable. The list includes infection, toxic inhalants, drugs, radiation and chemotherapy, trauma and shock, burns, and certain ingested material like kerosene.
Pathologically, the disease goes through two stages:
Exudative phase: usually in the first week of presentation and is characterized by presence of patchy areas of pulmonary edema and plasma proteins in the alveolar spaces. There are mild or focal areas of thickening of the interalveolar septa.
Organizing phase: usually sets in the second week and usually when the patient is stable enough to be biopsied. They are usually the findings discussed above. In later stages the hyaline membrane would start to disappear leaving behind a small fragment of fibrin or hyaline membrane embedded within the interstitium. This is a result of the sticky surfaces of opposing hyaline membrane-coated alveolar linings fusing together and taking with them the hyaline membrane in what would appear as the interstitium. In this stage the presence of organized fibrin thrombi in small blood vessels could be used in lieu of the hyaline membrane to diagnose DAD.
Histopathologic Features
The biopsy from a patient with DAD shares many similarities with those from BOOP. However, certain points need to be understood to recognize the difference between these two entities:
-
1.
DAD is a combination of an epithelial injury as well as endothelial injury. As such, the endothelial injury will result in leakage from the small vessels and the formation of intravascular thrombi, and plasma proteins will be present in the alveolar spaces. When the degeneration and necrosis by-products mix with the fibrin from the plasma proteins, they form a slurry-like material that paints the alveolar lining layer as what we recognize as the hyaline membrane (Fig. 4.4a, b ). The latter makes gas diffusion more difficult than even in BOOP. For this and other reasons, patients with DAD usually require mechanical ventilation and have worse prognosis than those with BOOP [8].
Fig. 4.4 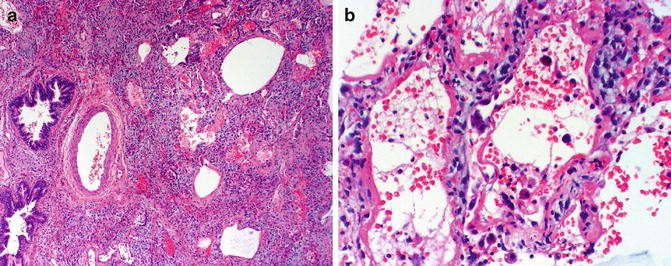
Organizing diffuse alveolar damage with the loose myxoid background and diminished air spaces similar to that in BOOP without the polypoid fibroblastic plugs (a). The well-defined hyaline membrane is lining the alveolar spaces with a continuous undulating pattern and the thick interalveolar septa with intercellular edema (b)
-
2.
The presence of intravascular thrombi in larger vessels could lead to areas of lung infarctions. These could ultimately result in the squamous metaplasia with atypia. These areas could include abnormal mitotic figures and areas of necrosis. It is very important to be very cautious in interpreting fine needle aspiration material or bronchoalveolar lavages (BALs) from patients suspected of having DAD or who are on ventilators. The metaplastic squamous epithelial cells along with the necrotic debris could lead to an erroneous diagnosis of squamous cell carcinoma (Fig. 4.5a, b).
Fig. 4.5 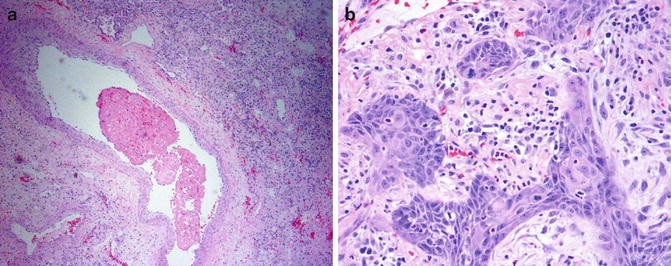
An intravascular thrombus blocking the lumen of medium-sized blood vessels (a). The area distal to these blood vessels showed pulmonary infarction with subsequent squamous metaplasia and atypical mitotic figures (b)
-
3.
Most patients with DAD get biopsied by the second week of presentation where the organizing phase is the predominant phase. However, some patients may be biopsied earlier. In the latter case, pulmonary edema and an eosinophilic material representing the leaked plasma proteins could be copiously present without the characteristic hyaline membrane or the areas of fibroblastic proliferation. Some authors called this “acute fibrinous and organizing pneumonia” (AFOP) [9]. Some investigators thought it belongs to a form of BOOP; others thought it represents an early phase of DAD (Fig. 4.6a, b). In practice the distinction is not important as the treatment would follow the patient’s performance status and the picture would be of an acute lung injury pattern.
Fig. 4.6 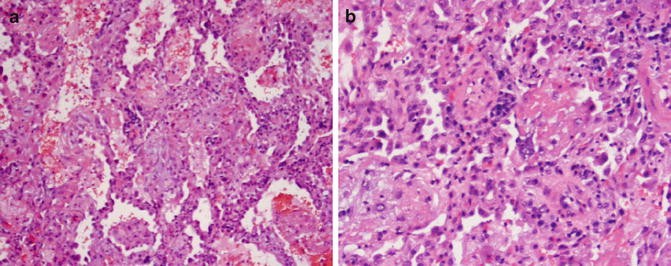
Low magnification view of the slightly thickened interalveolar septa, lined by type II pneumocytes and showing an eosinophilic material in the alveolar spaces (a). A closer view shows the lack of hyaline membrane and fibroblastic proliferation seen in the later organizing phase (b)
-
4.
The idiopathic form of DAD is also a distinct entity called “acute interstitial pneumonia” (AIP) or Hamman-Rich disease after the two physicians who first described the disease occurring in relatively young patients and resulting in an accelerated course of respiratory failure and a characteristic form of fibrosis on autopsy.
-
5.
DAD could be superimposed on cases of usual interstitial pneumonia (UIP), and in that case it is called “accelerated phase of UIP.” If the patient has been previously diagnosed with UIP or there is a radiologic evidence of UIP as would be discussed later, the presence of a DAD picture along with the honeycomb changes in the lung would point to that diagnosis. If there are several biopsies from different lobes, one might show UIP without DAD [10].
-
6.
A subset of patients with AIP may come with a protracted history of respiratory symptoms that does require mechanical ventilation only to show histopathologic evidence of DAD on the biopsy.



Intra-alveolar Hemorrhage
As a general rule the diagnosis of hemorrhage in the lungs requires the presence of hemosiderin macrophages. The mere presence of blood within the biopsy is not enough evidence for intra-alveolar hemorrhage as blood from the biopsy procedure is usually the culprit for such hemorrhage.
Intra-alveolar hemorrhage in its primary form is a diffuse process involving all areas of the lung. The potential etiology is usually an autoimmune disease such as Goodpasture syndrome [11]. In this case a small portion of the biopsy should be snap frozen for immunofluorescence studies. Other common causes would include vasculitides such as capillaritis syndrome in microscopic polyangiitis and Henoch-Schonlein purpura. Other primary diseases are associated with toxic inhalants and drugs. An idiopathic form also exists.
In Goodpasture syndrome, there is an associated renal lesion, and immunofluorescence with linear deposits along the basement membrane is diagnostic. There is a marked accumulation of hemosiderin-laden macrophages with their characteristic chunky refractile material with an orange or brown discoloration. They can also be deposited within the lung parenchyma. Iron stain usually is not needed to highlight hemosiderin as it is easy to identify on H&E stain (Fig. 4.7a, b).

Intra-alveolar hemorrhage with hemosiderin-laden macrophages containing chunky crystals brown to yellow hemosiderin (a). In a case of vasculitis, there are leaking vessels due to inflammation of the wall by the lymphocytic infiltrate of this case of lymphatoid granulomatosis with concomitant fibrin deposits in the alveoli. Notice the lack of neutrophilic infiltrate (b)
In cases of a vasculitis, a similar picture is present with the additional finding of fibrin in the alveolar spaces with the evidence of the vasculitis also present in the blood vessels.
In cases of idiopathic pulmonary hemosiderosis, the diagnosis is by exclusion as in any idiopathic case. The chronic bleeding may lead the marked deposits of hemosiderin to encrust the medial wall of the blood vessels resulting in what is called “endogenous pneumoconiosis.”
In secondary alveolar hemorrhage, the causes include infections especially necrotizing ones. Systemic diseases that affect the coagulation mechanisms such thrombocytopenia and coagulation defects, uremia, and renal failure are the most common ones.
Localized hemorrhage could be the result of a focal lesion or disease that causes bleeding in one or several small blood vessels. This includes vasoinvasive fungi such as aspergillus or narcotizing tumors. The bronchial wall could have lesions eroding through the wall and the accompanying vessel. The significance of identifying these lesions is to justify the resection that could be performed to stop the bleeding. Sometimes the pathologist is left with this task after the operation is performed, and if there is no lesion or an obvious culprit, the fear is that it could happen again.
Pulmonary Alveolar Proteinosis
Pulmonary alveolar proteinosis (PAP) is a rare disease that could be idiopathic, secondary, or congenital. In most cases the idiopathic or acquired form affects middle-age adults in 90 % of the cases. The secondary form (5–10 % of cases) is mainly due to inhalational exposure to industrial material such as silica, cement dust, aluminum, or titanium oxide. The rare congenital form affects children in the neonatal period. There is a controversy as whether it is a true PAP condition; however, the prognosis is invariably poor. The etiology of the primary type is poorly understood. It is thought to be a mutation that affects the function of GM-CSF, an important factor in surfactant homeostasis and an essential regulator in immune defense [12]. An increased level of GM-CSF autoantibodies was found in patients with primary PAP. Most patients present with dyspnea and nonproductive cough. Less common symptoms include low fever, weight loss, fatigue, and chest pain.
Imaging studies show areas of lung opacities sparing the apices and costophrenic angles on a chest X-ray. On CT scan the characteristic “crazy-paving” pattern is recognized. It is a combination of ground-glass opacities with reticular (septal) lines that involve any area of the lung but tend to spare the costophrenic angles. Even though the CT findings are highly suggestive, they are still nonspecific, and a lung biopsy is needed to confirm the diagnosis.
Histomorphologic Features
An eosinophilic amorphous material with cholesterol needle-shaped clefts is seen filling the alveoli. The alveolar walls are not usually affected by the process, but there could be a focal increase in the wall thickness that is filled by an inflammatory infiltrate. Small eosinophilic globules that stain positive with periodic acid-Schiff stain with diastase digestion are also present (Fig. 4.8a–c ). The interlobular septa are also widened and show abnormally dilated lymphatics.

General view of PAP showing the characteristic amorphous material in the alveolar space with needle-shaped cholesterol clefts (a). A higher magnification view of the D-PAS-positive globules in PAP (b). Contrasting view of pulmonary edema with a homogeneous material and several macrophages floating in the fluid (c)
The main differential diagnosis is with pulmonary edema where the edema leaves little strands of proteins or faint powdery material. Plasma proteins leaking in the alveolar space assume a homogeneous eosinophilic material that shows scalloping near the alveolar walls. The D-PAS-positive globules are also absent by special stains. Another differential is with the frothy material seen in Pneumocystis jiroveci. The latter is an infection in immunocompromised patients and as such usually shows widening of the interalveolar septa, and the material is frothy rather than granular with no cholesterol clefts or D-PAS-positive globules.
The treatment in these cases usually is by repeated BAL. The prognosis is usually good and few patients might need to have a repeat BAL within few months.
Pneumoconiosis
Most of pneumoconiosis results in an interstitial disease. The old entity of giant cell interstitial pneumonia or GIP was considered part of the idiopathic interstitial pneumonia till it was found to harbor many of the exogenous materials from industrial exposure. However, some of these agents can manifest in the alveolar spaces as numerous macrophages and giant cells containing the offending agent. The determination of the agent requires careful clinical history and tissue analysis of crystals and other materials in specialized laboratories.
Pulmonary Edema
Pulmonary edema is a common finding in hospitalized patients who undergo intravenous infusion, and they end up with circulatory overload. Patients with congestive heart failure, hypoproteinemia, or cirrhosis are prone to have pulmonary edema. The edema fluid can be serous with very few solutes or proteins, and this will appear as thinly reticular mesh or crisscrossing strands or powdery material in the alveolar spaces. If plasma proteins are admixed, they appear as a homogenous eosinophilic material. Corpora amylacea, which are concentrically lamellated eosinophilic bodies in the alveolar spaces, are usually seen especially in older patients. They are nonspecific findings in those patients and in autopsy cases.
References
Tsushima K, King LS, Aggarwal NR, De Gorordo A, D’Alessio FR, Kubo K. Acute lung injury review. Intern Med. 2009;48:621–30.
Cordier JF. Organising pneumonia. Thorax. 2000;55:318–28.
Epler GR. Bronchiolitis obliterans organizing pneumonia: definition and clinical features. Chest. 1992;102:2S–6S.
Epler GR, Colby TV. The spectrum of bronchiolitis obliterans. Chest. 1983;83:161–2.
Capdevila E, Banus E, Domingo C, Ferrer A, Mata JM, Marin A. [Bronchiolitis obliterans organizing pneumonia: the usefulness of the transbronchial biopsy as a diagnostic technic]. An Med Interna. 1994;11:449–51.
Myers JL, Colby TV. Pathologic manifestations of bronchiolitis, constrictive bronchiolitis, cryptogenic organizing pneumonia, and diffuse panbronchiolitis. Clin Chest Med. 1993;14:611–22.
Azzam ZS, Bentur L, Rubin AH, Ben-Izhak O, Alroy G. Bronchiolitis obliterans organizing pneumonia. Diagnosis by transbronchial biopsy. Chest. 1993;104:1899–901.
Blennerhassett JB. Shock lung and diffuse alveolar damage pathological and pathogenetic considerations. Pathology. 1985;17:239–47.
Beasley MB, Franks TJ, Galvin JR, Gochuico B, Travis WD. Acute fibrinous and organizing pneumonia: a histological pattern of lung injury and possible variant of diffuse alveolar damage. Arch Pathol Lab Med. 2002;126:1064–70.
Kaarteenaho R, Kinnula VL. Diffuse alveolar damage: a common phenomenon in progressive interstitial lung disorders. Pulm Med. 2011;2011:531302.
Boyce NW, Holdsworth SR. Pulmonary manifestations of the clinical syndrome of acute glomerulonephritis and lung hemorrhage. Am J kidney Dis. 1986;8:31–6.
Frazier AA, Franks TJ, Cooke EO, Mohammed TL, Pugatch RD, Galvin JR. From the archives of the AFIP: pulmonary alveolar proteinosis. Radiographics. 2008;28:883–99; quiz 915.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
Fraig, M.M. (2015). Airspace-Occupying Diseases. In: Fraig, M. (eds) Diagnosis of Small Lung Biopsy. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-2575-9_4
Download citation
DOI: https://doi.org/10.1007/978-1-4939-2575-9_4
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-2574-2
Online ISBN: 978-1-4939-2575-9
eBook Packages: MedicineMedicine (R0)