
Abstract
Due to the high prescription of antidepressants and their frequent involvement in clinical and forensic intoxications, reliable analytical techniques for identification and quantification of these therapeutic drugs should be available in clinical and toxicological laboratories. Improvements in liquid chromatography-mass spectrometry LC-MS(MS) technology over the last two decades have favored this technique to be one of the most commonly employed for this purpose, as it combines the high selectivity and sensitivity of the mass spectrometer with the great versatility of the liquid chromatographic separation. In this chapter, LC-MS(MS) applications for antidepressants determination are reviewed, detailing typical sample preparation techniques used for these therapeutic drugs, as well as common chromatographic and mass spectrometric characteristics. In addition, an LC-MS/MS method for the most common antidepressants used in clinical practice is described as an example of a whole method development and validation.
Similar content being viewed by others

Keywords
- Therapeutic Drug Monitoring
- Atmospheric Pressure Chemical Ionization
- Oral Fluid
- Mean Relative Error
- Oral Fluid Sample
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Antidepressants were first introduced into the market in the 1950s with the serendipitous discovery of the antidepressant effect of two drugs initially evaluated for other medical uses: Iproniazide, a monoamine oxidase inhibitor (MAOI), and Imipramine, a tricyclic antidepressant (TCA). Since then, a whole new generation of chemically and pharmacologically unrelated compounds have been introduced, which appear to be safer and better tolerated due to a more specific mechanism of action. These include selective serotonin reuptake inhibitors (SSRIs), serotonin and noradrenalin reuptake inhibitors (SNaRIs), noradrenergic and specific serotoninergic antidepressants (NaSSAs), and noradrenalin reuptake inhibitors (NaRIs).
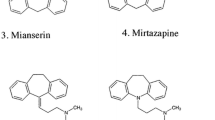
Figure 1 shows the chemical structures of some of the most common antidepressants used in clinical practice.

Chemical structure of some antidepressants commonly used in clinical practice
The main indication for antidepressants is depressive disorders, which have received increased attention owing to the growing recognition of their high prevalence. Other antidepressant uses include treatment of anxiety disorders, attention deficit hyperactivity disorders, nocturnal enuresis or psychosomatic disorders developed in several illnesses such as chronic pain, fibromyalgia, irritable bowel syndrome, or chronic fatigue syndrome.
Due to their high prescription, these therapeutic drugs are easy to acquire by depressed patients, who are prone to suicide attempts. This explains why antidepressants are among the most frequent therapeutic drug classes involved in forensic and clinical intoxications, mainly associated to voluntary intoxications [1–4]. Antidepressants with sedative side effects, like TCAs, could also be potentially used in drug facilitated sexual assault (DFSA) crimes [5]. Therefore, analytical techniques for the reliable identification and quantification of antidepressants should be available in clinical and forensic toxicology laboratories in order to perform a competent toxicological report. In addition, some antidepressants impair cognitive and psychomotor functions, and may increase the risk of driving accidents when under their influence [6–8]. For this reason, the Guidelines for Research in Drugged Driving elaborated by international experts in order to harmonize research in this field recommended the inclusion of sedative antidepressants in the panel of drugs to be analyzed in specimens collected from the roadside [9]. In addition to toxicological applications, analytical methodologies are also required to monitor plasmatic concentrations of some antidepressants. Therapeutic drug monitoring (TDM) of TCA is widely accepted [10–13] because of their narrow therapeutic window, and the development of severe cardiotoxicity and CNS toxicity close to the upper therapeutic concentrations; moreover, the enzymes involved in their metabolization show genetic polymorphism, being in part responsible for the interindividual variability in the plasmatic concentrations achieved at a given dose. Although new generations of antidepressants are less toxic and have wider therapeutic ranges due to a more selective mechanism of action, TDM of their plasmatic levels could be justified in special situations (assess compliance in nonresponder patients, hepatic or renal impairment, polymedicated patients, poor metabolizers, etc.) [11–13]. Antidepressant determination also is required to perform pharmacokinetic, bioavailability, and bioequivalence studies.
Different immunoassays are commercialized for the analysis of some antide-pressants [14–17]. Although useful for fast identification of these analytes, these techniques have several limitations: TCA are the main targeted analytes, it is not possible to differentiate between structurally related antidepressants, and several substances can cross-react with antidepressant assays [18–20]. Therefore, positive results must be confirmed with more specific techniques, usually using chromatography based procedures coupled to different detectors. Mass spectrometry is one of the most common detectors employed in clinical and toxicological analysis because of its high selectivity and sensitivity. Gas chromatography coupled to mass spectrometry (GC-MS) is a robust and well-established technique, and it is considered the golden standard for general unknown screening. Several GC-MS analytical methodologies have been described for identification and quantification of antidepressants in different biological matrices [21–25]; however, in most cases, antidepressants have to be derivatized because of their relatively high polarity. In the 1990s, the development of atmospheric pressure ionization interfaces (API) allowed the successful hyphenation of liquid chromatography to mass spectrometry (LC-MS). LC-MS combines the power of MS detection with the versatility of LC, which allows chromatographic separation of thermally unstable analytes, as well as compounds with a wide range of polarities without performing derivatization processes. For this reason, LC-MS and LC-MS/MS applications for the analysis of antidepressants have significantly grown over the last decade.
2 Sample Preparation for Antidepressants LC-MS(MS) Analysis
In the early stages of LC-MS, it was thought that the high selectivity provided by this technique could effectively eliminate intereferences caused by endogenous matrix compounds, and thus, the need for sample cleanup [26]. However, nowadays, it is well known that one limitation associated to LC-MS analysis is the suppression or enhancement on the analyte response when coeluting undetected compounds compete with the analyte in the ionization process [27, 28]. This phenomenon, generically known as matrix effect, may affect several validation parameters, such as the limit of detection, linearity, precision, and accuracy. Therefore, matrix effect may diminish method sensitivity and the reliability of quantitative results [29]. One of the main strategies to overcome matrix effect is to minimize the presence of these coeluting interferences through a more effective sample cleanup; thus, this step should be always taken into consideration when developing an LC-MS method.
Most of the published analytical methods for the determination of antidepressants were developed in plasma, serum, whole blood, and urine, which are the most useful matrices for clinical and toxicological analysis of these therapeutic compounds. However, albeit few, some LC-MS methodologies have also been described for the analysis of several antidepressants in hair [30–33], oral fluid [34, 35], breast milk [36], or typical forensic matrices such as gastric content, bile, vitreous humor, brain, liver, lung, and/or muscle [37–40].
Some biological matrices, such as hair and internal organs, require a special pretreatment prior to extraction. Hair samples must be washed to avoid external contamination, including an initial organic solvent, followed by aqueous washes [41]. After cutting or powdering, the hair matrix is usually disintegrated to extract the analytes from its inner structure. Ultrasonication in methanol (MeOH) [31, 32] or incubation in HCl [33] has been employed to extract antidepressants from the hair structure. Internal organs should be initially homogenized, and this process was usually performed in water or basic buffers by means of a blender or an ultrasonicator [37–40]. In addition, urine hydrolysis is sometimes performed to break glucuronide conjugates or some metabolites. β-Glucuronidase was employed for urine hydrolysis of mirtazapine [42] and bupropion metabolites conjugates [43, 44], and HCl was used for hydrolysis of 4-hydroxy-3-metoxy paroxetine metabolite [45], prior to sample extraction.
Several sample preparation or extraction procedures have been described for the analysis of antidepressants, from the most simple protein precipitation to online solid phase extraction (SPE). The optimum extraction technique depends on the analytical requirements, biological matrix, chromatographic separation, or the need for high throughput.
Several authors described a minimum sample pretreatment by plasmatic protein precipitation using acetonitrile (ACN), MeOH, acid solutions, or a mixture of them, for the analysis of one antidepressant and its metabolite(s) [46–52]. Single analyte procedures are useful for TDM or to perform pharmacokinetic, bioequivalence and pharmacogenomic studies, where the targeted antidepressant is known; however, this is an unrealistic situation in clinical and forensic toxicology, and for those applications, multianalyte procedures are preferable. Only Kirchherr et al. [53] used protein precipitation with ACN/MeOH as the only sample treatment procedure for the determination of 48 psychopharmaceuticals in human serum, including the main antidepressant drugs. No matrix effect was reported for any of the analytes, except for olanzapine, for which a 185% signal enhancement was observed.
However, protein precipitation usually produces severe matrix effect [54–56]. Therefore, in most LC-MS published methods, more extensive sample extraction procedures were used, being liquid–liquid (LLE) and SPE the most frequent techniques.
2.1 Liquid–Liquid Extraction (LLE)
In LLE, analytes are isolated from the biological matrix by means of an organic solvent immiscible with aqueous solution. Due to the basic character of antidepressants, samples are initially alkalinized with NaOH, NH4OH or a basic buffer to achieve a pH >8.5. The polarity range of the analytes included in the analytical method, as well as the biological matrix, determine the organic solvent of choice. Hexane, dichloromethane, butyl chloride, butyl acetate, isoamylic acid, or a mixture of them, have been used for the extraction of several antidepressants from the biological samples [39, 57–61]. Apart from those previously mentioned, other solvents employed for the extraction of only one antidepressant and/or metabolite(s) were diethylether, ethyl acetate or methyl tert-butylether [62–64]. After centrifugation, the organic layer is evaporated to dryness and reconstituted in a small volume for LC-MS analysis. In some cases, the organic layer was reextracted before evaporation by addition of aqueous acid solution to obtain cleaner extracts. De Santana et al. [42] and Halvorsen et al. [65] determined one or several antidepressants, respectively, in whole blood and/or plasma, using liquid-phase microextraction (LPME). LPME is a minituarized LLE procedure, where analytes are extracted from the biological matrix through an organic solvent impregnated in the pores of a hollow fiber and into a micro-liquid phase (acceptor solution) inside the fiber, which is subsequently injected into the LC-MS system. The main advantage of this technique is that it enables simultaneous analyte preconcentration and sample cleanup, using small sample and solvent volumes.
2.2 Solid Phase Extraction (SPE)
Different SPE procedures have been described using sorbents based on reversed-phase mechanism (C8, C18, hydrophilic–lipophilic balance), where the sample is loaded in basic conditions to guarantee analyte retention. After washing the cartridge, elution is performed with different organic solvents, sometimes in acid conditions [33, 66–71]. Due to the basic properties of antidepressants, mixed-mode sorbents simultaneously acting by reversed-phase and cation-exchange mechanisms, allow for a more selective extraction by removing nonbasic endogenous material [32, 34, 35, 43, 72, 73]. To allow analyte retention by cation-exchange mechanism, the sample should be initially conditioned with acidic solutions; after the washing step(s), analytes are eluted using alkalinized organic solvents. Common elution solvents are MeOH, ACN, dichloromethane, 2-propanol, or mixtures of them. The extraction process can be facilitated using semiautomated SPE robots [32, 66]. Moreover, online SPE-LC-MS instruments have also been employed for antidepressant analysis [72]. In these instruments, SPE extraction of the sample is performed in parallel to the chromatographic separation of the previous one, allowing complete automation of the whole analytical method, and the consequent sample high throughput.
2.3 Online Extraction
Online extraction techniques by means of supports coupled to the chromatographic system have also been applied to the determination of antidepressants [74–78]. These systems allow for direct sample injection, since large molecules from the biological matrix can readily pass through the column, while the analytes of interest can be retained under aqueous conditions, and subsequently eluted using high organic solvents composition. There are different supports, such as the so-called restricted access media (RAM), large particle size (LPZ) and monolithic supports, which can be used in the single column configuration or, more frequently, in the column-switching approach.
2.4 Solid-Phase Microextraction (SPME)
Another alternative technique, solid-phase microextraction (SPME), was used for the determination of fluoxetine [79] and several TCAs [80]. SPME is a miniaturized and solvent-free technique, where analytes are extracted from the sample by adsorption on a thin polymer coating fixed to the solid surface of a fiber, located inside an injection needle or a capillary. Its main disadvantage is that special strategies are needed to couple SPME to the LC-MS analysis.
3 Chromatographic Separation of Antidepressants by LC-MS(/MS)
LC is a very versatile technique that allows separation of nonvolatile, thermolabile and high polar analytes, without the need to perform derivatization processes. LC coupled to traditional detectors such as UV requires separation of interferences from the analyte of interest, and between them when several analytes are included in the analytical method; this is usually traduced in long chromatographic run times. The hyphenation of the LC system to the MS significantly reduced the chromatographic run, as there is no need for complete chromatographic resolution of the analytes included in the method. However, as previously mentioned, although endogenous interferences are not observed when analyte specific masses (m/z) or transitions are monitored, they can cause ion suppression or enhancement if they coelute with the analyte(s) of interest. Therefore, efficient chromatographic separation can minimize matrix effects and increase precision and accuracy of the assay.
In LC, several parameters such as the mobile phase, stationary phase, and column temperature can be optimized for a specific analytical application.
3.1 Mobile Phase
Mobile phase options are quite restricted, as only volatile buffers are suitable for LC-MS. In addition, ion-pairing agents traditionally used in LC to improve peak shape and retention time such as trifluoroacetic acid (TFA), have shown to produce ion suppression, and they are not recommended for LC-MS analysis [27]. Therefore, although few applications for specific antidepressants employ TFA or its ammonium salt due to sensitivity enhancement [48, 81–85], aqueous phases in most LC-MS analytical methods are composed by formic or acetic acid in water, or its ammonium buffers. Although acid mobile phases are by far the most common, basic aqueous mobile phases (pH ranging from 8 to 10) have been used for specific applications in order to increase antidepressant retention time or to couple the online SPE elution to chromatographic analysis [57, 72, 86, 87]. Organic phase composition was typically ACN and/or MeOH.
3.2 Stationary Phase
Antidepressant separation was usually performed by reversed-phase chromatography with typical C8 or C18 alkyl chain columns, although phenyl [30, 59] or cyano [48, 64, 84] stationary phases were also employed. As an exception, hydrophilic interaction liquid chromatography (HILIC), a variation of normal phase chromatography, was employed in two analytical methods for duloxetine [38] and paroxetine [85] determination, respectively. HILIC columns allow adequate retention of polar analytes poorly retained by reversed-phase chromatography, while still retaining less polar analytes; moreover, the high organic composition of the mobile phase increases electrospray efficiency, thus providing higher sensitivity. Chiral stationary phases were employed for enantioselective analysis of antidepressants marketed as a racemic mixture such as fluoxetine, citalopram, venlafaxine, mirtazapine, or bupropion [42, 43, 82, 88, 89].
Analytical methods for the determination of one antidepressant and/or its metabolite(s) were usually performed in isocratic mode, with total run times from seconds to a few minutes. However, as previously mentioned, multianalyte procedures are preferable, particularly if the method is intended for clinical or forensic analysis. Gradient separation was usually applied when the most common antidepressants were included in the methodology; however, total chromatographic run times varied widely, from 5 to 40 min [57, 76], depending on column length, extraction technique (offline vs. online techniques), biological matrix or the specific application of the method.
4 Mass Spectrometry Characteristics for Antidepressants LC-MS(MS) Analysis
4.1 Atmospheric Pressure Ionization Interfaces
Several LC-MS interfaces have been developed since 1974, when Arpino et al. [90] described the first attempt to couple the LC system to the mass spectrometer. Some of them were commercialized [91], but it was the development of atmospheric pressure ionization interfaces (API) which actually lead to the great expansion of LC-MS applications.
Within API interfaces, electrospray ionization (ESI) is the preferable ionization method for polar analytes, and it was used in the great majority of LC-MS methods for antidepressants analysis. However, ESI interfaces are more susceptible to matrix effects than atmospheric pressure chemical ionization (APCI) [54, 92, 93] due to differences in the ionization process. ESI is based on liquid phase reactions, where ion suppression is more likely than in gas phase due to high concentrations of nonvolatile materials present in the spray with the analyte [92]. Because of the lower susceptibility for matrix effects, although few, there have been authors who selected APCI as ionization mode in spite of the lower sensitivity for these analytes [59, 62, 74, 75]. Although ESI and APCI are by far the most popular ionization methods, other alternative interfaces were used for antidepressant analysis. Shinozuka et al. [69] used sonic spray ionization (SSI), a variant of ESI, where ionization is produced by high sonic gas velocity during pneumatic nebulization, instead of the electric field and capillary high temperatures applied in ESI. Atmospheric pressure photoionization (APPI) is a novel interface originally developed to widen the group of analytes to be determined by LC-MS towards less polar compounds that are not efficiently ionized by ESI or APCI. Theron et al. [61] compared ESI and APPI ionization for the analysis of venlafaxine and its metabolite O-desmethylvenlafaxine in plasma and water solutions. They concluded that the linearity of response in water, which is lost at high concentrations with ESI due to droplet surface saturation or limited amount of excess charge on the droplet, could be increased with APPI ionization. Moreover, APPI was less susceptible to ion suppression than ESI, with which signal response and calibration range was dramatically reduced in plasma compared to water, while similar results were obtained with APPI in both experiments. Regardless of the ionization method, positive ionization mode was employed in all cases, except for sulfate conjugates, which are more efficiently ionized in negative mode [45, 73].
4.2 Mass Analyzer
With regard to the mass analyzer, quadrupoles (Q) were usually employed due to its suitability for quantitative analysis and its relatively low prices, affordable for most laboratories. Ion trap mass spectrometers (IT) were employed in some but few LC-MS methodologies [65, 69, 74, 75]. Although these analyzers are less robust for quantitative analysis than Q, MSn spectrums can be obtained by successive selection and fragmentation of specific product ions. Franceski et al. [94] used Q-IT tandem mass spectrometer, combining the advantages of both analyzers, for the determination of fluoxetine and its metabolite norfluoxetine. A time-of-flight (TOF) mass analyzer was used for fragmentation pathway elucidation of some TCAs [58] and sertraline [62], structural elucidation of bupropion metabolites in urine [45], and fluoxetine quantitation [95]. TOF analyzers allow accurate mass measurement with an assignation of four decimal digits, which dramatically reduces the possible elemental formula of the detected analyte; however, TOF is more expensive and has a narrower linear dynamic range than that achieved with Q and, therefore, the later is preferable for quantitative analysis of target analytes.
5 LC-MS Applications for Antidepressant Quantitative Analysis
Quantitative LC-MS analysis is usually performed by selection of the pseudomolecular ion of the analyte of interest in the selected ion monitoring (SIM) mode. In single quadrupole instruments, selection of fragment ions (m/z) is also possible by promoting collision induced dissociation (CID) reactions in the entrance to the mass spectrometer. Tandem LC-MS/MS instruments enhance selectivity and signal-to-noise ratio compared to single quadrupole instruments by operating on multiple reaction monitoring (MRM) mode. In MRM mode, specific precursor-to-product ion transitions can be monitored by fragmentation of the analyte in the collision cell located between the two analyzers, and subsequently monitoring a selected fragment. According to the European Commission Decision 2002/657/EC [96], quantitative LC-MS(MS) methods for confirmation purposes should include a minimum number of fragments (m/z) or precursor-to-product ion transitions, which depends on the resolution of the mass analyzer. For low resolution analyzers, at least the parent ion (m/z) and two fragments (m/z) in SIM mode, or two precursor-to-product ions transitions in MRM mode, should be monitored.
Quantitative analytical methods should be validated in order to guarantee the quality, accuracy, and precision of the results. This is especially important in forensic and clinical toxicology, where the correct interpretation of the toxicological findings depends on the reliability of the analytical method. Minimum parameters that should be validated in quantitative procedures include selectivity, calibration model, lower limit of quantification (LLOQ), precision (repeatability and intermediate precision), accuracy (bias), and stability. If the method is applied to specimens where the analyte(s) concentration(s) is above the validated range, dilution integrity evaluation should also be included in the validation process. In addition to these parameters, in LC-MS methods it is essential to assess suppression or enhancement of the analyte signal due to matrix effects. Additional parameters that might be evaluated are recovery, limit of detection (LOD), reproducibility, and robustness. A review on validation experiments and acceptance criteria for LC-MS analysis has been published by Peters et al. [29, 97].
Another requirement for qualitative or quantitative analysis is the use of internal standards (IS) to compensate for sample preparation or chromatographic variability. This is of particular importance in LC-MS analysis, as an adequate IS can also compensate for the negative influence of matrix effects on method precision and accuracy. Stable-isotope-labeled ISs are the most appropriate for this purpose. If a specific deuterated analogue is not commercially available, it could be substituted for deuterated substances with similar physicochemical properties to the analyte of interest. However, the use of other marketed pharmaceuticals for this purpose should be avoided, as it cannot be excluded that the patient to be monitored has taken that drug.
LC-MS(MS) quantitative methods for antidepressant determination should fulfill special requirements regarding linearity range, LLOQ or the need for high throughput, depending on the specific application for which they were developed. Conditions and studied validation parameters for selected LC-MS(MS) methodologies for antidepressant determination are shown in Table 1.
Several LC-MS and LC-MS/MS methods were developed in plasma for only one antidepressant and, sometimes, its major metabolite(s) to perform pharmacokinetic, bioavailability, or bioequivalence studies. Analytical methods developed for these purposes require very low LLOQ values and, usually, narrow linear ranges covering the low range of the therapeutic concentrations are validated. In this context, several methodologies were described for the determination of fluoxetine [94, 95, 98–100], paroxetine [44, 71, 85, 101, 102], venlafaxine [48, 61, 64, 86, 103, 104], sertraline [62, 68, 83], citalopram [46, 89] and escitalopram [105], mianserine [106, 107], mirtazapine [42], trazodone [84], nefazodone [51, 81], duloxetine [47, 50, 73], and bupropion [43]. Deuterated analogues of the analyte of interest or of other drugs were employed by few authors as IS [43, 61, 73, 81, 85, 99]; however, in most of these methods, another antidepressant or other therapeutic drug was used for this purpose. Although it is not recommended, the use of commercially available pharmaceuticals as IS could be only justified if the method is applied to a controlled administration study in which the presence of that IS in the biological matrix can be ruled out.
Analytical methods for TDM should cover therapeutic ranges, and LLOQ requirements are not as low as those for pharmacokinetic applications. LC-MS methodologies for the determination of one specific antidepressant could also be applied in these cases. However, as previously stated in this chapter, multianalyte procedures are preferable because they are simpler, faster, cheaper, and allow for the determination of several analytes using the same sample aliquot. Moreover, multianalyte procedures are not only useful, but also required in clinical or forensic applications, where the target antidepressant is initially unknown, and several of them could be involved in the intoxication.
LC-MS(MS) methods including several antidepressants will be described in more detail. Some of these methods include analytes belonging to the same antidepressant group. Alves et al. [80] developed an LC-MS method for the determination of some TCAs in plasma with a total run time of 18 min. Kollroser et al. described two LC-IT-MS procedures in plasma for the determination of seven TCAs [74] and three SSRIs [75], respectively, using an online preparative column. Total analysis time per sample was 12 and 6 min, respectively. The main disadvantage of these methods is that a therapeutic drug was used as IS, hindering its applicability to TDM or clinical and forensic toxicology analysis. Also Juan et al. [66] used fluvoxamine as IS for the determination of several SSRIs; however, the authors argue that this drug was not commercially available in their region, and that patients’ history was studied in order to exclude fluvoxamine intake. Breaud et al. [78] developed a LC-MS/MS method for two TCAs and their main metabolites by turbulent flow LC-MS/MS, which allowed analyte determination from only 10 μL of plasma, with a total analysis time of 3.5 min from the second injection. Zhang et al. [58] used a LC-TOF-MS instrument for accurate mass measurement of TCAs in 18 s, using reference standards and plasma samples fortified with these analytes; however, validated linearity ranges were below the upper therapeutic concentrations and, therefore, evaluation of dilution integrity would be needed in order to analyze specimens from patients on antidepressant treatment or from intoxication cases. More details on validation experiments performed in these methods are shown in Table 1.
Other authors described LC-MS or LC-MS/MS methods in serum, plasma or whole blood for the determination of several analytes belonging to different antidepressant groups. LC-MS methods were developed by Halvorsen et al. [65] and Gutteck et al. [108] using an ion trap and a single quadrupole mass analyzer, respectively, with chromatographic elution of the analytes included in each method within 10 min. Analytes included in Gutteck’s et al. method were divided in four groups depending on their therapeutic ranges, and slightly different extraction and chromatographic procedures were applied to each group. Shinozuka et al. [69] extended the number of antidepressants using a LC-IT-MS instrument, and chromatographic separation was performed in 30 min. Tandem LC-MS/MS instruments were also employed in several occasions [53, 59, 60, 72, 77, 109]. Kirchherr et al. [53] employed protein precipitation of 0.1 mL of serum for the determination of 48 psycotherapeutics, including the most common antidepressants, with a total chromatographic run of 8 min. Also Remane et al. [59] developed a multianalyte procedure for the determination of 136 analytes from different drug classes using a generic LLE procedure; however, only matrix effect, recovery, and process efficiency were evaluated for method validation. Santos-Neto et al. [77] developed a LC-MS/MS method for the analysis of some antidepressants in plasma and urine using a monolithic column for simultaneous online sample preparation and chromatographic separation, with a total analysis time of 8 min. Sauvage et al. [76] extended the number of antidepressants determined in 0.1 mL of serum using turbulent flow LC-MS/MS, and decreased the total analysis time to 6 min. De Castro et al. [72] developed an online SPE-LC-MSMS procedure using 0.05 mL of plasma, where the complete analytical process for the determination of nine antidepressants was performed in 20 min. Table 1 shows the parameters evaluated for method validation, as well as analytes employed as IS, in each of these methods.
Although most LC-MS(MS) methods for antidepressants were applied to plasma, serum, or whole blood specimens, some analytical methodologies were also described in other biological matrices. Petsalo et al. [45] identified 20 bupropion metabolites in urine by accurate mass measurement using a LC-TOF-MS instrument. De Santana [42] applied a LC-MS/MS method with SPME extraction to urine samples to assess cumulative urinary excretion of mirtazapine and two metabolites. LC-MS/MS methods were also developed to compare enantiomers disposition of reboxetine [110], and bupropion and its metabolite [43] in plasma and urine specimens. Bupropion and some metabolites were also determined in urine by LC-MS/MS in a fatal overdose case where this antidepressant was involved [70]. LC-MS/MS was also applied to the analysis of other typical postmortem specimens, including gastric content, bile, vitreous humor, cerebrospinal fluid, brain, liver, lungs, kidney, or muscle, usually for the determination of one antidepressant and its main metabolite [38–40]. Goeringer et al. [57] extended the number of analytes included in the method to seven antidepressants, some metabolites and one antipsychotic in different forensic specimens. Unfortunately, validation performed in most of these methods was poor and, sometimes, only described for some of the analyzed specimens.
Few authors described antidepressant analysis in alternative specimens, such as hair or oral fluid. LC-CID-MS and MS/MS mass spectra libraries for identification of several drugs were employed by Müller et al. [32] for the detection of maprotiline, citalopram, and their desmethyl metabolites in authentic hair specimens; extracted ions chromatograms were employed for subsequent antidepressant quantification. Also Klys et al. [33] applied LC-MS/MS to the analysis of blood, urine, and hair specimens in a fatal case due to clomipramine overdose in combination with alcohol. Blood clomipramine and norclomipramine concentrations explained the fatal outcome, and hair analysis confirmed that the deceased was on clomipramine treatment for, at least, 12 months prior to his death. With regard to oral fluid analysis, de Castro et al. [34] developed and validated a LC-MS/MS procedure for the determination of the main marketed antidepressants in plasma and oral fluid to assess the possible correlation between the concentrations found in these two biological matrices. Also Coulter et al. [35] validated a LC-MS/MS methodology for several antidepressants and two other psychopharmaceuticals in oral fluid for its application to driving under the influence of drugs (DUID) cases.
6 LC-MS/MS Method for the Determination of Nine Antidepressants and Some of their Main Metabolites in Oral Fluid and Plasma
An LC-MS/MS method [34] will be described in detail in order to serve as an example of method development and validation. This method allows the determination of some of the most common antidepressants used in clinical practice and some of their main metabolites in oral fluid and plasma samples.
Plasma is the main biological sample used in clinical and toxicological analysis, as concentrations found in this matrix are correlated to the pharmacological effect, as well as to the side and toxic effects. However, oral fluid has also been employed in some specific applications because of the advantages associated to this alternative specimen: easy, painless, and noninvasive collection, which does not require qualified personnel, it represents the free analyte fraction, and it has a window of detection similar to that in plasma. Within the possible applications of oral fluid analysis, two are of special relevance:
-
1.
Detection of subjects driving under the influence of sedative antidepressants effects.
-
2.
TDM: As previously stated in this chapter, TDM is recommended for TCAs and, in special situations, for the new generations of antidepressants. However, several factors can affect diffusion of the analytes from plasma to oral fluid (pH, oral contamination, collection with or without stimulation). Therefore, the correlation between antidepressant plasma and oral fluid concentrations should be studied before using this alternative specimen for TDM purposes.
An example of method application to a study to assess the possible correlations between antidepressant concentrations in plasma and oral fluid will also be discussed in this section.
6.1 LC-MS/MS Method
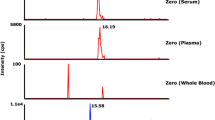
A Waters Alliance 2795 Separation Module with a Waters Alliance series column/heater (Waters Corp., Milford, MA) was employed, using a Sunfire C18 (20 mm × 2.1 mm, 3.5 μm) Intelligent Speed™ column (Waters Corp., Milford, MA) for chromatographic separation at 26 °C. Mobile phase was ammonium formate buffer (pH 3.0; 2 mM) and ACN at a flow rate of 0.4 mL/min, applying the following gradient: 15% ACN for 0.5 min, increased to 50% over 3.5 min, and increased again to 70% at minute 5. With these conditions, all compounds eluted within 5 min, with a total run time of 8 min. Figure 2 shows the chromatograms of the 13 antidepressants in oral fluid at the LLOQ (2 ng/mL).

Chromatograms of the quantitative transitions for the 13 antidepressants included in the LC-MS/MS method in oral fluid at the LLOQ (2 ng/mL) (Source: From de Castro A et al. (2008) J Pharm Biomed Anal. 48:183. With permission)
For the detection, a tandem mass spectrometer Quattro Micro™ API ESCI (Waters Corp., Milford, MA) with a triple quadrupole was employed. The instrument was operated in electrospray in the positive ionization mode (ESI+) with the following optimized parameters: capillary voltage, 0.5 kV; source block temperature, 130 °C; nebulization and desolvation gas (nitrogen) heated at 400 °C and delivered at 800 L/h, and as cone gas at 50 L/h; collision cell pressure, 3 × 10–6 bar (argon). Data was recorded in the multiple reaction monitoring (MRM) mode by selection of the two most intense precursor-to-product ion transitions for each analyte, except for the ISs, for which only one transition was monitored. The most intense transition for each analyte was used for quantitative purposes. Table 2 shows MRM transitions, cone voltages and collision energies used for the analysis of the antidepressants included in the LC-MS/MS method.
6.2 Oral Fluid and Plasma Extraction Procedure
Solid phase extraction (SPE) was performed with an ASPEC XL automated system (Gilson, Middletown, USA) and mixed mode OASIS MCX cartridges 60 mg 3 cm3 (Waters Corp., Milford, USA). Before SPE, 1 mL of sodium acetate buffer pH 3.6 and 50 μL of IS mixture (nortriptyline-d3, clomipramine-d3, paroxetine-d6, norfluoxetine-d6, and fluoxetine-d6) at 0.2 mg/L in oral fluid and 0.4 mg/L in plasma were added to 0.2 mL of sample. The applied SPE procedure is summarized in Fig. 3.

Solid-phase extraction (SPE) procedure applied to plasma and oral fluid samples for LC-MS/MS determination of nine antidepressants and some metabolites
6.3 Method Validation
LC-MS/MS method validation was performed as follows:
6.3.1 Selectivity
Selectivity of the method was evaluated by analysis of blank oral fluid and plasma specimens from ten healthy subjects. In addition, potential exogenous interferences were assessed by analysis of authentic plasma specimens containing other common therapeutic drugs like benzodiazepines and/or drugs of abuse. No endogenous or exogenous interferences were found in the monitored MRM channels in any of the analyzed specimens.
6.3.2 Calibration Model
Calibration curves (n = 6, six different days) were generated at eight concentration levels in the range from 2 to 500 ng/mL and 2–1,000 ng/mL for oral fluid and plasma, respectively. Coefficient of determination (r 2) was >0.99 for all analytes using a 1/x weighted linear regression, except for fluvoxamine, for which a quadratic response was observed.
6.3.3 Limit of Detection (LOD) and Limit of Quantification (LLOQ)
LOD was defined as the lowest concentration for which the two monitored transitions could be detected, and the peak area of the quantifier transition was, at least, three times the background noise. LOD was 0.5 ng/mL for all analytes. LLOQ was defined as the lowest concentration that could be quantified with appropriate imprecision (coefficient of variation (%CV) <20%) and inaccuracy (mean relative error (MRE) ± 20%). LLOQ was 2 ng/mL in oral fluid, and 2–4 ng/mL in plasma for most of the analytes. Carryover after automated SPE of clomipramine at 1,000 ng/mL was half of the signal obtained at 2 ng/mL; therefore, LLOQ in plasma was increased to 10 ng/mL for this analyte.
6.3.4 Intra- and Interday Imprecision and Inaccuracy
Intraday imprecision and inaccuracy were evaluated at low, medium and high concentrations within the validated concentration ranges for each matrix by analysis of five replicates on the same day. Interday imprecision and inaccuracy were assessed by analysis of five replicates at the same concentrations on five different days. MRE was ±15% and %CV <17% in all cases.
6.3.5 Relative Ions Intensity
Intraday imprecision of relative ions intensity for each analyte was evaluated by analysis of five replicates at four concentration levels analyzed on the same day, and interday imprecision on this parameter was calculated at the same concentration levels (n = 5 each) analyzed on five different days. %CV for the relative ions intensities was <17% in all cases, except for norfluoxetine, for which %CV was <26%.
6.3.6 Extraction Recovery
Extraction recovery was assessed at low and high concentrations by comparing analyte-to-IS peak area ratio when standards were added before extraction (n = 5) to that obtained when added after extraction (n = 5). IS mixture was added after extraction in all cases. Recoveries ranged from 49 to 72 % for all analytes.
6.3.7 Matrix Effect
Matrix effect was initially evaluated by postcolumn infusion of a mixture containing the analytes and the ISs (1 μg/mL, 10 μL/min) in “T” with the effluent of the chromatographic system. Chromatograms after the injection of extracted blank plasma (n = 6) and oral fluid samples (n = 6) from different sources were compared with the chromatograms after the injection of mobile phase (no matrix effect). Quantification of matrix effect was performed comparing average peak areas of blank plasma (n = 6) and oral fluid samples (n = 6) fortified with the analytes (100 ng/mL) and ISs after extraction to those obtained when the same amount of analytes and ISs were added to a clean tube, evaporated and reconstituted in mobile phase. Matrix effect was <15% for all analytes, except for norfluoxetine (signal enhancement <45%) and paroxetine (signal enhancement <30%). Nevertheless, inclusion of the deuterated analogues for these two analytes compensate for the possible errors in imprecision, inaccuracy and recovery.
6.3.8 Stability Study
Antidepressant stability after three freeze–thaw cycles was evaluated in triplicate at low and high concentrations. Calculated concentrations in the samples subjected to these conditions (stability samples) were compared to those obtained in freshly prepared samples (control samples). Stability and control samples were quantified with a calibration curve prepared on the day of the analysis. All analytes were stable under these conditions, except sertraline, for which a slight signal decrease was observed at 250 ng/mL in oral fluid (MRE = −33.4%; %CV = 6.0%).
6.4 Oral Fluid-Plasma Preliminary Correlation Study
Initially, plasma and oral fluid specimens from patients (n = 21) on different antidepressant treatment were collected twice to assess if any of the studied analytes was likely to show a good correlation. The best results were obtained for venlafaxine (%CV for plasma/oral fluid concentrations ratio (R OF/PL) <27%). Therefore, the study was extended for this antidepressant by analysis of oral fluid and plasma specimens from five patients on venlafaxine treatment collected on four occasions. Daily doses of venlafaxine retard formulations were 75 mg for two patients, and 150 mg for the remaining participants. Collection of oral fluid (direct spitting into polypropylene tubes) and plasma (heparinized tubes) specimens was performed, when possible, before the next dose to ensure the drug was in the elimination phase. The dose and the time of collection was the same on the four different occasions for each patient. For the analysis, oral fluid and plasma specimens were centrifuged at 14 × 103 rpm, and 0.2 mL of the supernatant were extracted. In addition, correlation between the concentrations in the plasmatic free fraction and in oral fluid was also evaluated. Plasmatic proteins were eliminated by filtering 0.5 mL of plasma samples using Microcon filter devices Ultracel YM-3 (Millipore Corp., Billerica, MA, USA).
Table 3 shows plasmatic and oral fluid concentrations, ratios between those concentrations and calculated coefficients of determination for the five participants on venlafaxine treatment. Results were not analyzed interindividually due to the low number of patients and differences in the daily dosage. As expected, oral fluid concentrations were higher than those found in plasma in all cases. This is explained by venlafaxine’s weak basic properties, which favors oral fluid accumulation due to the slightly lower pH of this matrix compared to that in plasma. Intraindividually, plasmatic concentrations (C PL) were similar in the four analyzed specimens, but higher variability was found in oral fluid (C OF). Also, a great variability was observed in plasmatic free fraction concentrations (C PL-FF), which could be favored by some retention of the analytes in the filter used to eliminate the plasmatic proteins. Correlation between C OF vs. C PL or C PL-FF on the four different days was analyzed by linear regression. Only r 2 values for one patient were >0.6; therefore, our data indicates that a correlation between venlafaxine concentrations in oral fluid and plasma or the plasmatic free fraction is unlikely. Nevertheless, a strong conclusion would require the extension of the study, including a higher number of patients on the same daily dose, collecting more samples from each patient, and standardizing the interval time between drug administration and sample collection. Although our data do not support oral fluid analysis for antidepressant TDM, this alternative matrix could be employed in special situations to assess patients’ noncompliance or to detect impaired drivers under antidepressant influence.
References
Drasch G, Dahlmann F, von Meyer L et al (2008) Frequency of different anti-depressants associated with suicides and drug deaths. Int J Legal Med 122:115–121
Jonsson A, Holmgren P, Ahlner J (2004) Fatal intoxications in a Swedish forensic autopsy material during 1992–2002. Forensic Sci Int 143:53–59
Ohberg A, Vuori E, Klaukka T et al (1998) Antidepressants and suicide mortality. J Affect Disord 50:225–233
Shields LB, Hunsaker DM, Hunsaker JC III et al (2006) Toxicologic findings in suicide: a 10-year retrospective review of Kentucky medical examiner cases. Am J Forensic Med Pathol 27:106–112
Jones G, Singer P (2001) Miscellaneous prescription and over-the-counter medications. In: LeBeau M, Mozayani A (eds) Drug-facilitated sexual assault. A forensic handbook, 1st edn. Academic Press, San Diego, CA
Verster JC, Mets MA (2009) Psychoactive medication and traffic safety. Int J Environ Res Public Health 6:1041–1054
Brunnauer A, Laux G, Geiger E et al (2006) Antidepressants and driving ability: results from a clinical study. J Clin Psychiatry 67:1776–1781
Ramaekers JG (2003) Antidepressants and driver impairment: empirical evidence from a standard on-the-road test. J Clin Psychiatry 64:20–29
Walsh JM, Verstraete AG, Huestis MA et al (2008) Guidelines for research on drugged driving. Addiction 103:1258–1268
Mann K, Hiemke C, Schmidt LG et al (2006) Appropriateness of therapeutic drug monitoring for antidepressants in routine psychiatric inpatient care. Ther Drug Monit 28:83–88
Mitchell PB (2004) Therapeutic drug monitoring of non-tricyclic antidepressant drugs. Clin Chem Lab Med 42:1212–1218
Lundmark J, Bengtsson F, Nordin C et al (2000) Therapeutic drug monitoring of selective serotonin reuptake inhibitors influences clinical dosing strategies and reduces drug costs in depressed elderly patients. Acta Psychiatr Scand 101:354–359
Burke MJ, Preskorn SH (1999) Therapeutic drug monitoring of antidepressants: cost implications and relevance to clinical practice. Clin Pharmacokinet 37:147–165
Hackett LP, Dusci LJ, Ilett KF (1998) A comparison of high-performance liquid chromatography and fluorescence polarization immunoassay for therapeutic drug monitoring of tricyclic antidepressants. Ther Drug Monit 20:30–34
Meenan GM, Barlotta S, Lehrer M (1990) Urinary tricyclic antidepressant screening: comparison of results obtained with Abbott FPIA reagents and Syva EIA reagents. J Anal Toxicol 14:273–276
Asselin WM, Leslie JM (1990) Use of the EMITtox serum tricyclic antidepressant assay for the analysis of urine samples. J Anal Toxicol 14:168–171
Banger M, Hermes B, Hartter S et al (1997) Monitoring serum concentrations of clomipramine and metabolites: fluorescence polarization immunoassay versus high performance liquid chromatography. Pharmacopsychiatry 30:128–132
Benitez J, Dahlqvist R, Gustafsson LL et al (1986) Clinical pharmacological evaluation of an assay kit for intoxications with tricyclic antidepressants. Ther Drug Monit 8:102–105
Yuan CM, Spandorfer PR, Miller SL et al (2003) Evaluation of tricyclic antidepressant false positivity in a pediatric case of cyproheptadine (periactin) overdose. Ther Drug Monit 25:299–304
Caravati EM, Juenke JM, Crouch BI et al (2005) Quetiapine cross-reactivity with plasma tricyclic antidepressant immunoassays. Ann Pharmacother 39:1446–1449
Maurer HH, Bickeboeller-Friedrich J (2000) Screening procedure for detection of antidepressants of the selective serotonin reuptake inhibitor type and their metabolites in urine as part of a modified systematic toxicological analysis procedure using gas chromatography-mass spectrometry. J Anal Toxicol 24:340–347
Lacassie E, Ragot S, Gaulier JM et al (1999) A specific dosage method for the analysis of 24 antidepressants using gas chromatography-mass spectrometry (GC/SM). Acta Clin Belg Suppl 1:20–24
Way BA, Stickle D, Mitchell ME et al (1998) Isotope dilution gas chromatographic-mass spectrometric measurement of tricyclic antidepressant drugs. Utility of the 4-carbethoxyhexafluorobutyryl derivatives of secondary amines. J Anal Toxicol 22:374–382
Salgado-Petinal C, Lamas JP, Garcia-Jares C et al (2005) Rapid screening of selective serotonin re-uptake inhibitors in urine samples using solid-phase microextraction gas chromatography-mass spectrometry. Anal Bioanal Chem 382:1351–1359
Eap CB, Bouchoux G, Amey M et al (1998) Simultaneous determination of human plasma levels of citalopram, paroxetine, sertraline, and their metabolites by gas chromatography-mass spectrometry. J Chromatogr Sci 36:365–371
Matuszewski BK, Constanzer ML, Chavez-Eng CM (2003) Strategies for the assessment of matrix effect in quantitative bioanalytical methods based on HPLC-MS/MS. Anal Chem 75:3019–3030
Annesley TM (2003) Ion suppression in mass spectrometry. Clin Chem 49:1041–1044
Taylor PJ (2005) Matrix effects: the Achilles heel of quantitative high-performance liquid chromatography-electrospray-tandem mass spectrometry. Clin Biochem 38:328–334
Peters FT, Drummer OH, Musshoff F (2007) Validation of new methods. Forensic Sci Int 165:216–224
Thieme D, Rolf B, Sachs H et al (2008) Correlation of inter-individual variations of amitriptyline metabolism examined in hairs with CYP2C19 and CYP2D6 polymorphisms. Int J Legal Med 122:149–155
Smyth WF, Leslie JC, McClean S et al (2006) The characterisation of selected antidepressant drugs using electrospray ionisation with ion trap mass spectrometry and with quadrupole time-of-flight mass spectrometry and their determination by high-performance liquid chromatography/electrospray ionisation tandem mass spectrometry. Rapid Commun Mass Spectrom 20:1637–1642
Muller C, Vogt S, Goerke R et al (2000) Identification of selected psychopharmaceuticals and their metabolites in hair by LC/ESI-CID/MS and LC/MS/MS. Forensic Sci Int 113:415–421
Klys M, Scislowski M, Rojek S et al (2005) A fatal clomipramine intoxication case of a chronic alcoholic patient: application of postmortem hair analysis method of clomipramine and ethyl glucuronide using LC/APCI/MS. Leg Med (Tokyo) 7:319–325
de Castro A, Concheiro M, Quintela O et al (2008) LC-MS/MS method for the determination of nine antidepressants and some of their main metabolites in oral fluid and plasma. Study of correlation between venlafaxine concentrations in both matrices. J Pharm Biomed Anal 48:183–193
Coulter C, Taruc M, Tuyay J et al (2010) Antidepressant drugs in oral fluid using liquid chromatography-tandem mass spectrometry. J Anal Toxicol 34:64–72
Lobo ED, Loghin C, Knadler MP et al (2008) Pharmacokinetics of duloxetine in breast milk and plasma of healthy postpartum women. Clin Pharmacokinet 47:103–109
Goeringer KE, McIntyre IM, Drummer OH (2001) Postmortem tissue concentrations of venlafaxine. Forensic Sci Int 121:70–75
Avella J, Lehrer M, Katz M et al (2004) Two cases involving clomipramine intoxication. J Anal Toxicol 28:504–508
Gronewold A, Dettling A, Haffner HT et al (2009) Doxepin and nordoxepin concentrations in body fluids and tissues in doxepin associated deaths. Forensic Sci Int 190:74–79
Wenzel S, Aderjan R, Mattern R et al (2006) Tissue distribution of mirtazapine and desmethylmirtazapine in a case of mirtazapine poisoning. Forensic Sci Int 156:229–236
Society of Hair Testing (2004) Consensus on hair analysis. http://www.soht.org/. Accessed 2 Dec 2010
de Santana FJ, Bonato PS (2008) Enantioselective analysis of mirtazapine and its two major metabolites in human plasma by liquid chromatography-mass spectrometry after three-phase liquid-phase microextraction. Anal Chim Acta 606:80–91
Coles R, Kharasch ED (2007) Stereoselective analysis of bupropion and hydroxybupropion in human plasma and urine by LC/MS/MS. J Chromatogr B Anal Technol Biomed Life Sci 857:67–75
Petsalo A, Turpeinen M, Tolonen A (2007) Identification of bupropion urinary metabolites by liquid chromatography/mass spectrometry. Rapid Commun Mass Spectrom 21:2547–2554
Segura M, Ortuno J, Farre M et al (2003) Quantitative determination of paroxetine and its 4-hydroxy-3-methoxy metabolite in plasma by high-performance liquid chromatography/electrospray ion trap mass spectrometry: application to pharmacokinetic studies. Rapid Commun Mass Spectrom 17:1455–1461
Jiang T, Rong Z, Peng L et al (2010) Simultaneous determination of citalopram and its metabolite in human plasma by LC-MS/MS applied to pharmacokinetic study. J Chromatogr B Anal Technol Biomed Life Sci 878:615–619
Ma N, Zhang BK, Li HD et al (2007) Determination of duloxetine in human plasma via LC/MS and subsequent application to a pharmacokinetic study in healthy Chinese volunteers. Clin Chim Acta 380:100–105
Patel BN, Sharma N, Sanyal M et al (2008) Liquid chromatography tandem mass spectrometry assay for the simultaneous determination of venlafaxine and O-desmethylvenlafaxine in human plasma and its application to a bioequivalence study. J Pharm Biomed Anal 47:603–611
Rudberg I, Hermann M, Refsum H et al (2008) Serum concentrations of sertraline and N-desmethyl sertraline in relation to CYP2C19 genotype in psychiatric patients. Eur J Clin Pharmacol 64:1181–1188
Senthamil Selvan P, Gowda KV, Mandal U et al (2007) Determination of duloxetine in human plasma by liquid chromatography with atmospheric pressure ionization-tandem mass spectrometry and its application to pharmacokinetic study. J Chromatogr B Anal Technol Biomed Life Sci 858:269–275
Yao M, Srinivas NR (2000) Simultaneous quantitation of d7-nefazodone, nefazodone, d7-hydroxynefazodone, hydroxynefazodone, m-chlorophenylpiperazine and triazole-dione in human plasma by liquid chromatographic-mass spectrometry. Biomed Chromatogr 14:106–112
Zhao RK, Cheng G, Tang J et al (2009) Pharmacokinetics of duloxetine hydrochloride enteric-coated tablets in healthy Chinese volunteers: a randomized, open-label, single- and multiple-dose study. Clin Ther 31:1022–1036
Kirchherr H, Kuhn-Velten WN (2006) Quantitative determination of forty-eight antidepressants and antipsychotics in human serum by HPLC tandem mass spectrometry: a multi-level, single-sample approach. J Chromatogr B Anal Technol Biomed Life Sci 843:100–113
Dams R, Huestis MA, Lambert WE et al (2003) Matrix effect in bio-analysis of illicit drugs with LC-MS/MS: influence of ionization type, sample preparation, and biofluid. J Am Soc Mass Spectrom 14:1290–1294
Bonfiglio R, King RC, Olah TV et al (1999) The effects of sample preparation methods on the variability of the electrospray ionization response for model drug compounds. Rapid Commun Mass Spectrom 13:1175–1185
Naidong W, Bu H, Chen YL et al (2002) Simultaneous development of six LC-MS-MS methods for the determination of multiple analytes in human plasma. J Pharm Biomed Anal 28:1115–1126
Goeringer KE, McIntyre M, Drummer OH (2003) LC-MS analysis of serotonergic drugs. J Anal Toxicol 27:30–35
Zhang H, Heinig K, Henion J (2000) Atmospheric pressure ionization time-of-flight mass spectrometry coupled with fast liquid chromatography for quantitation and accurate mass measurement of five pharmaceutical drugs in human plasma. J Mass Spectrom 35:423–431
Remane D, Meyer MR, Peters FT et al (2010) Fast and simple procedure for liquid–liquid extraction of 136 analytes from different drug classes for development of a liquid chromatographic-tandem mass spectrometric quantification method in human blood plasma. Anal Bioanal Chem 397:2303–2314
Titier K, Castaing N, Le-Deodic M et al (2007) Quantification of tricyclic antidepressants and monoamine oxidase inhibitors by high-performance liquid chromatography-tandem mass spectrometry in whole blood. J Anal Toxicol 31:200–207
Theron HB, van der Merwe MJ, Swart KJ et al (2007) Employing atmospheric pressure photoionization in liquid chromatography/tandem mass spectrometry to minimize ion suppression and matrix effects for the quantification of venlafaxine and O-desmethylvenlafaxine. Rapid Commun Mass Spectrom 21:1680–1686
Chen X, Duan X, Dai X et al (2006) Development and validation of a liquid chromatographic/tandem mass spectrometric method for the determination of sertraline in human plasma. Rapid Commun Mass Spectrom 20:2483–2489
Djordjevic S, Kovacevic I, Miljkovic B et al (2005) Liquid chromatographic-mass spectrometric method for the determination of fluoxetine and norfluoxetine in human plasma: application to clinical study. Farmaco 60:345–349
Liu W, Cai HL, Li HD (2007) High performance liquid chromatography-electrospray ionization mass spectrometry (HPLC-MS/ESI) method for simultaneous determination of venlafaxine and its three metabolites in human plasma. J Chromatogr B Anal Technol Biomed Life Sci 850:405–411
Halvorsen TG, Pedersen-Bjergaard S, Reubsaet JLE et al (2003) Liquid-phase microextraction combined with liquid chromatography-mass spectrometry. Extraction from small volumes of biological samples. J Sep Sci 26:1520–1526
Juan H, Zhiling Z, Huande L (2005) Simultaneous determination of fluoxetine, citalopram, paroxetine, venlafaxine in plasma by high performance liquid chromatography-electrospray ionization mass spectrometry (HPLC-MS/ESI). J Chromatogr B Anal Technol Biomed Life Sci 820:33–39
Bhatt J, Jangid A, Venkatesh G et al (2005) Liquid chromatography-tandem mass spectrometry (LC-MS-MS) method for simultaneous determination of venlafaxine and its active metabolite O-desmethyl venlafaxine in human plasma. J Chromatogr B Anal Technol Biomed Life Sci 829:75–81
Jain DS, Sanyal M, Subbaiah G et al (2005) Rapid and sensitive method for the determination of sertraline in human plasma using liquid chromatography-tandem mass spectrometry (LC-MS/MS). J Chromatogr B Anal Technol Biomed Life Sci 829:69–74
Shinozuka T, Terada M, Tanaka E (2006) Solid-phase extraction and analysis of 20 antidepressant drugs in human plasma by LC/MS with SSI method. Forensic Sci Int 162:108–112
Mercerolle M, Denooz R, Lachatre G et al (2008) A fatal case of bupropion (Zyban) overdose. J Anal Toxicol 32:192–196
Bhatt M, Shah S, Shivprakash (2010) Solid-phase extraction and analysis of paroxetine in human plasma by ultra performance liquid chromatography-electrospray ionization mass spectrometry. Biomed Chromatogr 24:209–215
De Castro A, Ramírez Fernandez MM, Laloup M, Samyn N, De Boeck G, Wood M, Maes V, López-Rivadulla M (2007) High-throughput on-line solid-phase extraction-liquid chromatography-tandem mass spectrometry method for the simultaneous analysis of 14 antidepressants and their metabolites in plasma. J Chromatogr A 1160:3–12
Satonin DK, McCulloch JD, Kuo F et al (2007) Development and validation of a liquid chromatography-tandem mass spectrometric method for the determination of the major metabolites of duloxetine in human plasma. J Chromatogr B Anal Technol Biomed Life Sci 852:582–589
Kollroser M, Schober C (2002) Simultaneous determination of seven tricyclic antidepressant drugs in human plasma by direct-injection HPLC-APCI-MS-MS with an ion trap detector. Ther Drug Monit 24:537–544
Kollroser M, Schober C (2003) An on-line solid phase extraction liquid chromatography tandem mass spectrometry method for the analysis of citalopram, fluvoxamine and paroxetine in human plasma. Chromatographia 57:133–138
Sauvage FL, Gaulier JM, Lachatre G et al (2006) A fully automated turbulent-flow liquid chromatography-tandem mass spectrometry technique for monitoring antidepressants in human serum. Ther Drug Monit 28:123–130
Santos-Neto AJ, Bergquist J, Lancas FM et al (2008) Simultaneous analysis of five antidepressant drugs using direct injection of biofluids in a capillary restricted-access media-liquid chromatography-tandem mass spectrometry system. J Chromatogr A 1189:514–522
Breaud AR, Harlan R, Di Bussolo JM et al (2010) A rapid and fully-automated method for the quantitation of tricyclic antidepressants in serum using turbulent-flow liquid chromatography-tandem mass spectrometry. Clin Chim Acta 411:825–832
Queiroz ME, Oliveira EB, Breton F et al (2007) Immunoaffinity in-tube solid phase microextraction coupled with liquid chromatography-mass spectrometry for analysis of fluoxetine in serum samples. J Chromatogr A 1174:72–77
Alves C, Santos-Neto AJ, Fernandes C et al (2007) Analysis of tricyclic antidepressant drugs in plasma by means of solid-phase microextraction-liquid chromatography-mass spectrometry. J Mass Spectrom 42:1342–1347
Mao Y, Huang MQ, Xia YQ et al (2007) High-throughput quantitation of nefazodone and its metabolites in human plasma by high flow direct-injection LC-MS/MS. J Pharm Biomed Anal 43:1808–1819
Liu W, Wang F, Li HD (2007) Simultaneous stereoselective analysis of venlafaxine and O-desmethylvenlafaxine enantiomers in human plasma by HPLC-ESI/MS using a vancomycin chiral column. J Chromatogr B Anal Technol Biomed Life Sci 850:183–189
Patel BN, Sharma N, Sanyal M et al (2009) Analysis of second-generation antidepressant drug, sertraline and its active metabolite, N-desmethyl sertraline in human plasma by a sensitive and selective liquid chromatography-tandem mass spectrometry method. J Chromatogr B Anal Technol Biomed Life Sci 877:221–229
Patel BN, Sharma N, Sanyal M et al (2008) High throughput and sensitive determination of trazodone and its primary metabolite, m-chlorophenylpiperazine, in human plasma by liquid chromatography-tandem mass spectrometry. J Chromatogr B Anal Technol Biomed Life Sci 871:44–54
Naidong W, Eerkes A (2004) Development and validation of a hydrophilic interaction liquid chromatography-tandem mass spectrometric method for the analysis of paroxetine in human plasma. Biomed Chromatogr 18:28–36
Wei Z, Bing-Ren X, Cai-Yun W (2007) Liquid chromatography-mass spectrometry method for the determination of venlafaxine in human plasma and application to a pharmacokinetic study. Biomed Chromatogr 21:266–272
Choong E, Rudaz S, Kottelat A et al (2009) Therapeutic drug monitoring of seven psychotropic drugs and four metabolites in human plasma by HPLC-MS. J Pharm Biomed Anal 50:1000–1008
Shen Z, Wang S, Bakhtiar R (2002) Enantiomeric separation and quantification of fluoxetine (Prozac) in human plasma by liquid chromatography/tandem mass spectrometry using liquid-liquid extraction in 96-well plate format. Rapid Commun Mass Spectrom 16:332–338
Rocha A, Marques MP, Coelho EB et al (2007) Enantioselective analysis of citalopram and demethylcitalopram in human and rat plasma by chiral LC-MS/MS: application to pharmacokinetics. Chirality 19:793–801
Arpino P, Baldwin MA, McLafferty FW (1974) Liquid chromatography-mass spectrometry. II. Continuous monitoring. Biomed Mass Spectrom 1:80–82
Niessen WMA (1999) History of LC-MS. In: Niessen WMA (ed) Liquid chromatography-mass spectrometry, 2nd edn. Marcel Dekker, Inc., New York
King R, Bonfiglio R, Fernandez-Metzler C et al (2000) Mechanistic investigation of ionization suppression in electrospray ionization. J Am Soc Mass Spectrom 11:942–950
Smeraglia J, Baldrey SF, Watson D (2001) Matrix effects and selectivity issues in LC-MS-MS. Chromatographia 55:S95–S99
Franceschi L, Faggiani A, Furlanut M (2009) A simple method to monitor serum concentrations of fluoxetine and its major metabolite for pharmacokinetic studies. J Pharm Biomed Anal 49:554–557
Saber AL (2009) On-line solid phase extraction coupled to capillary LC-ESI-MS for determination of fluoxetine in human blood plasma. Talanta 78:295–299
European Union Decision 2002/657/EC (17/8/2002) (2002) Off J Eur Commun 221:8–36
Peters FT (2006) Method validation using LC-MS. In: Polettini A (ed) Applications of LC-MS in toxicology, 1st edn. Pharmaceutical, London
Moraes MO, Lerner FE, Corso G et al (1999) Fluoxetine bioequivalence study: quantification of fluoxetine and norfluoxetine by liquid chromatography coupled to mass spectrometry. J Clin Pharmacol 39:1053–1061
Li C, Ji Z, Nan F et al (2002) Liquid chromatography/tandem mass spectrometry for the determination of fluoxetine and its main active metabolite norfluoxetine in human plasma with deuterated fluoxetine as internal standard. Rapid Commun Mass Spectrom 16:1844–1850
Sutherland FC, Badenhorst D, de Jager AD et al (2001) Sensitive liquid chromatographic-tandem mass spectrometric method for the determination of fluoxetine and its primary active metabolite norfluoxetine in human plasma. J Chromatogr A 914:45–51
Massaroti P, Cassiano NM, Duarte LF et al (2005) Validation of a selective method for determination of paroxetine in human plasma by LC-MS/MS. J Pharm Pharm Sci 8:340–347
Zhu Z, Neirinck L (2002) High-performance liquid chromatography-mass spectrometry method for the determination of paroxetine in human plasma. J Chromatogr B Anal Technol Biomed Life Sci 780:295–300
Qin F, Li N, Qin T et al (2010) Simultaneous quantification of venlafaxine and O-desmethylvenlafaxine in human plasma by ultra performance liquid chromatography-tandem mass spectrometry and its application in a pharmacokinetic study. J Chromatogr B Anal Technol Biomed Life Sci 878:689–694
Rajasekhar D, Kumar IJ, Venkateswarlu P (2009) Rapid high-performance liquid chromatography-tandem mass spectrometry method for simultaneous measurement of venlafaxine and O-desmethylvenlafaxine in human plasma and its application in comparative bioavailability study. Biomed Chromatogr 23:1300–1307
Singh SS, Shah H, Gupta S et al (2004) Liquid chromatography-electrospray ionisation mass spectrometry method for the determination of escitalopram in human plasma and its application in bioequivalence study. J Chromatogr B Anal Technol Biomed Life Sci 811:209–215
Xu P, Li HD, Chen BM et al (2008) Determination of mianserin in human plasma by high performance liquid chromatography-electrospray ionization mass spectrometry (HPLC-ESI/MS): application to a bioequivalence study in Chinese volunteers. J Pharm Biomed Anal 47:994–999
Chauhan B, Rani S, Guttikar S et al (2005) Analytical method development and validation of mianserin hydrochloride and its metabolite in human plasma by LC-MS. J Chromatogr B Anal Technol Biomed Life Sci 823:69–74
Gutteck U, Rentsch KM (2003) Therapeutic drug monitoring of 13 antidepressant and five neuroleptic drugs in serum with liquid chromatography-electrospray ionization mass spectrometry. Clin Chem Lab Med 41:1571–1579
Castaing N, Titier K, Receveur-Daurel M et al (2007) Quantification of eight new antidepressants and five of their active metabolites in whole blood by high-performance liquid chromatography-tandem mass spectrometry. J Anal Toxicol 31:334–341
Fleishaker JC, Mucci M, Pellizzoni C et al (1999) Absolute bioavailability of reboxetine enantiomers and effect of gender on pharmacokinetics. Biopharm Drug Dispos 20:53–57
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2012 Springer Science+Business Media, LLC
About this chapter
Cite this chapter
de Castro, A., Cruz, A., López-Rivadulla, M. (2012). Liquid Chromatography-Mass Spectrometry for the Determination of Antidepressants and Some of their Major Metabolites in Human Biological Matrices. In: Xu, Q., Madden, T. (eds) LC-MS in Drug Bioanalysis. Springer, Boston, MA. https://doi.org/10.1007/978-1-4614-3828-1_7
Download citation
DOI: https://doi.org/10.1007/978-1-4614-3828-1_7
Published:
Publisher Name: Springer, Boston, MA
Print ISBN: 978-1-4614-3827-4
Online ISBN: 978-1-4614-3828-1
eBook Packages: Chemistry and Materials ScienceChemistry and Material Science (R0)