
Abstract
A 17-year-old female presented with 7-month history of erythema and swelling of the upper left eyelid, associated with restriction of eyeball movement and diplopia (Fig. 35.1). The swelling was painless, with no discharge, and no fever. She had no medical illness and no history of ocular trauma or surgeries. Examination revealed a firm palpable mass in the superior-nasal quadrant of left eye.
Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Case
Clinical Data
A 17-year-old female presented with 7-month history of erythema and swelling of the upper left eyelid, associated with restriction of eyeball movement and diplopia (Fig. 35.1). The swelling was painless, with no discharge, and no fever. She had no medical illness and no history of ocular trauma or surgeries. Examination revealed a firm palpable mass in the superior nasal quadrant of left eye.

Young lady with ptosis, conjunctival chemosis and swelling of the upper left eyelid
Differential Diagnosis
-
Insect bite reaction.
-
Trauma.
-
Tumid lupus erythematosus.
-
Tumor:
-
Angiosarcoma.
-
Sebaceous adenocarcinoma.
-
Metastatic adenocarcinoma.
-
Lymphoma.
-
Biopsy Findings
Biopsy findings revealed diffuse monotonous infiltrate of small lymphocytes (Figs. 35.2, 35.3, and 35.4). Immuno-histochemistry showed positive CD20 (Fig. 35.5).

Low power showing diffuse monotonous infiltrate of small lymphocytes

Medium high power showing diffuse monotonous infiltrate of small lymphocytes

High power showing diffuse monotonous infiltrate of small lymphocytes

Positive CD20
Investigations
-
Lab Investigations:
-
CBC: Normal.
-
ESR: Normal.
-
B2 Microglobulin: Normal.
-
Lactate dehydrogenase (LDH): Normal.
-
-
Radiology Investigations:
-
Chest X ray: Normal.
-
Abdominal ultrasonography: Normal.
-
CT-scan: Large mass arising at the medial canthus, indenting the globe and displacing medial rectus. However, there was not eroding into bone or surrounding soft tissue (see Fig. 35.6).
Fig. 35.6 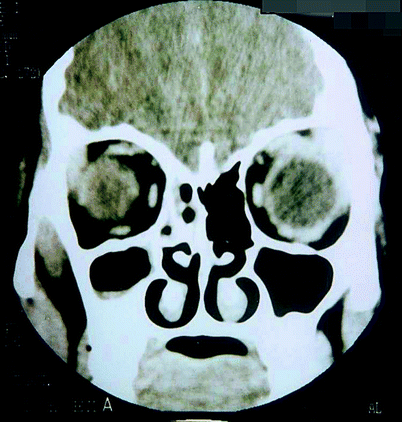
CT scan head; homogeneous isodense left orbital mass molding around the lateral ocular surface
-
-
Bone marrow biopsy: Normal.

Based on the Following Findings
-
Slowly enlarging unilateral mass arising from the eyelid, in proximity to the lacrimal gland.
-
CT scan finding of soft tissue mass.
-
Biopsy finding of diffuse monotonous infiltrate of small lymphocytes which are CD20 positive.
The Final Diagnosis was Primary Orbital Lymphoma (Small B-cell lymphoma type).
About the Diagnosis
Definition
-
Orbital lymphoma is a B-cell non Hodgkin lymphoma, and in most cases arises from Mucosa-Associated Lymphoid Tissue (MALT); i.e. Orbital Adnexal MALT Lymphoma (OAML).
-
It is unclear; however, if MALT exists normally in the conjunctiva of the eye, or whether it represents the sequelae of inflammation (thus the potential link to chlamydial infection).
-
Non-OAML tumors are of a variety of histologies, with diffuse large B-cell lymphoma being relatively common.
-
Classification of orbital lymphoma (see Fig. 35.7).
Fig. 35.7 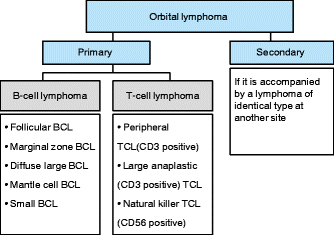
Classification of orbital lymphoma

Epidemiology
-
Lymphoma is the most common primary malignant orbital tumor in Asian countries like Japan and Korea as well as in Europe.
-
Orbital lymphomas account for only 2 % of all lymphomas, but constitute 5–15 % of all extranodal lymphomas and approximately 50 % of all primary orbital malignancies in adults.
-
The incidence of lymphoproliferative ocular diseases, especially malignant lymphoma, has increased over the years.
-
The possible infective etiology may explain the high incidence of orbital lymphomas.
-
Typically, patients are between 50 and 70 years of age. However, it may affect any age.
-
There is no sex predilection.
Pathogenesis and Etiology
-
Recent molecular studies demonstrating viral DNA in the ocular lymphoma cells suggest a role for infectious agents in the pathogenesis of intraocular lymphoma.
-
Chlamydia psittaci is associated with ocular adnexal mucosa-associated lymphoid tissue (MALT) lymphoma, and this association varies across different geographical areas.
Clinical Features
-
The commonest presentation of the disease is a slowly growing orbital mass that is generally asymptomatic.
-
Symptoms are usually secondary to pressure effects on the surrounding structures.
-
Depending on the location of the tumor, symptoms may include proptosis, ocular dysmotility, periorbital swelling, blurring of vision and chemosis.
-
The tumor is usually located the superior lateral quadrant, in proximity to the lacrimal gland.
-
In 25 % of patients the conjunctiva is involved in which case patients demonstrate a ‘salmon-red patch’ of a swollen conjunctiva.
-
Usually unilateral, however, bilateral involvement occurs in 10–15 % of cases.
-
Direct infiltration of the globe and/or optic nerve is rare, and vision is usually preserved.
-
The presence of cervical or preauricular lymphadenopathy, parotid gland swelling, or an abdominal mass can signify systemic disease.
Histological Features
-
Diffuse monotonous infiltrate of small lymphocytes.
-
CD20 positive (Pan B).
-
The most frequent histology of primary orbital lymphoma is indolent NHL such as extranodal marginal B-cell lymphoma of mucosa-associated lymphoid tissue (MALT).
-
Most patients with ocular adnexal lymphoma have stage-IE disease.
-
Histopathologically, it may be difficult to differentiate malignant lymphoma from a lymphoid hyperplasia. However:
-
Lymphomas show monoclonal staining and are predominantly B cells.
-
Lymphoid hyperplasia shows a mixture of B and T cells and is polyclonal.
-
Investigations
-
Radiological features:
-
CT scan:
-
CT scan of the orbits is a sensitive investigation that facilitates the diagnosis of orbital and adnexal lymphoma.
-
Well-defined, lobulated or nodular, homogeneous masses of relatively high density and sharp margins. The lesions mold themselves to preexisting structures without eroding the bone.
-
Frequently located in the upper outer quadrant, closely associated with the lacrimal gland.
-
Heterogeneous lesions with bony destruction are indicative of high-grade lymphomas.
-
Bilateral lesions are possible and can signify systemic disease.
-
Invasion of the globe or optic nerve is rare.
-
CT scans of the chest and abdomen are obtained to rule out retroperitoneal lymphoma.
-
-
Magnetic resonance imaging (MRI):
-
MRI of the orbits possesses good soft-tissue definition; however, it lacks the ability to delineate bone destruction, which can be seen in high-grade lymphomas.
-
MRI may miss conjunctival disease.
-
-
-
Other investigations:
-
Lumbar puncture is indicated to obtain cerebrospinal fluid (CSF) for cytology if the patient is believed to have CNS lymphoma.
-
Bone marrow aspiration to rule out marrow involvement. Bone marrow aspiration is used for staging systemic lymphomas.
-
Differential Diagnosis
It includes benign lymphoproliferative lesions, epithelial tumors, inflammatory and infectious lesions, among others:
-
Orbital rhabdomyosarcoma.
-
Uveal melanoma.
-
Lacrimal gland tumors.
-
Sebaceous adenocarcinoma of eyelids.
-
Orbital metastases (including disseminated lymphoma).
-
Angiosarcoma.
-
Leukemia cutis.
-
Idiopathic orbital inflammatory pseudotumor.
-
Orbital lymphoid hyperplasia.
-
Orbital sarcoidosis.
-
Thyroid associated orbitopathy.
-
Necrobiotic xanthogranuloma.
-
Superior vena cava syndrome.
-
Chronic dacryoadenitis.
-
Wegener granulomatosis.
Definite Diagnosis
-
The diagnosis of primary orbital lymphoma is made based on a combination of histopathologic, immunophenotypic, and molecular genetic studies.
Prognosis
-
The major prognostic criteria for ocular adnexal lymphomas include anatomic location of the tumor, stage of disease at first presentation, subtype of lymphoma, immunohistochemical markers determining factors such as the tumor growth rate, and the serum lactate dehydrogenase (LDH) level.
-
Marginal zone lymphoma has a significantly better prognosis than other low-grade tumors both in terms of disease progression and overall survival.
-
Systemic dissemination is only seen in 5–10 % of cases.
-
Orbital lymphoma can cause blindness in untreated or aggressive cases with severe proptosis leading to corneal complications or optic neuropathy.
-
Local irradiation can also cause reversible blindness due to cataract and irreversible blindness in cases of radiation-induced optic neuropathy and retinopathy.
Treatment
Treatment of lymphoma depends upon the specific type and staging of the disease at the time of diagnosis, as well as the age and general health of the patient. Options include:
-
Radiotherapy:
-
Orbital lymphomas are typically sensitive to local radiation.
-
Radiotherapy alone is a highly effective modality in the curative management of primary orbital lymphoma.
-
It is the therapeutic option for low grade lymphomas, with no systemic involvement.
-
Chemotherapy:
-
In patients with aggressive lymphomas and systemic involvement.
-
For patients with advanced disease, sequential chemo-radiation treatment is preferred.
-
-
-
Surgical excision:
-
It depends on the involved area.
-
Not recommended as an exclusive therapy because of the high rate of local relapses and difficulty to preserve the vital tissues of the eye.
-
Surgery is usually limited to biopsy.
-
-
Others:
-
Biologic therapy: Rituximab has recently been used for patients relapsing with lymphoma that expresses CD20 antigen.
-
Stem cell transplantation.
-
The recent identification of Chlamydia psittaci as a likely important causative factor in the increasing incidence of orbital lymphomas, has led to antibiotic therapy being used to not only reduce the size of the tumour, but in some cases result in remission.
-
Management of This Case
-
This case was referred to the oncology department for further management.
Message
-
Orbital lymphoma should be included in the differential diagnoses of chronic conjunctivitis not responding to standard treatment.
-
All patients with ocular lymphoma should have a complete workup to rule out systemic lymphoma.
Bibliography
Adam YG, Farr HW. Primary orbital tumors. Am J Surg. 1971;122:726–31.
Ahmed S, Shahid RK, Sison CP, Fuchs A, Mehrotra B. Orbital lymphomas: a clinicopathologic study of a rare disease. Am J Med Sci. 2006;331(2):79–83.
Astarita RW, Minckler D, Taylor CR, Levine A, Lukes RJ. Orbital and adnexal lymphomas: a multiparameter approach. Am J Clin Pathol. 1980;73:615–21.
Bardenstein DS. Intraocular lymphoma. Cancer Control. 1998;5(4):317–25.
Bennett CL, Putterman A, Britan J, Recant W, Shaprio CM, Karesh J, Kolokhe D. Staging and therapy of orbital lymphomas. Cancer. 1986;57:204–8.
Bessell EM, Henk JM, Wright JE, et al. Orbital and conjunctival lymphoma treatment and prognosis. Radiother Oncol. 1988;13:237–44.
Bhatia S, Paulino AC, Buatti JM, Mayr NA, Wen BC. Curative radiotherapy for primary orbital lymphoma. Int J Radiat Oncol Biol Phys. 2002;54(3):818–23.
Bolek TW, Moyses HM, Marcus Jr RB, et al. Radiotherapy in the management of orbital lymphoma. Int J Radiat Oncol Biol Phys. 1999;44:31–6.
Chanudet E, Zhou Y, Bacon CM, Wotherspoon AC, Muller-Hermelink HK, Adam P, et al. Chlamydia psittaci is variably associated with ocular adnexal MALT lymphoma in different geographical regions. J Pathol. 2006;209(3):344–51.
Esik O, Ikeda H, Mukai K, et al. A retrospective analysis of different modalities for treatment of primary orbital non-Hodgkins’s lymphomas. Radiother Oncol. 1996;38:13–8.
Hasegawa M, Kojima M, Shioya M, Tamaki Y, Saitoh J, Sakurai H, Kitamoto Y, Suzuki Y, Niibe H, Nakano T. Treatment results of radiotherapy for malignant lymphoma of the orbit and histopathologic review according to the WHO classification. Int J Radiat Oncol Biol Phys. 2003;57(1):172–6.
Jakobiec FA, Knowles DM. An overview of ocular adnexal lymphoid tumors. Trans Am Ophthalmol Soc. 1989;87:420–42; discussion 442–4.
Jenkins C, Rose GE, Bruno C, et al. Histological features of ocular adnexal lymphoma (REAL classification) and their association with patient morbidly and survival. Br Ophthalmol. 2000;84:907–13.
Jenkins C, Rose GE, Bunce C, Cree I, Norton A, Plowman PN, et al. Clinical features associated with survival of patients with lymphoma of the ocular adnexa. Eye. 2003;17(7):809–20.
Knowles DM, Jakobiec FA. Orbital lymphoid neoplasms: a clinicopathologic study of 60 patients. Cancer. 1980;46:576–89.
Margo CE, Mulla ZD. Malignant tumors of the orbit. Analysis of the Florida Cancer Registry. Ophthalmology. 1998;105(1):185–90.
Martinet S, Ozsahin M, Belkacemi Y, Landmann C, Poortmans P, Oehlere C, Scandolaro L, Krengli M, Maingon P, Miralbell R, et al. Outcome and prognostic factors in orbital lymphoma: a rare cancer network study on 90 consecutive patients treated with radiotherapy. Int J Radiat Oncol Biol Phys. 2003;55:892–8.
McKelvie PA, McNab A, Francis IC, Fox R, O’Day J. Ocular adnexal lymphoproliferative disease: a series of 73 cases. Clin Experiment Ophthalmol. 2001;29(6):387–93.
Miralbell R, Cella L, Weber D, et al. Optimizing radiotherapy of orbital and paraorbital tumors: intensity-modulated x-ray beams vs. Intensity-modulated proton beams. Int J Radiat Oncol Biol Phys. 2000;47:1111–9.
Nerad JA. Oculoplastic surgery. The requisites in ophthalmology. Philadelphia: Mosby; 2001. p. 348–86.
Nutting CM, Jenkins CD, Norton AJ, Ian C, Rose GE, Nicholas Plowman P. Primary orbital lymphoma. Hematol J. 2002;3:14–6.
Ohtsuka K, Hashimoto M, Suzuki Y. High incidence of orbital malignant lymphoma in Japanese patients. Am J Ophthalmol. 2004;138(5):881–2.
Pelloski CE, Wilder RB, Ha CS, Hess MA, Cabanillas FF, Cox JD. Clinical stage IEA–IIEA orbital lymphomas: outcomes in the era of modern staging and treatment. Radiother Oncol. 2001;59(2):145–51.
Shikishima K, Kawai K, Kitahara K. Pathological evaluation of orbital tumours in Japan: analysis of a large case series and 1379 cases reported in the Japanese literature. Clin Experiment Ophthalmol. 2006;34(3):239–44.
Vogiatzis KV. Lymphoid tumors of the orbit and ocular adnexa: a long-term follow-up. Ann Ophthalmol. 1984;16:1046–55.
Woog JJ, Kim YD, Yeatts RP, Kim S, Esmaeli B, Kikkawa D, et al. Natural killer/T-cell lymphoma with ocular and adnexal involvement. Ophthalmology. 2006;113(1):140–7.
Author information
Authors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer-Verlag London
About this chapter
Cite this chapter
El-Darouti, M.A. (2013). Non-resolving Chronic Eyelid Swelling. In: Challenging Cases in Dermatology. Springer, London. https://doi.org/10.1007/978-1-4471-4249-2_35
Download citation
DOI: https://doi.org/10.1007/978-1-4471-4249-2_35
Published:
Publisher Name: Springer, London
Print ISBN: 978-1-4471-4248-5
Online ISBN: 978-1-4471-4249-2
eBook Packages: MedicineMedicine (R0)